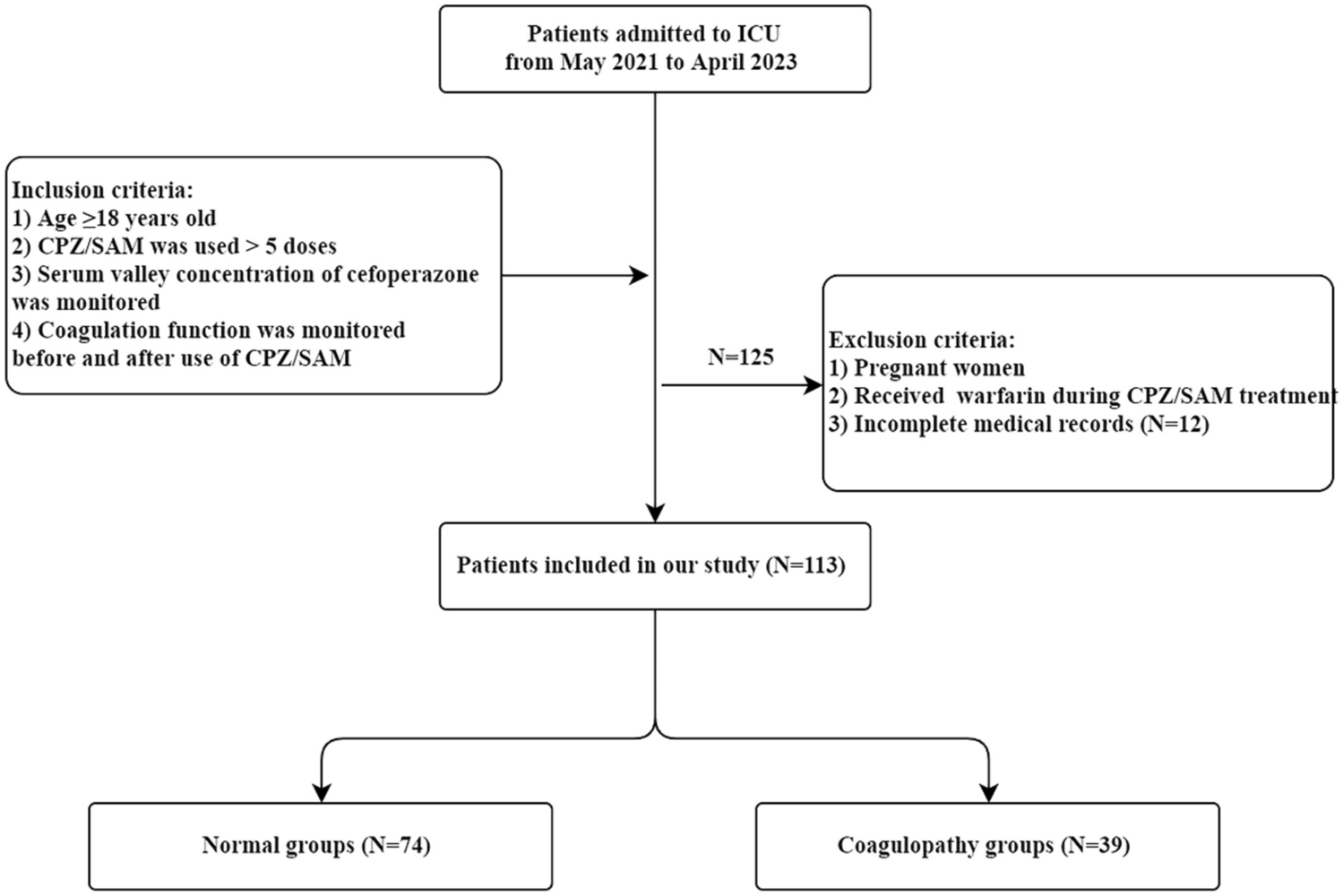
Coagulopathy is a more serious adverse reaction during the use of CPZ-containing drugs, and the incidence of coagulation dysfunction in patients using CPZ/SAM has been reported to be about 25.8% or even up to 45% in clinical practice [7]. The main manifestations are reduced prothrombin activity, prolonged prothrombin time, and thrombocytopenia [8, 9]. Grasela et al. [10] concluded that patients with severe disease are at the highest risk of developing coagulopathy. Due to their specific pathophysiological situation, critically ill patients may already be in a relatively disturbed state of coagulation. This phenomenon is mainly associated with endothelial cell damage caused by factors such as the release of inflammatory transmitters and activation of leukocyte adhesion factors in patients, or with the inflammatory response of patients [11]. At the same time, the pharmacokinetics of CPZ in critically ill patients undergo significant changes [12], which increases the risk of CPZ-induced coagulation dysfunction. Patients with severe coagulopathy not only experience a significant increase in bleeding events and transfusion volume but are also more likely to develop multiple organ dysfunction syndrome, with a mortality rate more than 4 times higher than that of patients with normal coagulation function [13]. This study showed that the incidence of coagulation dysfunction induced by CPZ in critically ill patients is 34.5%, with a bleeding event rate of 7.08%. Patients in the coagulopathy group experienced significant PT prolongation around 6 days (median) after CPZ application.
