The increase in life expectancy and advancements in diagnostic procedures have led to a rise in malignant diseases, including various types of cancer [4]. The increase in life expectancy and advancements in diagnostic procedures have led to a rise in malignant diseases, including various types of cancer [4]. Consequently, the demand for dependable biomarkers and measurable parameters for assessing disease severity and therapy progress is also on the rise. To address these demands, research into disease progression, cellular mechanisms, and diagnostic options is just as crucial as the exploration of existing parameters and their predictive capabilities.
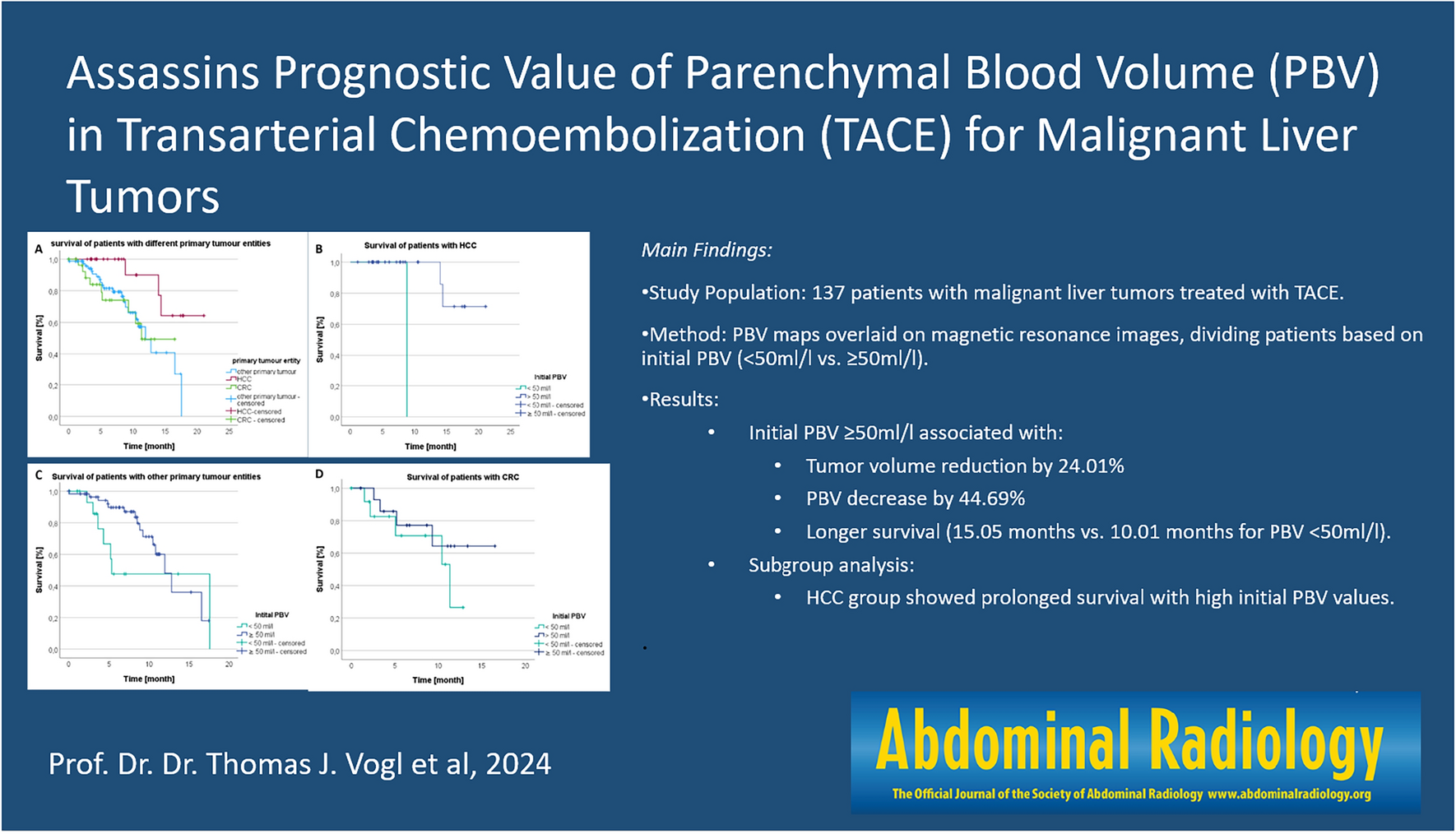
This study focused on patients who have HCC, CRC, or other primary tumor entities which were treated by TACE. The aim was to investigate whether a high initial PBV value is associated with a better treatment response and prolonged survival. Current gold standard in the assessment of tumor treatment success are the Response Evaluation Criteria in solid tumors, the so called RECIST criteria [3, 18]. These criteria are based on a 2-dimensional measurement of the tumor either by MRI or by spiral CT, where the longest diameter of solid tumor lesions is assessed and used as comparison value after the intervention. Hence, the tumor shrinkage is the only treatment parameter which is focused on [12] and the measurement is followed by an internationally valid classification in partial response (PR), complete response (CR), progressive disease (PR), and stable disease (SD) [18, 26]. This system makes it possible to evaluate the therapy progress in a standardized manner but also has some limitations based on the diversity of treatment options and cancer types [6]. The traditional RECIST criteria and thresholds of response were developed in order to evaluate the response to cytotoxic chemotherapeutic treatments and modern personalized medical approaches, which have other outcomes than tumor shrinkage, may not fit in this criteria [6]. Additionally, liver lesions and their treatment push the RECIST criteria to their limits based on the alterations of visibility and size of liver tumors after contrast injection depending on time, treatment and devascularization and also morphological changes of the lesions and scarring after focal therapy such as chemoembolization [6]. For patients with these lesions the criteria were adapted and the mRECIST (modified RECIST) criteria were established in 2010; these also address changes in the viable portion and tumor necrosis in order to evaluate the effectivity of focal therapies [6] and they are taken into account in the European guideline [7].
