
記住我



Between 2019 and 2021, we recruited 28 stroke patients from the rehabilitation department of Chang Gung Memorial Hospital. We screened 557 patients, but excluded 525 patients. Four patients declined to participate, leaving us with a total of 28 participants. We randomly assigned them to either the rPMS + iTBS group (n = 14) or the sham rPMS + iTBS group (n = 14). The inclusion criteria for the study were as follows: (1) aged between 20 and 80 years; (2) ischemic or hemorrhagic stroke for the first time; (3) unilateral cerebral stroke with hemiplegia or hemiparesis; and (4) subacute (between 7 days and 6 months since onset) or chronic (more than 6 months since onset) stages of stroke [29]. The exclusion criteria were as follows: (1) stroke at brainstem or cerebellum; (2) progressive neurodegenerative diseases; (3) history of epilepsy; (4) medical histories of aneurysm and cerebral arteriovenous malformation; (5) patients with active medical problems; (6) active psychiatric disorders; (7) severe cognitive and language impairment; (8) metal implants such as pacemakers, head metal implants, and aneurysm clips; (9) Botox injections in six months; and (10) patients who are pregnant or who are probable pregnant. All patients signed the informed consent prior to the enrollment. The study protocol was executed in accordance with the Declaration of Helsinki and was approved by Chang Gung medical foundation institutional review board. This trial is registered under ClinicalTrials.gov ID No. NCT04265365.
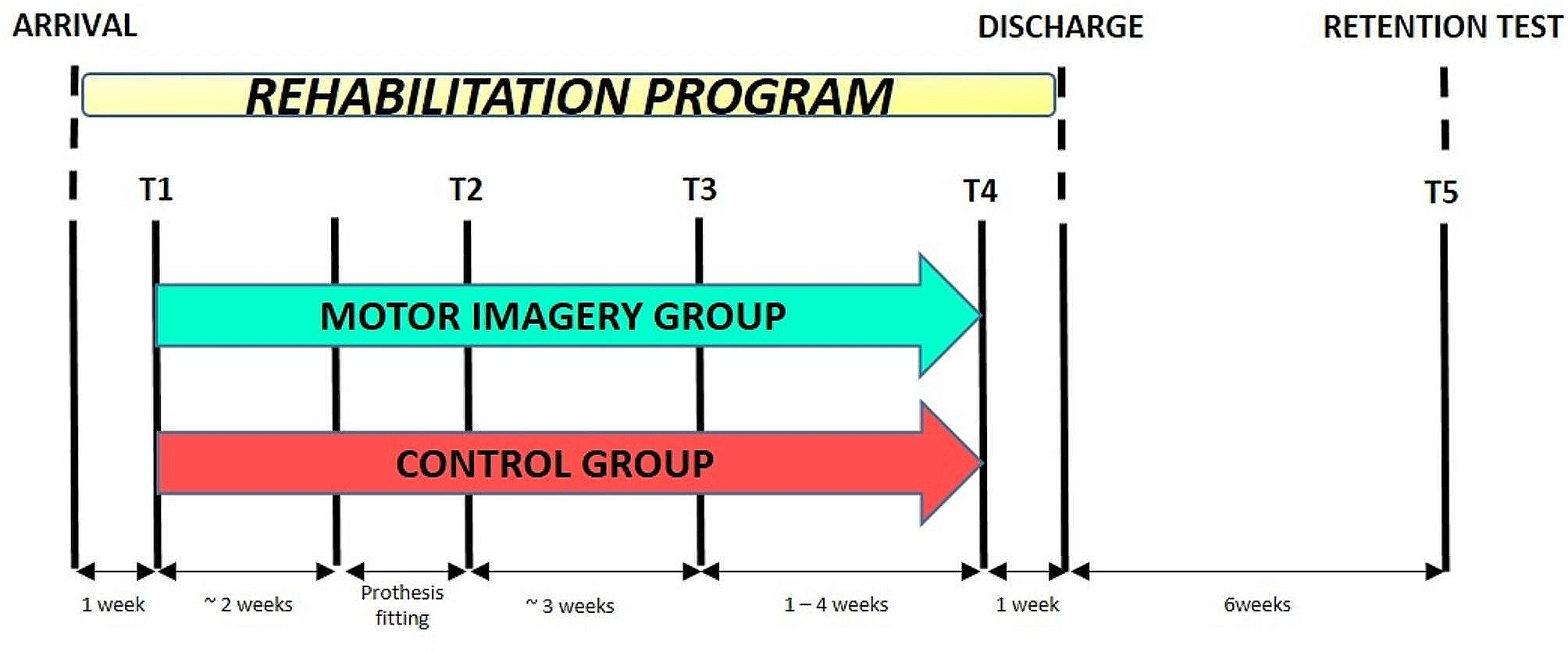
Study designThe study was a prospective double-blinded, randomized, controlled trial. Various measures or restriction were used to ensure intervention and assessment accuracy and consistency. The severity of stroke was stratified according to Brunnström stage [30, 31] before randomly allocating the twenty-eight patients into two groups on the website (https://www.randomizer.org/) because the Brunnström stage is a quick and convenient bedside evaluation method to assess a