Peripheral neuropathy is increasingly being recognized as a common problem in PD patients. Prolonged L-dopa exposure may contribute to neuropathy via increased homocysteine and methylmalonic acid levels. However, PD patients without L-dopa exposure may have underlying genetic mutations or separate mitochondrial disorders driving their neuropathy. Vitamin B12 and cobalamin deficiencies have also been implicated as causal factors, as has accumulation of phosphorylated α-synuclein [3].
Aiming to investigate PN in PD patients, we designed the current study including both drug-naive patients and patients receiving dopaminergic drugs. We tried to exclude patients with comorbid disorders that could also cause neuropathy. Nerve conduction studies were used to assess large fiber neuropathy. Autonomic function tests were utilized to evaluate autonomic and small fiber neuropathy, as our center lacks experience with skin biopsy which is used to assess intraepidermal nerve fiber density, quantitative sudomotor axon reflex testing or laser evoked potentials.
Screening for neuropathy using the TCNS revealed that 15% of drug-naive patients had mild neuropathy, while 45% of patients receiving dopaminergic drugs had mild to moderate neuropathy. This result was like Corrà et al. [2], who reported PN in about 40% of PD patients, with the majority being small fiber neuropathy. Another study by Grambalová et al. [20] conducted electromyography examinations on 49 patients with PD with asymptomatic polyneuropathy and 40 controls. They found that polyneuropathy was significantly higher in patients with PD compared to controls (45% versus 2%). However, they did not find a relationship in the PD group according to long-term L-dopa usage, PD duration, or age.
A previous study by Notermans and colleagues [21] looked at the relationship between L-dopa therapy and PN prevalence in PD patients. They found PN in only 12.1% of L-dopa-naive patients, compared to 36.1% of L-dopa-treated patients. This significant increase in PN prevalence with L-dopa treatment suggests that dopaminergic therapy and disease progression both play an important role in the development of PN in PD patients.
Ramachandran and colleagues [4] conducted their study on a cohort of early-stage PD patients. They found PN in 49 patients (31.8%), with large fiber neuropathy present in 18.2% and small fiber neuropathy in 30.5%. There was an overlap of large and small fiber neuropathy in 16.9% of the patients.
In the current study, analysis of nerve conduction studies showed significant impairment of sensory fibers in the median, ulnar, radial, and sural nerves of PD patients compared to healthy subjects. This agrees with findings from Ramachandran and colleagues [4], who reported mild axonal sensory neuropathy in 53% of patients, severe sensory neuropathy in 29%, and sensorimotor neuropathy in 18%. Our results confirm previous findings that large-fiber polyneuropathy in PD is typically distal and symmetrical, predominantly axonal, sensory-motor in nature, and affects sensory fibers primarily [22].
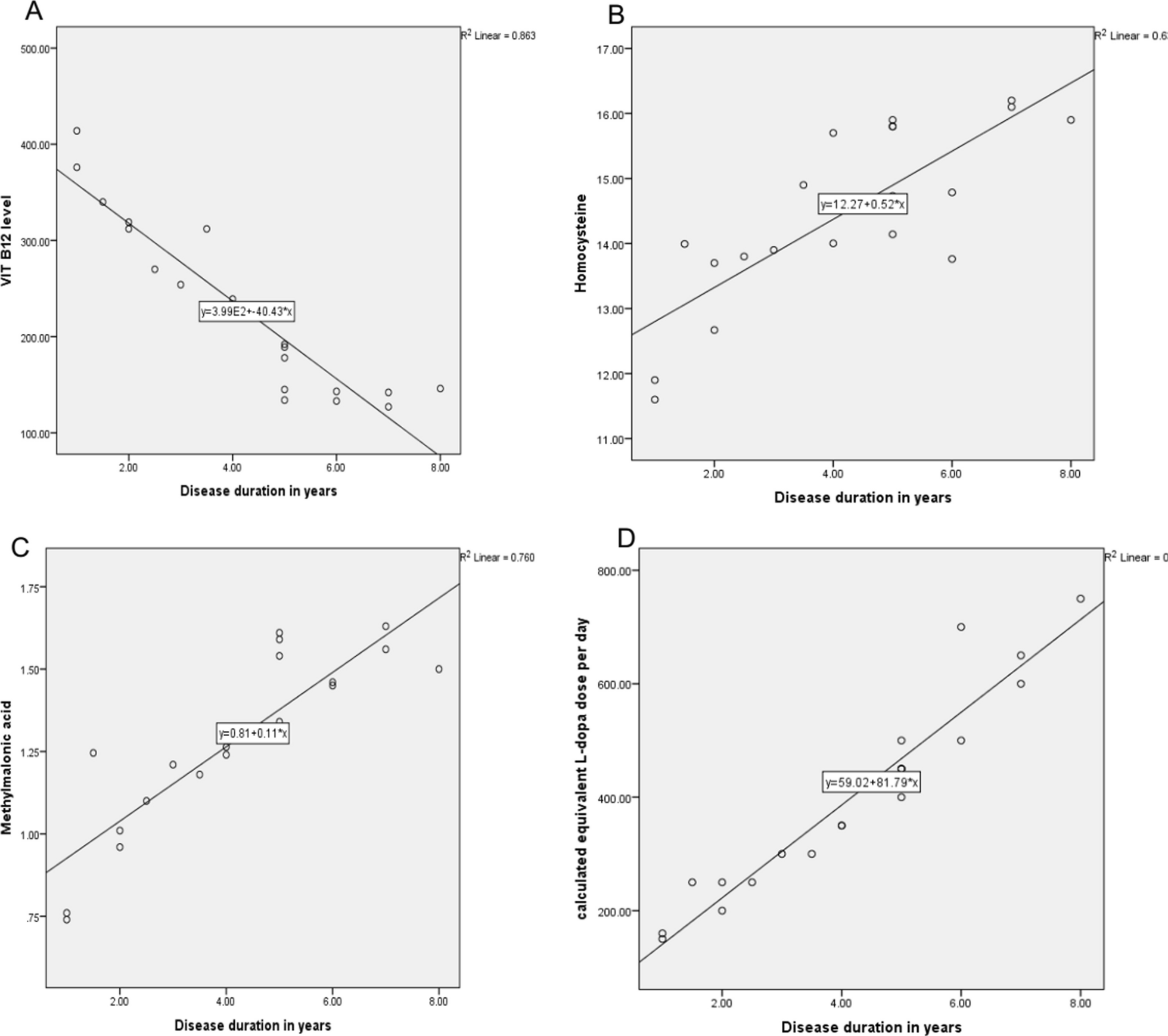
Our results revealed that serum vitamin B12 levels were significantly lower in PD patients on dopaminergic drugs compared to both drug-naive patients and healthy subjects. In contrast, PD patients on dopaminergic drugs had significantly higher serum homocysteine and methylmalonic acid levels compared to the other groups.