These criteria and specific diagnostic procedures open up the possibility to evaluate therapy success of TACE in HCC patients. One of those diagnostic methods is the C-arm CT which allows the visualization of the vascularity of the tumor tissues and thus, the measurement of the PBV.
Previous studies indicate that PBV measurements can assess TACE treatment success and that there is a correlation between a high initial PBV value and tumor response [9, 10, 15, 16, 24]. The results of the studies mentioned can be supported by comparable results of our study. We are able to show that there is a significantly higher decrease in PBV and tumor size after TACE with a high initial PBV, than with a low initial PBV. Similar results were reported by Vogl, Schäfer et al. who showed in a comparable study that in patients with a high initial PBV > 100 ml/l the percental decrease in PBV and tumor size is greater than with a low initial PBV < 50 ml/l [25]. The interesting question now is whether a high initial PBV value is associated with prolonged survival. To the best of the author's knowledge, there are currently no comparable studies on survival in relation to the initial PBV value. In our work, we refer to the study of Syha, who mentioned in his work that future survival analyzes should be performed in relation to the initial PBV value [17].
Our survival analysis results indicate that patients with high initial PBV survived significantly longer than patients with low initial PBV (p = 0.002)—on average nearly 5 months longer. However, the subgroup analysis of HCC, CRC, and patients with other primary tumors showed only that a higher initial PBV significantly increased the survival rate for HCC patients. For the other groups we found that the survival time for high and low PBV was not significantly different, which may be due to the small patient population. It is therefore advisable to expand the patient population in future studies and to conduct studies over a longer observational period. In future studies, expanding the patient population and conducting investigations over an extended observational period, while considering the diverse tumor burdens, will provide a more comprehensive understanding of the relationship between initial PBV values, treatment responses, and overall survival across various malignancies. With regard to the detailed analysis of differences between groups in terms of tumor biology or other baseline characteristics, we would like to emphasize that consideration of additional parameters such as ECOG status would have further reduced the size of our patient cohorts. Given the already limited sample size, smaller subgroups could have led to statistical uncertainty and limited interpretability.
