
記住我



Twenty-two persons with LLA, recruited in the “Centre Médico-Chirurgical de Réadaptation des Massues - Croix-Rouge Française” (Lyon, France), voluntarily participated in the present study that was approved by the local ethics committee (2015-A00573-46). Due to personal relocation, one participant did not complete the study after moving to another region, and two participants quit voluntarily after losing interest in the experiment. The characteristics of the 19 participants who fully completed the protocol and were included in the statistical analysis are reported in Table 1. Inclusion criteria were the following: (i) being included in the rehabilitation program of the “Centre Médico-Chirurgical de Réadaptation des Massues” (ii) being aged between 18 and 80 years old, (iii) having, during the last 20 days, suffered from an unilateral transfemoral or transtibial amputation of vascular, trauma, infectious or cancerous origin, (iv) having a score above 24/30 on the Mini-Mental State Examination [29], and (v) currently not participating to any other research protocol. Exclusion criteria included the presence of (i) neurologic and/or psychiatric disorders, (ii) motor dysfunctions unrelated to the present amputation, and (iii) guardianship, as well as any other administrative or legal right deprivation measure. After the validation of participation by the physician, participants signed an informed consent form. All participants arrived at the rehabilitation center maximum two weeks after their amputation and were included in the study within the week upon their arrival at the rehabilitation center (Fig. 1). For medical facilitation, participants were continuously assigned in a predetermined group depending the order of inclusion (the Control group was first completed, before the MI group, to avoid any contamination across the participants). The MI and control groups entailed nine and ten participants, respectively, and the analysis strategy was “intention to treat”. The Trend statement complementing the widely adopted consolidated standards of reporting trials was used in this study [30].
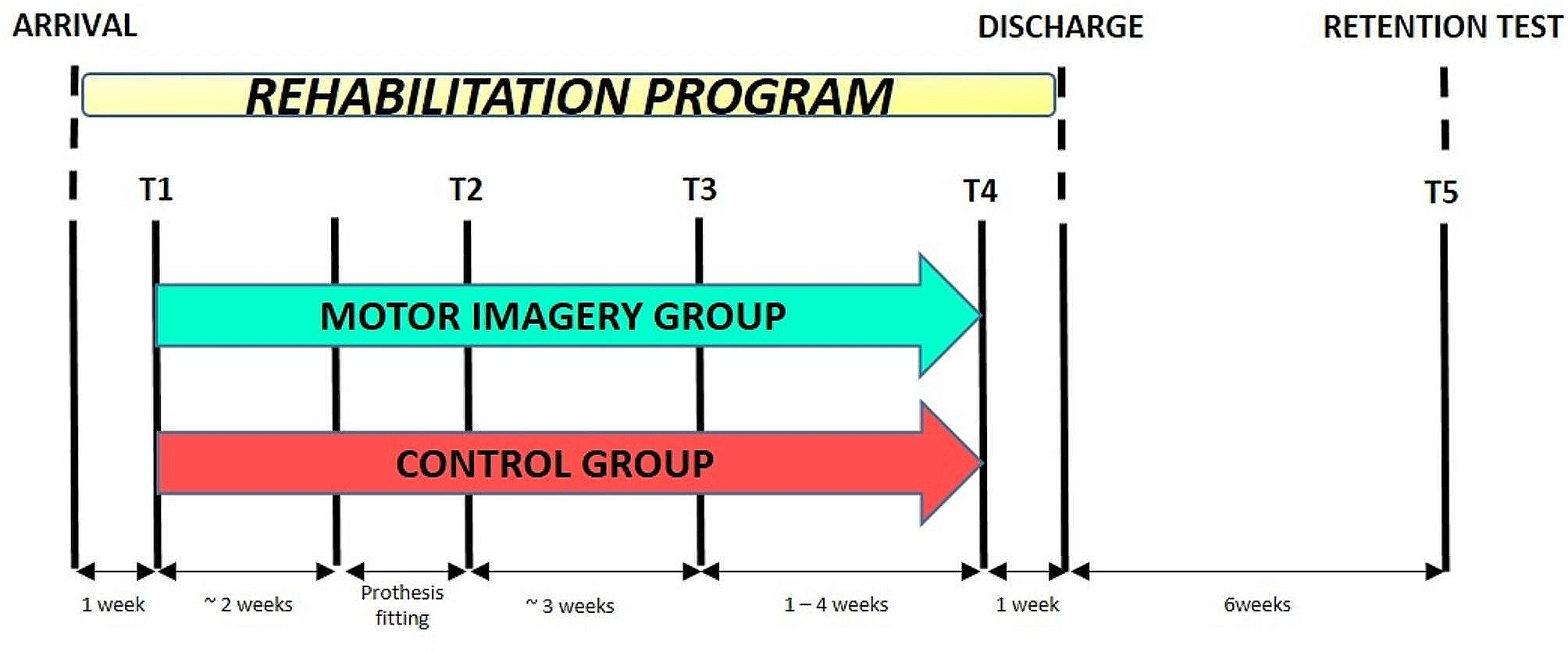
Fig. 1
Experimental design showing the chronology of assessments. One week after arrival at the rehabilitation center (T1), participants were assigned to the MI or control group and started to perform MI or the control task concomitantly with physical therapy, up to one week preceding the end of the rehabilitation program (T4). Participants were tested at their arrival to the center (T1), after prosthesis fitting once they could walk with it safely (T2), at an equivalent time of rehabilitation (T3), at an equivalent functional rehabilitation level before leaving the center (T4), and six weeks after the end of the rehabilitation program (T5)
Table 1 Participants’ characteristicsExperimental designRehabilitation programAfter their arrival at the rehabilitation center, participants started the rehabilitation program under the supervision of physio- and occupational therapists, five times per week, until they reached independent steady gait and functional balance. As a first step, they received stump care and followed the pre-prosthetic rehabilitation program, mainly composed of static balance exercises. During this early phase, only a small amount of the rehabilitation work was organized around dynamic exercises, mainly consisting in unipodal walking between parallel bars. The same program was scheduled in the two groups, with a daily time of training of about 30 min. After healing was considered satisfactory by the medical team, participants were fitted with a prosthesis. Prosthetic rehabilitation program consisted in 10 min of static exercises and a series of dynamic balance and walking-related exercises per day, depending on the fatigue and pain level of the participant. While the time window usually recommended by the medical team during this period ranges from 30 min to 2 h, we restricted the variability in the duration of these exercises to avoid significant diversity among patients (30 to 45 min).
