
記住我

A total of 207 patients hospitalized and diagnosed as newly diagnosed T2DM were from the Department of Endocrinology of Shaanxi Provincial People’s Hospital from April 2022 to September 2022 were collected, and 196 healthy people in the physical examination center of the hospital were collected as control group during the same period. All participants provided written informed consent. This investigation was approved by the Medical Ethics Committee of the School of Xi’an Medical College.
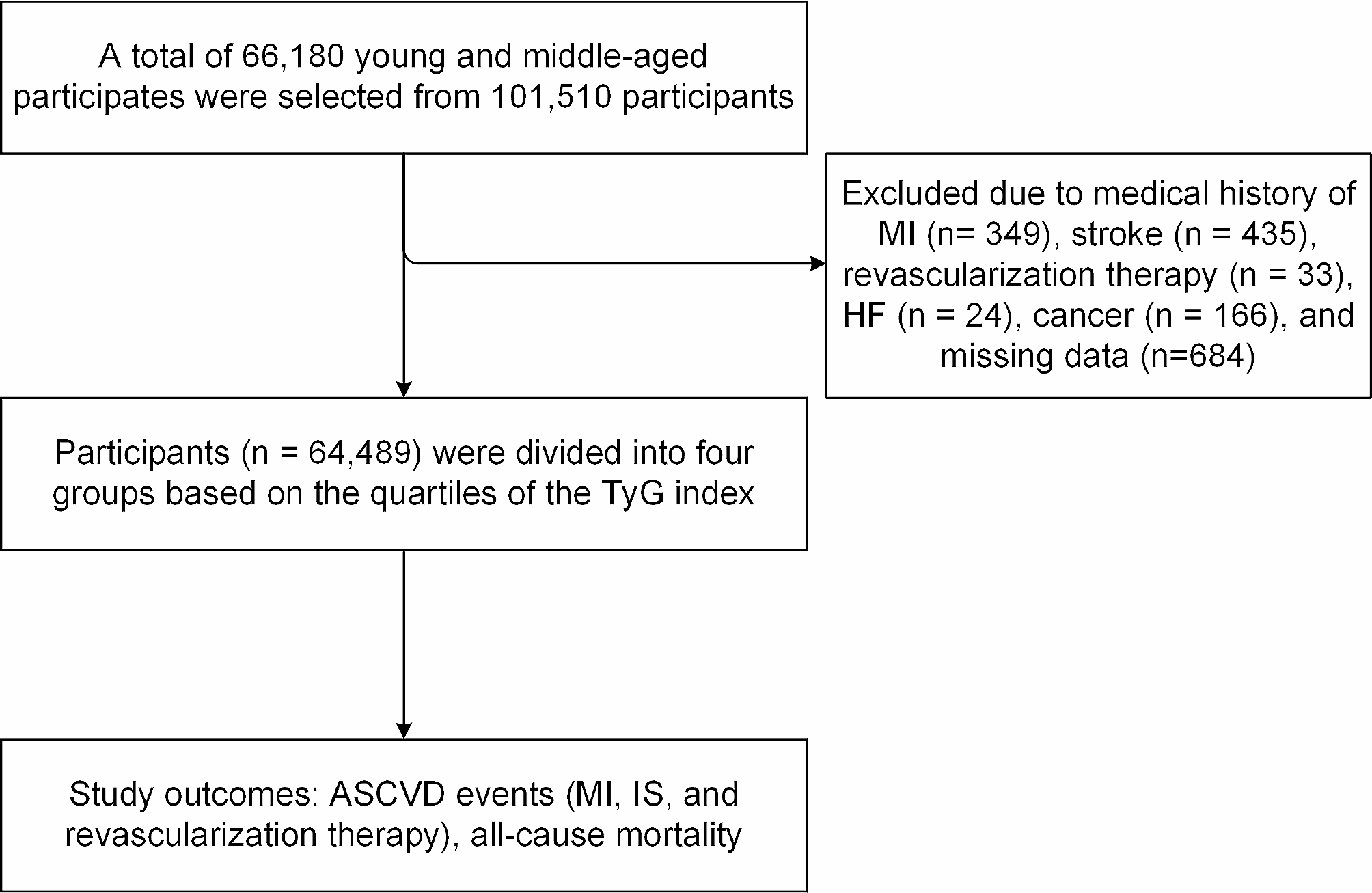
The inclusion criteria for patients were as follows: T2DM was defined according to the criteria of diagnosis and classification of diabetes proposed by WHO: diabetes symptoms (polydipsia, polyphagia, polyuria, and weight loss) with fasting blood glucose (FBG) ≥ 7.0 mol/L, random blood glucose ≥ 11.1 mol/L or oral glucose tolerance test (OGTT) 2-hour blood glucose ≥ 11.1 mol/L. The exclusion criteria for patients were as follows: Subjects with type 1, pregnancy, and other special types of diabetes, serious complications related to diabetes; hyperthyroidism, parathyroidectomy; osteoporosis, osteomalacia; acute and chronic infections, malignant tumors, rheumatic immune system diseases; hypertension, cerebrovascular diseases, hypercalcemia; severe liver and kidney function impairment were excluded. Overall, 403 patients were included in this study (Fig. 1).