patient’s recovery stage. The clinical data were also recorded. Figures 1 and 2 demonstrated the randomized allocation and experimental design, respectively. The patients were asked to relax 5 min before, during, and 5 min after the stimulation to avoid the effects of physical activities on central iTBS. The patients received 10 courses of central iTBS with real or sham rPMS on consecutive working days for 2 weeks. The rPMS was delivered before central iTBS. Outcome measures were performed 3 days before intervention and after intervention. The evaluators were well trained to administer outcome measures prior to the project after passing competency and reliability test. At least two professional evaluators blinded to the group assignment performed the outcome measure and, both intra-rater and inter-rater reliability should be recorded. The intra-rater/inter-rater reliability of the Action Research Arm Test (ARAT) and FMA-UE was 0.986/0.998 and 0.984/0.992, respectively. The intra-rater reliability of the Functional independence measure-Self care (FIM-Self care) and Stroke impact scale (SIS) were 0.994, 0.956, respectively. Besides magnetic stimulation, patients received comprehensive rehabilitation programs, including physical therapy (60 min) and occupational therapy (60 min), both administered five times a week. Additionally, specialized speech-language therapy was provided for patients exhibiting symptoms related to speech and swallowing issues.
Fig. 1
Flow diagram of recruitment and randomized allocation
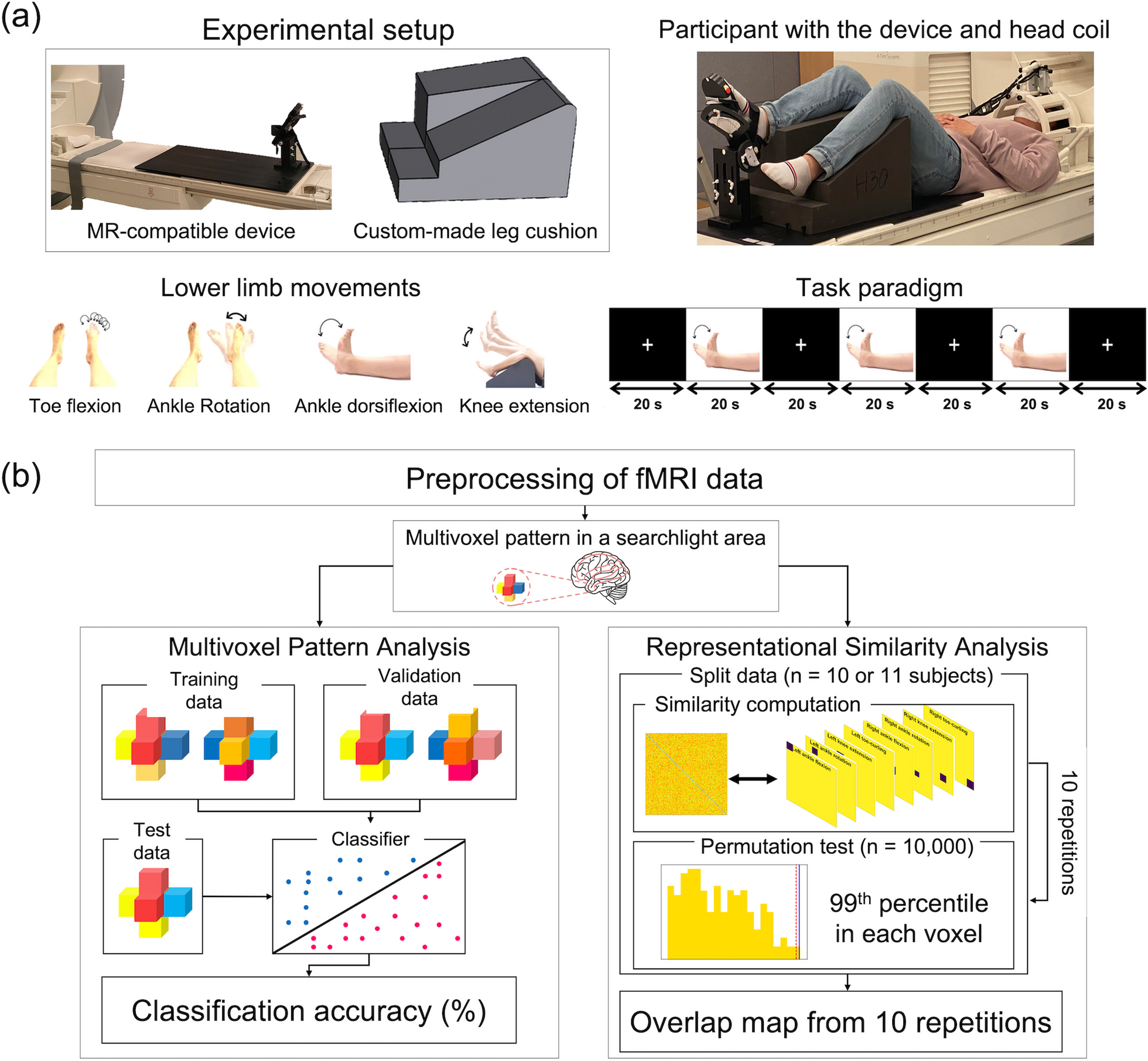
Fig. 2 Participant selection and positioning
Participant selection and positioningParticipants were carefully screened based on inclusion/exclusion criteria. This involved assessing upper limb dysfunction severity via the Brunnström stage, ensuring medical stability, and verifying their comprehension and participation capability. Participants were consistently positioned, with forearms resting on a desk during rPMS and central iTBS administration to minimize variability.
