
記住我




This case series focuses on three instances of anti-LGI1 encephalitis in three patients in their 3rd to 5th decades, each displaying diverse symptoms, such as subacute onset facio-brachial dystonic seizures (FBDS), behavioural changes, and, in one case, hyperhidrosis.
Case 1 was a 21-year-old female with a sudden onset of FBDS. She presented to the emergency department after two days of FBDS and repetitive hyperhidrosis in both hands, arms and back. Case 2 was a 46-year-old male who had FBDS with altered mood and progressive cognitive decline over eight weeks. Case 3 was a 36-year-old male with FBDS, forgetfulness, anger episodes, psychosis, and heightened irritability for the last four weeks. All three patients experienced 50 to 100 FBDS episodes per day. EEG did not show any epileptiform discharges in any of the cases. MRI brain scans of patients 1 and 2 appeared normal, and patient 3 displayed bilateral FLAIR/T2 basal ganglia hyperintensities on their MRI brain. They underwent PET (Positron Emission Tomography) Scans on a GE Discovery 710 PET/CT machine (General Electronics, Wisconsin, USA) preceded by intravenous injection of an average of 112 MBq of F18 Flurodeoxy Glucose (F18 FDG). The median time between the MRI Scan and PET imaging was three days. The images reconstructed using an iterative reconstruction algorithm and studied in transaxial, coronal, and sagittal views revealed significant hypermetabolism in the Basal Ganglia (BG)and Mesial temporal region (Patient 1 and 3) and thalamus (patient 1) (Figs. 1, 2, 3) while we awaited the antibody reports.
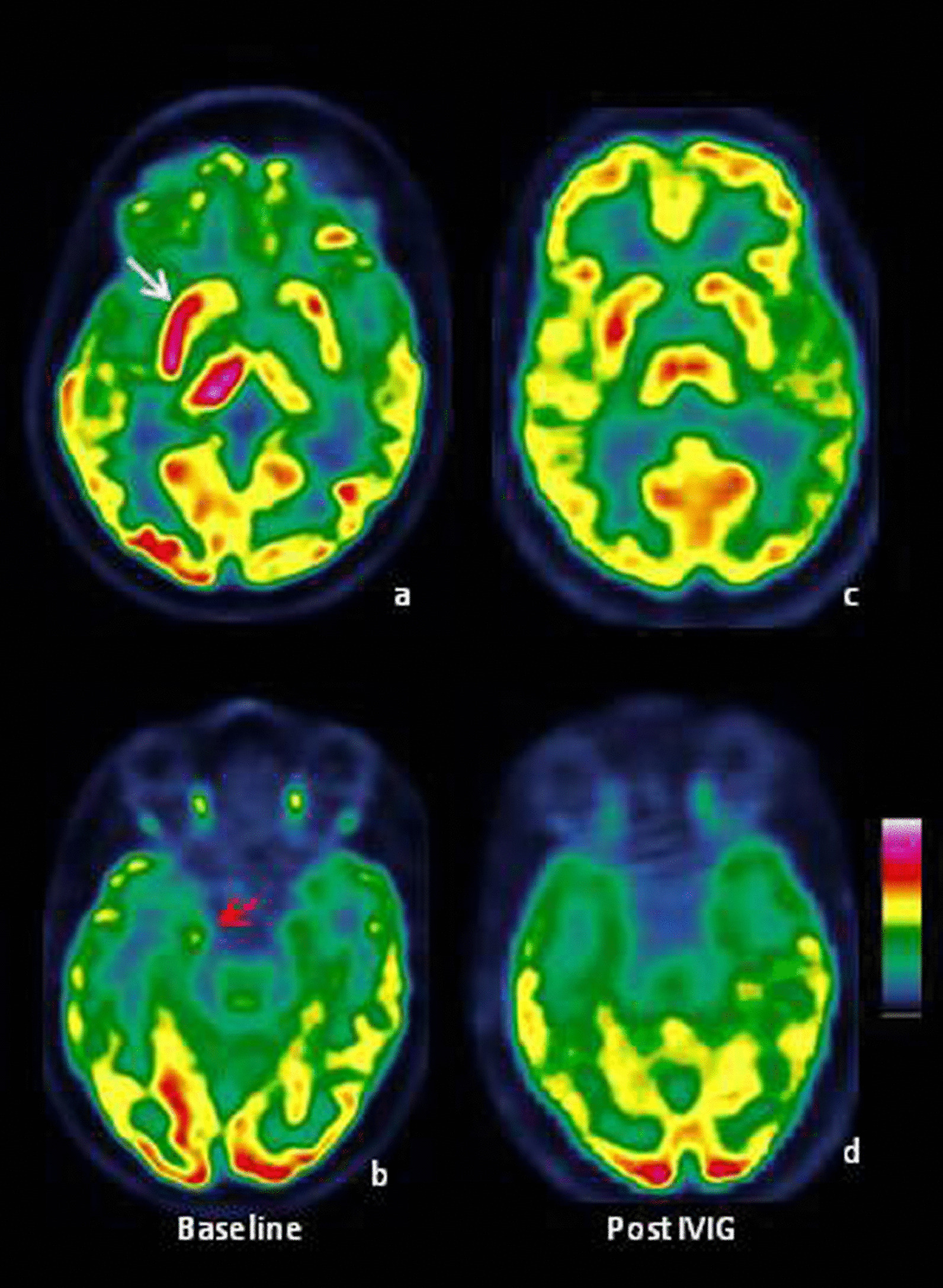
Fig. 1
Case 1 A: F-18 FDG PET images of the brain showed increased FDG uptake in the right caudate, putamen, and thalamus in transaxial view (a) (white arrow) and right mesial temporal region in coronal (b) (red arrow). A repeat scan after 6 months suggests normalisation of FDG uptake (c and d)
Fig. 2
Case 2, R: F-18 FDG PET images of the brain suggested increased FDG uptake in the left caudate and putamen (a: PET/CT) (b: PET) (red arrow) in the transaxial image. A repeat scan three days after IVIG showed a reduction in metabolism in the same region (c and d) (yellow arrow)
Fig. 3
Case 3, H: F-18 FDG PET images in transaxial view showed increased uptake (hypermetabolism) in bilateral caudate and putamen (a: white arrow), midbrain (b: red arrow) and bilateral mesial temporal regions in (c) and (d: coronal view) (hollow arrowhead). A repeat scan image was unavailable in her case, but it showed a reduced hypermetabolism in that region
Without delay, the three patients received pulse therapy of 1-g intravenous methylprednisolone for 5 days, followed by weight-based Intravenous immunoglobulin (IVIG). All three patients were found to be anti-LGI-1 positive in serum. Subsequently, they were maintained on weight-based oral prednisolone for 6–8 months and/or immunotherapy. In all three cases, serial PET showed resolution and/or reduction in the FDG uptake after therapy, with complete resolution observed in patient 1, who had