Low levels of serum vitamin B12 have been increasingly associated with PN in patients with PD. A major study by Ceravolo and colleagues [23] found significantly decreased serum B12 levels in patients with PD with neuropathy compared to those without neuropathy and healthy controls. This effect was independent of levodopa therapy duration.
The mechanisms linking B12 deficiency and neuropathy in PD are not fully elucidated. However, it is known that B12 is an essential cofactor in single-carbon metabolism, and deficiency can lead to accumulation of neurotoxic intermediates like methylmalonic acid and homocysteine [3]. Elevated homocysteine has been significantly associated with PN in patients with PD. Hyperhomocysteinemia triggers the development and progression of PD by different mechanisms, including oxidative stress, mitochondrial dysfunction, apoptosis, and endothelial dysfunction [24]. Particularly, the progression of PD is linked with high inflammatory changes and systemic inflammatory disorders [25].
To evaluate small fiber neuropathy in early PD, Podgorny and colleagues [26] studied a group of newly diagnosed patients with PD with no or minimal previous exposure to levodopa. Using corneal confocal microscopy, they found abnormalities in the small corneal nerve fibers of patients with PD compared to controls. This suggests small fiber neuropathy may be present in PD prior to initiation of levodopa treatment. Our findings support these results, as we have also reported autonomic dysfunction in both drug-naïve and patients with PD on dopaminergic medication. Together, these results indicate that small fiber neuropathy and autonomic abnormalities may manifest in early PD, even before dopaminergic treatment.
In agreement with our findings, another longitudinal study in PD patients found associations between abnormalities in cardiac electrical activity and PD progression. Specifically, they reported that prolonged QT intervals and decreased heart rate variability were associated with greater PD severity and progression over 5 years. These changes in cardiac autonomic function may serve as useful biomarkers to monitor PD progression [27]. Our results align with this study, demonstrating that autonomic dysfunction, evidenced by altered cardiac activity, correlates with disease status in PD. Cardiac autonomic abnormalities may prove to be helpful objective measures to track PD severity and progression over time.
Further supporting our findings, a recently published study reported that assessment of small autonomic nerve fiber function using the quantitative pilomotor axon-reflex test could serve as a noninvasive tool for detecting PD-related autonomic neuropathy and monitoring disease progression [28]. Our findings align with this study, and together they suggest that measures of small fiber autonomic function may have diagnostic and prognostic value as accessible biomarkers in PD.
Autonomic neuropathology in patients with PD includes both neuronal damage and α-synuclein pathology affecting the central and peripheral autonomic nervous systems, as we summarized. Peripheral α-synuclein changes can even predate central pathology [5]. Additionally, Brumberg and colleagues [29] suggested that alpha-synuclein contributes to peripheral neurodegeneration and impairs cardiac sympathetic neurons in patients with synucleinopathies like PD. Their findings further support a role for α-synuclein-mediated peripheral autonomic pathology in PD, including early cardiac sympathetic denervation.
While PD has historically been characterized as a central nervous system neurodegenerative disorder, accumulating research now recognizes intrinsic involvement of the peripheral and autonomic nervous systems. Consequently, quantitative indices of parasympathetic and sympathetic nervous system function may have utility as accessible biomarkers for early diagnosis and tracking progression of PD [30].
The main challenge in determining the intrinsic role of PD in PN is that most patients start treatment right after diagnosis. Therefore, epidemiological data have only been gathered on small groups of early stage, drug-naive PD patients [31]. No large prospective case–control study has been conducted to compare the prevalence of PN in untreated PD patients versus healthy controls. This point favors our study, as we enrolled drug-naive patients, despite the limitations of our methodology.
The study has several limitations that should be addressed in future research. Firstly, the relatively small sample size of 40 patients with PD and 20 controls warrants larger studies to confirm the findings with greater statistical power. Additionally, the cross-sectional design provides only a snapshot of the participants’ condition, whereas longitudinal studies tracking PN over time would give more insight into its evolution with disease progression. Furthermore, the nerve conduction studies employed in this research assess only large fibers, while incorporating assessments of small fibers, such as skin biopsy, could provide a more comprehensive understanding of the PN in PD.





留言 (0)