
記住我






Stroke (often called cerebrovascular accident in the 1950s) was mostly understood as ischemic injury due to occlusion of a large cerebral artery or as an intracerebral nontraumatic hemorrhage (ICH). Early studies of cerebral hemorrhage were hampered by lack of angiographic verification, lack of computed tomography, lack of autopsy confirmation, lack of neurosurgical options, lack of sufficient reversal of a coagulopathy, and other imperfections, such as timing (when to consider a clinical sign stable). The only available solution was careful assessment of the early trajectory of the patient with changing neurological examination. Early outcome assessment was crudely simplistic.
By now we know that even as the hemorrhage is large on computed tomography, even when the patient is hard to awaken before going to the operating room, and even when the hemorrhage has expanded, the patient’s functionality and quality of life can still be manageable.
In the 1980s, newer studies on outcome gave clinicians a better sense of the natural history [1, 2]. These studies could then be a benchmark toward the evaluation of medical or surgical treatments.
Surgical selection of patients and surgical techniques of revascularization also largely remained unknown. For example, better insight into prognostic factors could address the potential benefits of surgical evacuation of a cerebral hematoma.
Furthermore, outcome studies identified causes of worsening that led to better recognition. Investigators recognized that the natural history of acute stroke is biased by referral patterns, and in some hospital series, these included the more severely affected patients. This prompted the development of studies of patients from a defined geographic location (“population-based studies”).
Medical complications only recently received attention. Modern intensive care unit care undoubtedly improved outcome, and better outcomes became apparent when patients with stroke were transferred to more secure settings rather than being simply observed on the ward.
The complex interaction of many factors makes studying the natural history almost futile. Most studies of patients with a recent cerebral hemorrhage identified that the neurological examination of the patient and the initial clot size (> 50 ml) were potent predictors of outcome. Initial studies undoubtedly used heterogeneous groups; later studies were more location specific, in particular when computed tomography scans became available in the early 1970s. Limited deficits in a patient with a presumed ischemic stroke could now be linked to a hemorrhagic stroke, and this changed the epidemiology of stroke.
Tuhrim’s studies were an important first attempt in sorting out the melee of factors contributing to outcome in cerebral hemorrhage [3,4,5].
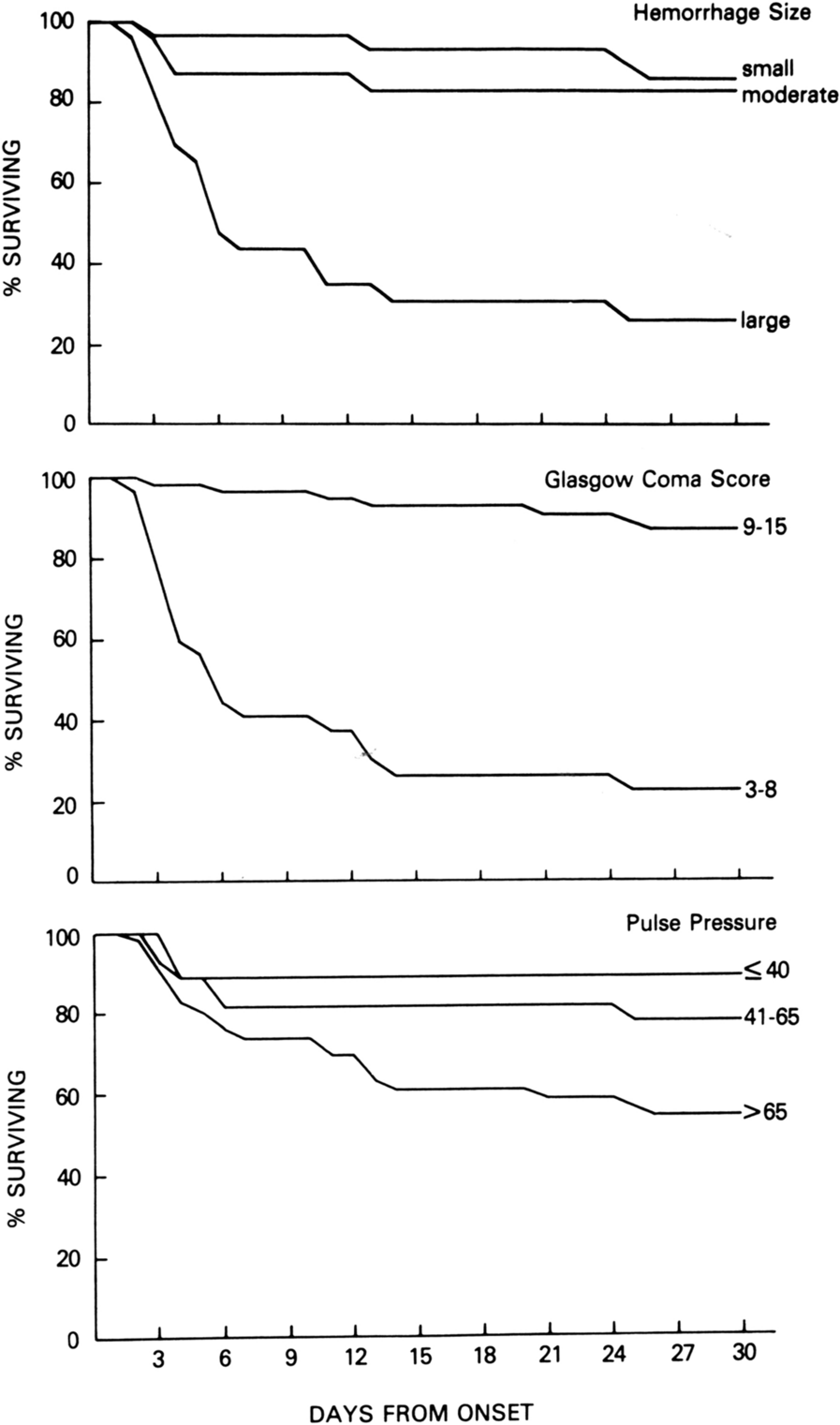
In 82 patients, the 30-day survival status was known. Tuhrim et al. [3] identified multiple variables possibly related to ICH outcome. He included medical history (21 variables), demographics (11 variables), stroke course (eight variables), physical examination (four variables), neurological examination (20 variables), and laboratory values (seven variables). The data were obtained through the pilot phase of the stroke data bank, a cooperative effort of four hospitals and the National Institute of Neurological Disorders and Stroke. All statistically significant variables were entered into a multiple logistic-regression model. Factors associated with outcome were Glasgow Coma Scale score, systolic blood pressure, vertical gaze palsy, severity of weakness, presence of brainstem or cerebellar deficits, clinical course, and size of parenchymal hemorrhage. The major prognostic factors included Glasgow Coma Scale (≤ 8), size of hemorrhage (large, > 1 lobe; small, < 1/2 lobe), and pulse pressure (≤ 40 mm Hg, 41–65 mm Hg, or > 65 mm Hg).