Our aim was to include patients receiving TACE under as comparable conditions as possible in their respective groups. However, due to the complexity and time involved in the detailed inclusion of parameters like ECOG status, it was not feasible for us to make these allocations at this stage. This could represent a promising perspective for future studies specifically targeting the collection and analysis of such baseline characteristics. We acknowledge the importance of more comprehensive consideration of such factors and could view this as a suggestion for further research.
The results could indicate that a high PBV value was associated with prolonged survival and patients with HCC could possibly benefit from better prognosis estimation and potential extended lifetime with improved quality of life. Further investigations are necessary to evaluate the predictive power of the initial PBV in patients with malignant liver tumors before PBV can be used as a prognostic marker in diagnostics. In our discussion, we can underscore the significance of our findings regarding the elevated PBV in more vascular tumors in relation to overall survival. This outcome implies that tumors with a robust vascular supply may exhibit a heightened responsiveness to Transarterial Chemoembolization (TACE), potentially due to their greater dependence on arterial blood supply. Consequently, TACE might be more efficacious in treating such tumors, ultimately leading to prolonged survival.
Additionally, it would be pertinent to consider future investigations exploring whether analogous correlations hold true for alternative treatment modalities, such as radiation therapies or surgical resections. Such research endeavors could contribute to a comprehensive understanding of PBV's role as a prognostic factor across diverse therapeutic approaches and potentially assist in the optimal selection of treatment options tailored to specific tumor types.
Limitations of this approach to establish PBV as a biomarker were the time consuming preparation and analysis of PBV cards (it took an average of 15 min to create one PBV card), which is a disadvantage in the daily clinical life. All patients in this study received TACE on Syngo Artis Pheno CT (second generation) and/or Syngo Artis Zeego (first generation) and an impact on the results based on the type of device cannot be excluded. However, since all PBV cards, regardless of whether TACE was performed on 1st or 2nd generation devices, were created on the same workstation and all data were evaluated under the same conditions, this is unlikely. Furthermore, one should not disregard the heterogeneity of the patient collective. All patients with malignant liver disease and different primary tumors were included in this study. It must also be remembered that the primary tumors, underwent different pretreatments, some of which were not traceable. In some patients, the initial diagnosis was up to 20 years ago so that more detailed information on possible pretreatments were no longer accessible. An influence of these possible pretreatments on the results of our study is unlikely but cannot be ruled out completely. Additionally, theoretical considerations regarding potential effects of Lipiodol on the accurate calculation of PBV have been made. While Lipiodol is commonly used in transarterial chemoembolization (TACE) procedures and plays a crucial role in the delivery of therapeutic agents to the tumor site, its presence could introduce complexities in the accurate calculation of parenchymal blood volume (PBV). Theoretical considerations and potential interactions between Lipiodol and imaging techniques may impact the precision of PBV measurements. It is essential to acknowledge the possibility of such effects on PBV calculations and consider them as potential sources of error in our study. Future research could delve into the specific influences of Lipiodol on PBV determination to enhance the accuracy of these measurements in the context of TACE interventions. In our study, we ensured that all patients underwent TACE treatment to an angiographic endpoint of stasis or near stasis. Efforts were made to ensure that embolization was as effective as possible in achieving maximum tumor necrosis. However, lesser reductions in PBV cannot be ruled out and could be attributed to various factors. One possible explanation for lesser PBV reductions could be tumor biology. Tumors are heterogeneous, and their blood supply can vary significantly. Some tumors may have extensive and complexly branched blood supplies that may not be entirely reached by TACE treatment, leading to lesser PBV reductions even when embolization is performed to the best of our abilities. Furthermore, suboptimal techniques or individual anatomical differences among patients could play a role. The precise placement of embolic material and vascular architecture can vary, affecting the efficiency of embolization and the resulting PBV reduction. It's important to note that further research is needed to better understand these issues and the reasons for varying PBV reductions after TACE. This could help enhance the effectiveness of TACE treatment and improve the accuracy of predicting treatment responses.




留言 (0)