Fig. 1
Flowchart of the study population. T2DM, type 2 diabetes mellitus; FGF23, fibroblast growth factor 23; α-klotho, α-membrane binding receptor Klotho; SD, standard deviation
Measurement of serum FGF23 and α-klotho levelsHuman FGF23 ELISA Kit (Beyotime) and Human α-klotho ELISA Kit (Solarbio) were used to detect the corresponding protein concentrations respectively, which were both based on double antibody sandwich enzyme-linked immunosorbent assay (ELISA), and serum samples were sent to Wuhan Xavier Biological Laboratory for detection, and the detailed steps are as follows;
Peripheral venous blood was taken after overnight fasting, and the serum samples were separated and frozen at − 80 °C for subsequent analysis. Serum samples were firstly diluted in dilution buffer without carrier protein and then added to 96-well microplates (100 µL). After the plate was sealed, the plates were incubated at room temperature. Afterwards, the wells were washed five times with buffer (400 µL) after containment, and each well was shielded with 300 µL of diluent. Afterwards, the plates were incubated at room temperature for at least 1 h and washed several times so that the antibody coating was completed. Then, Streptaviin-ORP (100 µL), a specific sandwich of the FGF23 or α-klotho immune complex, was added and incubated for 20 min in the dark. Finally, the substrate (100 µL) and termination solution (50 µL) were added, after which the mixture was fully mixed. The absorbance (OD) of each well was determined by a microplate reader (450 nm) for FGF23 and α-klotho, and the corresponding concentrations of FGF23 and α-klotho were calculated from the standard curve. The quality control results showed a variation coefficient of less than 10% in and between plates and a recovery rate of more than 95%.
Carotid artery-intimal thickness and carotid plaque measurementThe cervical vessels were examined by experienced physicians. All patients underwent color Doppler ultrasound examination with a Philips IU22 color Doppler ultrasound diagnostic instrument, and the linear array probe frequency was 7.0 MHz. Patients with carotid plaques were placed in the supine position, the supraclavicular fossa was used as the starting point for scanning, and the initial segment and bifurcation of the carotid artery were scanned. Once plaque was found, the local carotid artery was scanned repeatedly to evaluate the location, size, and number of carotid plaques. The above procedure was repeated to explore the condition of the bilateral carotid arteries of the patient. The diagnostic criteria for carotid atherosclerosis were formulated by the National Conference of Internal Medicine, and the results of carotid intima ultrasound examination were divided into three categories: (1) Normal blood vessels: CIMT was thin and smooth, as indicated by a double line sign, and CIMT thickness ≤ 0.9 mm; (2) CIMT thickening: Ultrasound revealed irregular CIMT echoes with thick light spots and an CIMT thickness of 0.9–1.2 mm; (3) Carotid plaque formation: Ultrasound showed that the vessel wall of the lesion site was elevated into the lumen, and the CIMT thickness at the lesion site was ≥ 1.2 mm or 1.5 times greater than that at the adjacent site.
Definition of covariatesThe basic information (name, age, BMI, blood pressure, smoking status, and duration of diabetes) of the patients was collected. BMI was calculated as weight (kg) divided by height squared (m2). Smoking status is defined as smoking and never smoking, while smoking includes current smoking or former smoked. Biochemical indicators, including fasting blood glucose (FBG), glycosylated hemoglobin (HbA1c), systolic blood pressure (SBP), diastolic blood pressure (DBP), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c), blood urea nitrogen (BUN), serum creatinine (Scr), cystatin C (Cys-C) and 25-hydroxyvitamin D3 (25-(OH)D3), were detected in blood and urine samples collected from the Department of Clinical Laboratory of Shaanxi Provincial People’s Hospital. And eGFR was calculated based on the serum cystatin C (Cys-C) concentration and creatinine concentration according to the combined creatinine–cystatin C equation, which is useful as a confirmatory test for chronic kidney disease [30].
Statistical analysisSince the distributions of FGF23 and α-klotho levels were both skewed, these two variables were log10-transformed to obtain normal distributions. Participants were then divided into 3 groups based on tertile cut-off values for serum FGF23 and α-klotho levels. Baseline information was expressed as the mean and standard deviation (SD) or median and interquartile ranges (IQRs) for continuous variables and the number (percentage) of categorical variables based on tertiles of serum FGF23 and α-klotho.
Using multiple logistic regression models, we estimated odds ratios (ORs) with 95% confidence intervals (CIs) for serum FGF23, α-klotho levels and FGF23/α-klotho ratio in patients with T2DM and carotid atherosclerosis and per unit increase in log10-transformed FGF23, α-klotho levels and FGF23/α-klotho ratio. Age, sex, smoking status (smoking and never smoking), BMI, SBP, DBP, TC, TG, HDL-c, LDL-c, and eGFR were used as confounders in this analysis. We excluded 21 samples with detection concentrations of FGF23 and α-klotho exceeded the median plus or minus 1.5 standard deviations, and a total of 18 subjects had missing covariate data and were estimated using multiple interpolation. In addition, we conducted spline analyses to explore the dose‒response relationships of serum FGF23, α-klotho levels and FGF23/α-klotho ratio with T2DM, T2DM combined with CIMT and T2DM combined with carotid atherosclerosis, with 3 knots placed at the 5th, 50th, and 95th percentiles and the reference value set at the 10th percentile of serum FGF23, α-klotho levels and FGF23/α-klotho ratio.
All analyses were completed with R (version 3.6.1, R Foundation for Statistical Computing). Two-sided P values less than 0.05 were considered to indicate statistical significance.
留言 (0)