Randomization and blindingTo ensure the integrity of the blinding process, participants were randomly assigned to either the rPMS + iTBS group or the sham rPMS + iTBS group through the (https://www.randomizer.org/) website. The generated sequence was concealed from both the researchers and the participants until the allocation process was completed, maintaining the integrity of the randomization process. Patients were then assigned to their respective groups according to the generated sequence. An independent researcher not directly involved in assessments or interventions carried out the allocation. Importantly, the operators responsible for administering the stimulation and the evaluators conducting the outcome measurements were separate individuals, and they were unaware of each other’s roles. Furthermore, the evaluators remained blinded to the patients’ group assignments throughout the study, enhancing the study’s double-blind nature. Additionally, patients were kept unaware of the specific treatment conditions, further ensuring the blinding of the intervention.
Standardization of assessments and interventionsAll individuals, including evaluators and operators, underwent comprehensive training and competence tests to ensure their qualifications and expertise. Evaluators were trained for assessment accuracy, and supervised by the principal investigator and a senior certified occupational therapist. Operators were trained and supervised by the principal investigator and a senior neurologist to ensure standardized equipment operation.
Determination of AMT and RMTThe study used the TMS protocol to evaluate the Active Motor Threshold (AMT) and Resting Motor Threshold (RMT ). The MagProX100 package (Magventure, USA)was used for magnetic stimulation with a figure-of-eight coil (outer diameter of each wing 7.5 cm). Silver/silver chloride (Ag/AgCl) disc electrodes were attached to the first dorsal interosseous muscles (FDI) of the affected limb. The coil was positioned tangentially to the scalp over the motor area of the affected limb in the optimal position for activating the FDI. The handle was held pointing backward and laterally at an angle of 45° to the sagittal plane to generate a posterior-to-anterior current flow in the brain. The point at the scalp that induced the maximum MEP was identified as the motor hot spot [32]. If the MEPs could not be induced, we would identify the motor hot spot from the mirror site from unaffected hemisphere [32]. The MEP was recorded using a Multifunctional Response and Stimulus Device (BioPAC Inc, USA). The patients were seated in a comfortable chair with their forearm in a pronated position on the desk. They were instructed to remain relaxed throughout the procedure. The RMT was defined as the minimal intensity of TMS that induced an MEP equal to the 50 uV peak-to-peak amplitude when the FDI was relaxed in at least 5 of 10 consecutive trials. The AMT was defined as the intensity of TMS that induced an MEP equal to the 200 uV peak-to-peak amplitude when the FDI slightly contracted in at least 5 of 10 consecutive trials (10–20% of maximum contraction).
Central iTBS and rPMS protocolDuring the study, we administered iTBS to either the affected primary motor cortex as central iTBS or to the radial nerve as rPMS. To administer central iTBS, we used a handheld figure-of-eight coil at the motor hot spot of the first dorsal interosseous (FDI) muscle, while for rPMS, we applied the coil at the radial groove.
As for central iTBS, we administered iTBS to the affected primary motor cortex. The true stimulation was given at 80% of AMT or 70% of RMT.
