Study Participants
We prospectively enrolled unresponsive or low-response patients with acute traumatic and nontraumatic brain injuries admitted to the neurocritical and cardiological ICUs of a tertiary referral center. The ICUs were screened daily for patients admitted overnight, and patients were consecutively enrolled when deemed feasible by the attending clinical team and patient family consent was obtained. Using automated pupillometry, we investigated patients at least once or, if possible, several times during their ICU stay until they recovered consciousness, were discharged from the ICU, or died, whichever came first. We did tests on one eye (not both). Eye selection was random or based on practical considerations at the bedside. Participants with eye disease of any kind were excluded, as well as acute medically unstable patients. Age-matched and sex-matched healthy volunteers were recruited in parallel using a local advertisement. Each healthy volunteer was investigated once.
Clinical Classification of Consciousness Levels
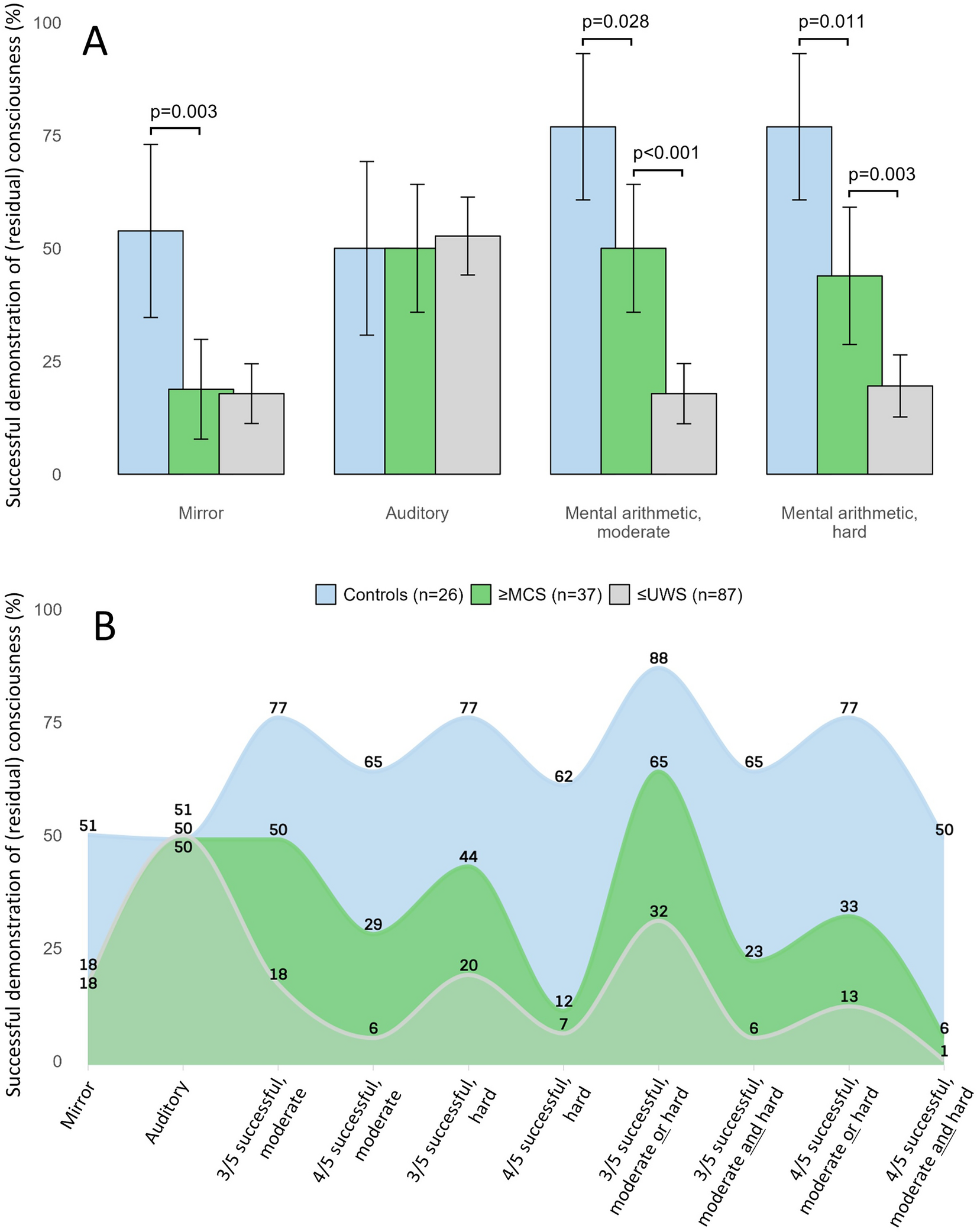
Applying previously described criteria [7], patients with DoC were classified into coma, unresponsive wakefulness syndrome (UWS), minimally conscious states (MCS) minus/plus, and emerged from MCS at each pupillary measurement. Intravenous sedation was stopped or decreased as much as possible [7], Briefly, patients were classified according to consciousness levels by a detailed neurological bedside examination performed under supervision of an experienced board-certified neurologist (DK) just prior to pupillometry. The neurological examination included (1) cranial nerves and sensorimotor status, (2) Glasgow Coma Scale, (3) Full Outline of Unresponsiveness score [14], (4) fixation and visual pursuit using a mirror, (5) ability to follow simple motor commands (including with instructions from the family, if present, to stimulate arousal), (6) reaction to central and peripheral noxious stimuli in the absence of command following, and (7) evaluation of verbal and nonverbal communication. Patients were divided into those without (≤ UWS, i.e., coma or UWS) and those with (≥ MCS, i.e., MCS or better) clinical signs of residual consciousness.