This study attempted to determine the threshold of toxic exposure to CPZ by therapeutic drug monitoring (TDM). To our knowledge, this is the first study on the concentration-response relationship of CPZ-induced coagulation disorders. Previous studies only found that CPZ was associated with an increased risk of hypoprothrombinemia and bleeding, and there was a dose–response relationship. Chen et al. [14] suggested that patients who used anticoagulants, suffered from liver failure, or malnutrition, and had a history of bleeding events faced a significantly increased risk of bleeding events. They calculated the cumulative dose of CPZ based on a defined daily dose (DDD), and when the cumulative dose exceeded 5 DDDs, the incidence of bleeding events was even higher. In a retrospective cohort study involving 476 patients, the risk of prolongation of PT was found to increase fivefold in the high-dose group of CPZ (> 4.5 g/d) compared to the cefotaxime or ceftizoxime group and 16-fold compared to the ceftazidime group [15]. Andrassy et al. [16] also demonstrated that in the presence of high CPZ serum Cmin, a platelet defect with prolonged bleeding time and impaired platelet aggregation may occur. In this study, the Cmin threshold for CPZ-induced coagulation dysfunction was 87.765 mg/l, and the AUC was 0.734, which had a good predictive value by plotting the ROC curve. Moreover, the results of multivariate logistic regression analysis showed that cefepime Cmin ≥ 87.765 mg/l was associated with a fivefold increase in the risk of CPZ-induced coagulopathy in patients.
Vitamin K is an essential cofactor for the carboxylation of hepatic cell mitochondria. It is involved in the γ-carboxylation reaction of glutamic acid in prothrombin precursors and is mainly obtained from daily dietary intake [17]. Many studies have suggested that there are two main mechanisms for CPZ-induced coagulopathy: (1) CPZ is hardly metabolized in the body, with about 75% excreted in bile, inhibiting the growth of normal intestinal flora and reducing the synthesis of vitamin K in the intestines; (2) the N-methylthiotetrazole (NMTT) side chain carried by CPZ has a structure similar to glutamic acid, which can interfere with the carboxylation of vitamin K in the liver, thereby reducing the synthesis of prothrombin and lowering the levels of coagulation factors II, VII, IX, and X that depend on vitamin K [18, 19]. Nevertheless, prophylactic use of vitamin K1 prior to CPZ therapy remains controversial. In a retrospective cohort study of 374 patients treated with CPZ in a teaching hospital, prophylactic use of vitamin K did not reduce bleeding [15]. Rockoff et al. [20] concluded that routine use of vitamin K and CPZ for perioperative infection prophylaxis may not be necessary. The results of a clinical trial showed that 141 patients who received CPZ without prophylactic vitamin K did not bleed [21]. The logistic regression results of this study indicated that the prophylactic application of vitamin K1 is an independent protective factor for preventing CPZ-induced coagulation disorders. Prophylactic administration of vitamin K1 can significantly prevent patients’ coagulation disorders, even when exposed to higher concentrations of CPZ.
Currently, there were many studies on the factors influencing the abnormal coagulation function caused by CPZ, and a large number of studies believed that the risk of this coagulopathy is closely related to the patient’s own pathological and physiological conditions. Advanced age, cancer, malnutrition, underlying hepatic impairment, renal insufficiency, combined use of anticoagulants, and previous bleeding history were all considered risk factors for CPZ-induced coagulopathy [7, 22]. The results of this study showed that combined hepatic impairment was an independent risk factor for coagulation dysfunction in patients (OR, 5.616; p = 0.014), which was consistent with previous studies. Hepatic insufficiency can lead to reduced drug metabolism and accumulation in the body, as well as a decreased ability of the liver to synthesize its own coagulation factors, leading to abnormal coagulation [22]. In a study of 35 patients with severe infections and renal dysfunction [23], in non-jaundiced patients with abnormal liver function, the mean peak and trough serum concentrations produced by a 2-g dose every 12 h were 254 and 125 mg/l, respectively, while in five tests with normal liver function, they were 179.5 and 19.5 mg/l, respectively. Although the trough value increased significantly, there was no statistical significance (p > 0.1).