Motor imagery practiceThroughout the course of physical therapy, participants from the MI group followed a MI intervention. During break times of locomotor training, they were asked to mentally rehearse the movements they just physically performed, using both visual and kinesthetic modalities of MI, from a first-person perspective. Participants’ ability to perform visual and kinesthetic MI was measured after each trial using a 5-point Likert scale graduated from 1 (no image/no sensation) to 5 (image as clear as seeing/sensation as intense as when physically performing the action). To promote MI accuracy, MI trials were scheduled right after physical practice [31, 32]. Each MI trial consisted in repeating for 2 min the movements previously performed. Practically, during the pre-prosthetic phase, MI training included the mental rehearsal of hip flexion/extension movements alternated with unilateral walking between the parallel bars, with an emphasis on strong and safe ground contact with the intact limb. While it is possible to imagine a motor sequence that is not yet physically feasible, based on the memory of these movements, the decision not to perform such imagery was related to the fact that amputees do not recover their normal locomotor function. Functional recovery and restoration of locomotion abilities will depend on the integration of a prosthesis. It was therefore critical for gait imagery to incorporate the use of this individualized prosthetic device before considering its fine-tuned use. During the prosthetic phase, additional MI trials of the Timed Up and Go test (TUG) [33] were also performed. Participants completed 5 trials per day, so a total of 10 min of MI, 5 days per week. Participants from the control group performed a neutral cognitive task (crossword puzzles and Sudoku games) during an equivalent amount of time, and in the presence of the same physiotherapist.
MeasuresA total of five tests were scheduled (Fig. 1). A first test (T1) was programmed one week after participants’ arrival to the rehabilitation center. A second test (T2) was scheduled after they were fitted with the prosthesis and able to walk continuously during 10 min (including short rest breaks). Due to recovery time variability between participants, a third evaluation (T3) was planned 3 weeks later, to provide “time equivalent” data. As the standardization of the therapeutic patient management was not possible, the program evolution remained somewhat patient-dependent, most especially regarding decisions related to the temporal frame. Consequently, to avoid significant disparities among patients, we established a comparison at T3 based on a similar treatment duration, allowing a comparison for an equivalent duration of rehabilitation. Then, to extend data analysis over a longer period, we conducted an assessment at equivalent functional levels prior to clinic discharge (T4). This choice of two complementary evaluations ensured a more detailed and comprehensive comparison of recovery effects in patients, allowing for an assessment of functional recovery dynamics, i.e. satisfying levels of gait speed and balance (standing up, standing, and sitting without external assistance). Finally, a retention test (T5) was scheduled 6 weeks post-departure from the rehabilitation center. The medical assessors who determined the end-points, as well as the therapists performing the evaluation measures, were blinded and did not have information about whether participants were assigned in the control or MI group.