Evaluation of Pupillary Responses to Cognitive Loads
Using a PLR-3000 pupillometer (NeurOptics, Laguna Hills, CA; sampling rate 30 Hz, accuracy ± 0.03 mm), we measured pupillary responses over 10 min (detailed video in the Supplementary Material). When measuring the responses, the examiner kept one of the patient’s eyes open. To prevent dry eyes and eye discomfort, regular rest periods with eyes closed were taken between measurements.
Passive Cognitive Paradigms
The first stimulus was the participants’ own facial reflection in a mirror; the second a series of three different 10 s long sound clips, each with 20 s of white noise interspersed. The first sound clip was “Aaron Copland’s Rodeo—Four Dance Episodes” [15], the second sound clip was that of a crying toddler, and the third sound clip was a burglary alarm, all included for their arousal-inducing properties. We used different thresholds to classify pupil dilation as successful. For the mirror stimulus, a single pupillary dilation was sufficient. For the series of prerecorded sounds, two or more of three pupillary dilations were required for success. We compared the pupillary size during the 10 s of the stimulus to the 5 s immediately before it and to 5 s during the midresting period (so that the pupil could return to baseline after a stimulus).
Active Cognitive Paradigms
These included two series of mental arithmetic tasks of increasing complexity. Mental arithmetic is a robust method to induce cortical activation that has been validated by studies based on functional neuroimaging and electroencephalography (EEG) [16,17,18,19]. Furthermore, we previously showed that such tasks can induce sufficient cognitive load in healthy volunteers and neurological patients detectable by automated pupillometry [12]. It is important to note that successful command following is determined by the attempt to perform a mental calculation. Thus, it is the mental effort and cognitive load that induces pupillary dilation, regardless of whether the result of the calculation is mathematically correct or not. The mental arithmetic tasks consisted of five sets of moderate and five of sets high complexity tasks (4 × 36, 8 × 32, 3 × 67, 6 × 37, and 7 × 43; and 21 × 22, 33 × 32, 55 × 54, 43 × 44, and 81 × 82, respectively). Participants were asked to engage in mental arithmetic and relax, five times in succession. Task duration was set to 20 s with 20 s rest in between, as previously described [12]. Minimal cutoffs for successful command following were defined as three or more pupillary dilations on five mental arithmetic tasks in one set (moderate or hard mental arithmetic). To test more conservative thresholds, we also included analyses using cutoffs of three or more pupillary dilations in both sets and cutoffs of four or more pupillary dilations in one and in both sets.
Pupillary Dilation
The PLR-3000 pupillometer records pupil diameter over time and initially displays the information as a graph on the device. To evaluate pupillary dilation, we uploaded the data as an Excel file via the device’s Bluetooth functionality. We then analyzed pupillary dilations using an in-house developed R package (see the following section). A pupillary dilation was defined as a significantly larger pupil compared with the resting period before and after a stimulus/task (i.e., we calculated the average pupillary size during a stimulus and used an unpaired Student’s t-test to compare it against the averages from preceding and subsequent rest periods). Trigger markers of the applied stimuli were manually inserted while recording. All pupil measurements were included for each period of interest and, as stated, compared using Student’s t-test. Although these were autocorrelated measurements, we used the unpaired t-test because it is more conservative and does not require equal numbers of measurements in the groups. All recordings were visually inspected for artifacts; however, the presence or absence of pupillary dilations were revealed to the investigators only after the publication of the statistical analysis plan [20]. Data points with abrupt deviations exceeding 1.5 mm from the preceding data point (i.e., blinks) were labeled as physiologically implausible and removed. For transparency, we have added a supplemental file revealing all corrected trigger markers (Supplemental Material).
Sample Size and Power Calculations
The study sample size was calculated based on data obtained from a feasibility study [12]. To detect a clinically significant difference in pupillary dilations between resting and stimulation periods, we aimed for a statistical power of 80% and a type 1 error probability (α) of 0.05. This calculation resulted in a minimum required sample size of n = 41 patients. Because the pupillometry paradigm was easy to implement in daily clinical routine and associated with neither harm nor risks, and because we also wanted to test for more conservative success thresholds, we aimed for a sample size of approximately twice that number.
Statistics Analysis
Following a preregistered statistical analysis plan [20], statistics were performed in R (R Core Team, Vienna, Austria). Most of the patients underwent repeated assessments, with each assessment treated as an independent observation, including evaluations of the state of consciousness and pupillometry. The number of pupillary dilations of each group were compared using the χ2 test or Fisher’s exact test as appropriate. Numeric data were analyzed for intergroup comparisons using Student’s t-test, the Mann–Whitney U-test, or the Kruskal–Wallis test, as appropriate. Spearman’s rank analysis was done to assess the association between average pupillary dilations (in millimeters) during mental arithmetic and consciousness levels. A p ≤ 0.05 was considered significant.
Data Sharing Statement and Code Availability
All study data are available in the article and Supplementary Material (including raw data). The algorithm for pupillometry data processing is available at https://github.com/lilleoel/clintools.
Additional Material
Details are provided (1) in a preregistered statistical analysis plan at Zenodo.org [20]; (2) in the online Supplementary Material, including pupillometry raw data, anonymized patient data, and a videoclip of the examination setting; and (3) at https://cran.r-project.org/web/packages/clintools/, which also includes the code for processing the pupillometry data. We also provide a step-by-step guide to use automated pupillometry for the bedside detection of covert consciousness (Supplementary Methods).
Ethics
Regional Ethics Committee (Region Hovedstaden) approval was obtained (H-21022096).




留言 (0)