In this study, an APACHE II score > 25 was also found to be associated with CPZ-induced coagulopathy (OR, 3.229; p = 0.034). The APACHE II score is currently the most widely used system for assessing the condition and prognosis of critically ill patients in clinical settings and can serve as an indicator for evaluating the condition and prognosis of patients in intensive care units [24]. It has been shown that critically ill patients with an APACHE II score of > 10 are at high risk for severe malnutrition [25]. This also explained why patients with higher APACHE II scores are more likely to experience CPZ-related coagulation dysfunction. However, when the Nutric score (p = 0.052) was included in a multivariate logistic regression, it was progressively eliminated from the model. This may be related to the bias in the definition of malnutrition and nutrition scores of the included population. Meanwhile, there was no statistical difference in gender between the two groups (p = 0.052). However, in previous studies, results showed that when including patients under 12 years old, the incidence of antibiotic-associated hypoprothrombinemia in males was higher than in females. They concluded that according to the effect of sex hormones on prothrombin, in the presence of estrogen, prothrombin formation is faster, and the effective concentration of vitamin K is lower. The level of prothrombin is higher in women than in men, and the dietary requirement of vitamin K is lower in women [26]. Perhaps because of differences in the included populations, this study could not reach similar conclusions. Cohort studies with larger sample sizes may be needed regarding the effect of sex hormones on prothrombin.
Drugs that may cause coagulation disorders in patients were also included in the analysis, including antiplatelet agents, other antimicrobials, drugs that may cause bleeding (NSAIDs and glucocorticoids), and anticoagulants (heparin and new oral anticoagulants) [27]. Univariate analysis showed that the combined use of tigecycline was associated with prolonged PT in patients. According to current researches, tigecycline could cause prolongation of PT and APTT, elevation of INR, decreased platelet count [28], and hypofibrinogenemia. Hu et al. [29] analyzed the characteristics of patients with hypofibrinogenemia who received treatment with CPZ/SAM and found that these patients had a higher incidence of coagulation abnormalities (p = 0.009) and required more blood products (p = 0.003). However, this study did not obtain similar results, possibly due to the small sample size and the use of vitamin K1 for prevention, indicating the need for large-scale cohort studies to draw conclusions. Several recent studies have also yielded similar conclusions [30,31,32]. Furthermore, Miao et al. [31] also investigated the effect of the combined use of sodium valproate on CPZ-induced coagulation disorders, and the results showed that sodium valproate is not associated with this adverse reaction, which is consistent with our research findings. Low-dose aspirin is commonly used for antiplatelet therapy, but its antiplatelet mechanism may lead to an increased risk of bleeding. When patients on long-term aspirin use CPZ for antibiotic therapy, the combination of CPZ and aspirin can have a cumulative effect on coagulation dysfunction, resulting in a significant increase in the risk of bleeding [33]. However, this study has not yielded similar conclusions, possibly because the duration of combined use of aspirin and CPZ in ICU patients was insufficient for us to observe the occurrence of this phenomenon. A prospective observational study has also concluded that the combination of vancomycin, a commonly used drug for Gram-positive bacteria in the ICU, with CPZ could lead to a significantly higher risk of coagulation disorders [34]. Although this study did not find any drug combination as a risk factor for CPZ-induced coagulation dysfunction, caution should still be exercised in clinical practice regarding the potential bleeding risk associated with these drugs.
Obviously, the patient’s own risk factors are an important component of adverse reactions, and higher serum Cmin levels of CPZ amplify these inducing factors [35]. This study has certain limitations. Firstly, this is a single-center, retrospective case-control study, which cannot exclude the bias of medical monitoring. Secondly, the heterogeneity of critically ill patients limited our statistical analysis. The serum Cmin threshold of coagulation disorders caused by CPZ needs further multicenter, prospective, randomized controlled studies to determine. Thirdly, this is a study aimed at the Chinese population and does not involve discussion of other races. We did not conduct genetic testing on the patients, and in fact, pharmacogenetics is also an area worth exploring. For example, since CPZ is mainly excreted via bile, it has been suggested that multidrug resistance-associated protein (MRP) 2 (ABCC2) is the transporter protein primarily responsible for CPZ excretion. In patients with hereditary MRP2 (ABCC2) expression deficiency, if there is no compensatory efflux mediated by other transporter proteins, it may lead to obstruction of CPZ excretion in bile, resulting in elevated blood drug concentration and potential occurrence of coagulopathy [36, 37]. Not only that but due to the possibility of vitamin K epoxide reductase (VKOR) being one of the targets of NMTT [18], we are unable to rule out its pharmacogenetic effects. Whether single nucleotide polymorphisms (SNPs) in VKOR increase CPZ sensitivity and lead to coagulation disorders in patients, further genomic research may be needed to confirm this hypothesis. Nevertheless, our study results still provide valuable information about the serum Cmin threshold of coagulopathy caused by CPZ in real-world patients.
In conclusion, we found that the incidence of coagulopathy in critically ill patients treated with CPZ was 34.5%, with a higher likelihood of bleeding events. The median time for the occurrence of coagulation dysfunction was 6 days, and the CPZ serum Cmin threshold was 87.765 mg/l. Prophylactic application of vitamin K1 significantly reduces the incidence of this adverse reaction in critically ill patients. We recommend that critically ill patients with an APACHE II score > 25 and combined hepatic impairment should have timely TDM and coagulation monitoring with the application of CPZ-containing drugs, and it would be more prudent to apply vitamin K1 prophylaxis, while ensuring the efficacy of CPZ treatment in order to prevent coagulopathy and fatal bleeding events.






留言 (0)