Motor imagery abilityTo assess participant’s ability to imagine movements, MI vividness and temporal accuracy were measured at T1. MI vividness was assessed through an adapted version of the Kinesthetic and Visual Imagery Questionnaire (KVIQ [34]) focusing on five movements involving lower limbs (see [22] for greater details). For each imagined movement, participants physically performed the sequence beforehand. They scored from 1 (no image/no sensation) to 5 (image as clear as seeing/sensation as intense as when physically performing the action) the clarity/intensity of the images/sensations perceived during MI. The temporal accuracy of MI was assessed with the chronometric measure of a single-joint movement [35]. The time required to actually and mentally perform five consecutive hip abductions was recorded for both intact and amputated sides, with an electronic digital stopwatch (Extech Instruments, model 365,515, USA). The ratio between mean MI and actual execution times was then calculated. The closer the ratio to 1, the better the temporal accuracy of MI.
A manipulation check was scheduled each week to control adherence of the participants to the imagery guidelines, and the quality of their imagery experience. We gathered informal information participants was likely to share about his/her imagery experience, and further asked them to rate the quality of their imagery and describe any difficulty they may have experienced. Very few patients sporadically reported some trouble during the imagery exercises, hence supporting that they overall quite easily followed the instructions as intended.
Motor recoveryAfter prosthesis fitting, motor recovery was assessed with two locomotor functional tasks (at T2, T3, T4 and T5): (i) the 10 m walking task [36] which required to walk a 10 m distance at a safe speed, and (ii) the TUG task where participants get up from a chair, walk 3 m, turned around, came back to the chair, turned around and sat down. During all evaluations, participants could use one or both of their crutches or even a walker, if required for safety reasons. A functional level score and the estimated force of the amputated limb were further collected. These two tests are part of a standardized clinical procedure in patient’s care, and thus frequently used by therapists. The functional score was rated by the medical assessors at T2 and T4. Such score allows healthcare professionals to categorize the level of assistance required for walking, ranging from complete dependence on a wheelchair to no needed assistance. Practically, a 6-level scale here reflected the required assistance for walking (necessity of using a wheelchair, the parallel bars, a walker, a rollator, two walking canes, one walking cane, or no needed assistance). It then aids in treatment planning, and ensures a consistent understanding of patient’s mobility, promoting effective care and support tailored to individual needs. The force of the amputated limb was also measured at T2 and T4, using a 5-level of pressure scale exerted by the physiotherapist. This scale helped to quantify the force provided by the patients against a constant pressure exerted on the residual limb by the therapist. Beside the measurement of the force per se, this force provided relevant information to the therapists to tailor the prosthetic device to individual needs and reduce discomfort. Finally, the time of hospitalization was collected to compare delays separating the different time measurements.
PainAlthough this experiment was specifically designed to assess the benefits of MI on functional recovery, the potential influence of the intervention on phantom limb pain was also measured. During each of the five tests, participants were asked to rate on an analog scale, ranging from 0 (no pain at all) to 100 (worst pain possible), the intensity of the phantom limb pain they experienced during the last 24 h.
Group data analysisThe durations of the locomotor-related tasks (10 m walking and TUG) at the different evaluations (T2 to T5), as well as the individual time of hospitalization in days at each evaluation (T2 to T5), were the primary dependent variables quantifying sensorimotor recovery. As secondary outcomes, we also analyzed the clinical assessments of force on the amputated limb on a 5-point Likert-type scale at T2 and T4, as well as pain scores at T1-T5, as subjective dependent variables. KVIQ score and MIRATIO were the dependent variables indexing MI ability. Since MI ability was not measured in the Control group, who did not perform MI training after receiving their prosthesis, we conducted a univariate analysis of KVIQ scores and MIRATIO.
We used R [37] and nlme [38] to run a linear mixed effects analysis, with by-subject random intercepts, of the dependent variables quantifying motor performance during the prosthetic phase (TUG and walking test durations). We built a random-regression coefficient ANCOVA model testing for the fixed effects of GROUP (MI, Control) and TEST (T1-T5), with interaction term. To account for baseline differences, we included performance at T2 as the covariate. Due to deviations from normality (visual inspection of Q-Q plots), we ran a non-parametric analysis of hospitalization time data using the ARTool [39] package. Aligned-Rank Transformation (ART) consists in a preliminary step of data alignment based on the mean estimates of main/interaction effects of a given factorial model, followed by rank assignment [40]. We applied the ART to both linear and linear mixed effects models (with by-subjects random intercept accounting for repeated measures), using the fixed effects of GROUP (MI, Control) and TEST (T1-T5), with interaction term. We obtained partial coefficients of determination (η2P) as measures of effect sizes, using the ad hoc procedure for linear mixed effects models implemented from the effectsizes package [41]. As post-hoc investigations, we used contrast tests of marginal means estimates implemented from the multcomp package [42]. The proportion of participants’ distribution across 6 progressive impairment walking categories at T4, corresponding to the end of hospitalization, was compared between MI and Control groups using a Chi-squared independence test. The statistical significance threshold was set up for a type 1 error rate of 5%. Holm’s sequential corrections for multiple comparisons were applied to control the false discovery rate [43].
留言 (0)