the relatively rare manifestation [1, 2] of autonomic symptoms in LGI1 encephalitis. Patients 2 and 3 had a reduction of uptake compared to their initial PET scans. This may be because they were treated early before their functional damage became structural and irreversible. These patients have been symptom-free for three years and no longer require anti-seizure medications or immunotherapy. However, they are on a follow-up radar, and if any old or new symptoms occur, the possibility of re-evaluation and treatment has been communicated to them.
The closest differential includes anti-NMDA receptor encephalitis, showing the most pronounced discrepancy between PET abnormality and MRI findings. This includes PET findings of a wedge-shaped zone of occipital hypometabolism and involvement of Mesial temporal limbic (MTL) structures. MTL structure involvement is less commonly seen in NMDA receptor encephalitis than in Limbic encephalitis [3, 4]. The clinical picture usually helps to differentiate between specific tumour associations (for example—teratoma) in NMDA encephalitis and LGI1-specific signs like FBDS. An LGI1 encephalitis systematic review [5] has shown abnormal metabolism in various brain areas, including medial temporal, hippocampus, cerebellum, and BG, or even isolated BG uptake. More importantly, LGI1 antibodies have been detected in the pallidum, hippocampus, and BG through western blot analysis of brain tissue [6]. Graus and colleagues [7] have laid down the importance of PET scans in diagnosing Anti LGI1 AE and mentioned how hypermetabolism of medial temporal lobes on PET scans can be considered diagnostic. In our series, Case 1 had unilateral mesial temporal involvement, case 2 showed bilateral mesial temporal hypermetabolism, and Case 3 had no temporal involvement. However, all three of them showed abnormal uptake in basal ganglia. Basal Ganglia T1 and T2 hyperintensities on MRI have been noted in 42% (11) patients in a series of 26 LGI1 encephalitis patients with FBDS [8]. However, the current diagnostic criteria [7] do not account for the findings of increased FDG uptake in bilateral BG in LGI1-positive patients, especially with FBDS. Moreover, FDG‑PET is used to diagnose definite AE only when the clinical, MRI, CSF, and EEG criteria are not met. This series also questions the highly debated question of FBDS being a borderland between being an epileptic seizure versus being a paroxysmal movement disorder [9]. As there is basal ganglia hypermetabolism in all our patients, our data tips the scales toward movement disorders. Despite having better sensitivity than MRI [10], PET is not routinely performed, probably due to practicality issues and uncertain specificity in evaluating AE. Nevertheless, it has proven to be instrumental in altering the diagnosis in patients with normal MRI by helping reach the diagnosis early (when antibody tests are still awaited). PET also helped us modulate/stop therapy in patients, as besides clinical improvement, we saw a resolution of hypermetabolism in the follow-up scans.
留言 (0)