Application of Tuhrim’s model resulted in 90% correct prediction. The worst prognosis was seen in a patient with a Glasgow Coma Scale < 8, hemorrhage involving more than one lobe, and a pulse pressure > 65 mm Hg. The prognostic value of the pulse pressure was novel. Pulse pressure is defined as the difference between systolic blood pressure and diastolic blood pressure, which represent the maximal and minimal circulatory pressures during the cardiac cycle, respectively. A “widened” pulse pressure is defined as > 100 mm Hg. Pulse pressure is a surrogate of increased intracranial pressure when systolic blood pressure increases as a Cushing reflex outgains systolic pressure (Fig. 1 [3]). The model was later validated with inclusion of hyperglycemia and intraventricular hemorrhage extension as additional variables [4], in which intraventricular hemorrhage contributed significantly.
Fig. 1
Outcomes per variable [3], John Wiley & Son, used with permission
Current ICH models have included Glasgow Coma Scale score, National Institutes of Health Stroke Scale, ICH volume, location (supra or infratentorial), age, and presence of comorbidity, but no universal scale has emerged, and there is lack of a standard [6,7,8,9,10,11,12]. Further differentiation by specific lesion site has proven helpful in determining prognosis. Studies found that extension of the hemorrhage mattered greatly. For example, extension of a putaminal hemorrhage into the posterior limb of the capsule markedly reduces the chance of motor recovery. Further classification included lesions involving anterior limb of capsule and thalamus. Moreover, the significance of intraventricular hemorrhage depended on the location, with poor outcome in putaminal hemorrhage but much higher chance of recovery in caudate hemorrhage. Presence of acute hydrocephalus (often a result of shift and compression of a large hematoma) also became recognized as a poor prognosticator in ganglionic hemorrhage, with trivial improvement after aggressive management with ventriculostomy placement.
In the early 1980s, anticoagulation-associated hemorrhage received more attention, and aggressive reversal of warfarin became a major part of management. Outcome prediction in patients presenting early with cerebral hemorrhage likely relates best to clinical assessment of brainstem injury. With it, the outcome is poor; without it, the degree of midline shift reflects size and predicts morbidity. Older age, previous functional status, and greater severity of neurological condition, and expansion to a greater volume are major indicators of worse prognosis for survival and neurological recovery after ICH. The neurological examination must be assessed at several time points. The degree of brainstem involvement in acute supratentorial lesions has always been the most important determinant.
The effectiveness of anticoagulation-reversal therapy in ICH has not been established in phase III randomized trials, and this most certainly applies to the timing of administration. Renewed interest in blood pressure control came with the recent ICH treatment trials, such as INTERACT and ATACH [13, 14]. But recently, the prognostic value of a widened pulse pressure was again confirmed [15]. The relationship between widened pulse pressure and mortality in ICH remains unclear. The authors queried whether this relationship represents a dynamic, potentially modifiable acute-phase process or a reflection of chronic underlying systemic atherosclerosis. A second mechanism may involve disruption of autoregulation and a resultant need to maintain adequate stroke volumes. A third mechanism may be higher pulse pressures associated with severe brain edema.
The most important determinant, however, may be that premature withdrawal of life-support measures leads to a “self-fulfilling prophecy.” The argument is that delivery of an (unjustified) overly pessimistic prognosis leads to withholding or withdrawing aggressive care, which results in a possibly avoidable death. Several studies have found correlations between early limitations of care and greater mortality, particularly in patients with ICH [16]. Furthermore, the use of a care bundle protocol (order set) incorporating the early control of elevated blood pressure together with management algorithms for hyperglycemia, fever, and abnormal coagulation resulted in an improved functional outcome at 6 months [17]. After all, history teaches us that while outcome may seen obvious, long term prognosis is determined by medical and surgical management of the patient and is not always a given fact. History thus teaches us that the early benchmarks of outcome are still unknown. Probabilities adjust as the clinical trajectory shifts.
留言 (0)