As for rPMS, the stimulation intensity for real rPMS was individually adjusted for each participant to achieve a joint movement resulting from muscle contraction of extensor carpi radialis muscle. In contrast, sham stimulation was set at a low-intensity level at 5% of the maximal stimulator output [33], which did not induce the MEP in the extensor carpi radialis muscle. The participants receiving sham stimulation were still able to perceive the noise, leading them to maintain the belief that they were indeed receiving the stimulation throughout the study. Besides, participants were kept separate from each other and were unaware of the group assignments. Each session of iTBS comprised 20 rounds of stimulation. Each round consisted of a 2-second burst at 5 Hz followed by an 8-second period of rest. Each burst contained 3 pulses at 50 Hz, resulting in a total of 600 pulses per session, which lasted 200 s. We administered 2 sessions of iTBS for central iTBS and rPMS, with a 10-minute break between sessions. The stimulation was conducted at the same time each day for five consecutive days per week for two weeks.
Outcome measuresThe primary outcomes were the improvement in motor function, as reflected by the scores on the FMA-UE and the Action Research Arm Test (ARAT). The FMA-UE is a performance-based scale used to evaluate motor function of upper limbs in patients with stroke [23]. In contrast, the ARAT is composed of 19 items divided into four subsections, including grasp, grip, pinch, and gross movement [24].
Secondary outcomes focused on improvement in activities and participation. Activities were assessed using the self-care domain of the Functional Independence Measure (FIM). The self-care domain was selected for this study because it comprises six items specifically associated with activities of the upper limb [34].
Participation was evaluated using the Stroke impact scale (SIS), a self-report assessment of disability and quality of life after stroke [35]. The SIS includes eight domains: strength, hand function, activities of daily living (ADL), mobility, communication, emotion, memory and thinking, and participation. The scale comprises 59 items that are rated on a 5-point scale, with a score of 5 representing the best performance in participation.
Statistical analysisThe data was processed by SPSS version 21.0 for Windows (SPSS Inc., Chicago, IL, USA). Shapiro–Wilk tests were adopted to confirm the assumptions of normal distribution, and only total SIS, some SIS domains, and FIM-Self care met the criteria. Therefore, we used nonparametric method to analyze the data. The baseline of outcomes and demographic of clinical characteristics were analyzed under Chi-square test or Fisher’s exact test for categorical variables and an Independent t-test for continuous data. Wilcoxon signed-rank test was applied to determine whether each group had significant improvement after the intervention. Analysis of covariance was adapted to test whether the rPMS + iTBS group showed greater improvement than the sham rPMS + iTBS group after treatment. We defined pre-treatment performance and baseline differences (sex, and Mini Mental Status Examination (MMSE)) as the covariates, with group as the independent variable, and post-treatment performance as the dependent variable. We conduct power analysis for repeated measures design using G*Power software (G*Power 3.1.9.7) to estimate our sample size requirement [36]. We found that a total of 27 participants will be required for effect size of 0.5 with a power of 0.8 and type I error of 0.05. Thus, we recruited 28 participants, resulting in 14 participants for each group. The significance was pinpointed at 0.05 (one-tailed) and, we adopted t-distribution to determine a 95% confidence interval (95% CI) for small sample size (n < 30).
ResultThe demographic and clinical data did not differ in age, stroke side, stroke stage, stroke location, stroke type, aphasia, MMSE, NIHSS, modified Ashworth scale, and Brunnström stage except sex (Table 1). The baseline of outcome measures did not differ between groups (Table 2). All patients well tolerated the intervention without significant adverse effects in the study.
Table 1 Demographic and clinical characteristicsTable 2 Baseline of outcome measurePrimary outcomesMotor functionIn FMA-UE, both groups had significant improvement after the intervention (rPMS group: p = 0.019; sham group: p = 0.025) (Table 3). However, the change scores did not differ in FMA-UE between groups.
Table 3 Descriptive and inferential statistics of primary outcome measuresIn total ARAT, both groups did not achieve significant improvement after the intervention (Table 3). In Grasp domain of ARAT, only rPMS + iTBS group attained significant improvement. (Grasp domain: rPMS: p = 0.013; sham group: p = 0.107). The change scores did not differ between groups in total ARAT and the four domains of ARAT.
Secondary outcomesActivityIn FIM-Self care, both groups achieved significant improvement after the intervention (rPMS group: p = 0.013; sham group: p = 0.011). The change scores did not differ between groups.
ParticipationIn total SIS, both groups did not attain significant improvement after the intervention (rPMS group: p = 0.064; sham group: p = 0.352). The rPMS + iTBS group had significant improvement in Strength and ADL. The rPMS + iTBS group had borderline improvement in Hand Function. The sham rPMS + iTBS group achieved significant improvement in Mobility. (rPMS group: Strength: p = 0.019; ADL: p = 0.040; Mobility: p = 0.346; Hand Function: p = 0.050; sham group: Strength: p = 0.385; ADL: p = 0.430; Mobility: p = 0.034; Hand Function: p = 0.562). The change scores did not differ in total SIS and the 8 domains of SIS between groups.
Table 4 Descriptive and inferential statistics of secondary outcome measures
留言 (0)