The results demonstrate that the OH children’s blood Pb surveillance program is robust and representative based on the calculated exceedance rate and population rate and that BLL data can be used in the generalizable approach initially published in Xue et al. [15] in other states or locations. The kappa statistic over time showed substantial to near perfect agreement, proving that visual observation translated to quantitative concordance. This is further supported by an analysis by Roberts et al. [16] who report a high ascertainment ratio (0.93) for OH that reflects a high likelihood that testing is comprehensively capturing those children with EBLL. Although the statistical modeling was conducted for 1999–2010 using 10 µg/dL for calculating prevalence [16], the ODH blood Pb screening guidance has been consistent, such that these findings should hold for the years included in the current analysis.
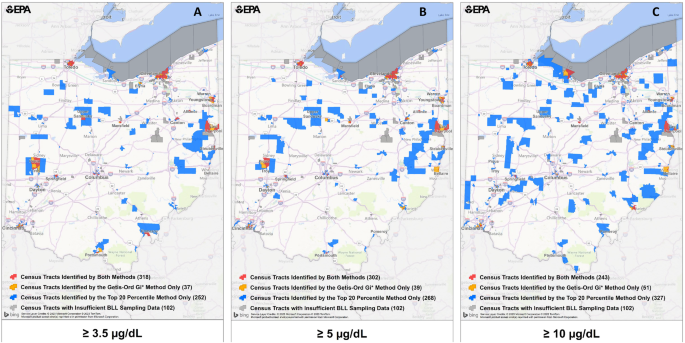
Comparing results across different EBLL thresholds facilitates evaluation of the ability to properly detect census tracts of potential Pb exposure. We demonstrated that the most recent blood Pb reference value (3.5 µg/dL) can be used with the derived BLL metrics and spatial analysis approaches to identify areas for targeting. The strong agreement between 5 and 3.5 µg/dL results for the years analyzed provides confidence that blood Pb surveillance programs will continue to identify areas containing children most at risk for Pb exposure. The limit of quantification per the ODH for capillary measurements is 3.3 µg/dL, so using a cutoff of 3.5 µg/dL should not result in misclassification. In addition, the EBLL rate utilizing percentages rather than absolute values was intentionally derived for the generalizable approach to avoid potential challenges in having to consider how to handle limits of detection at the lower end of the BLL distribution.
The observed decrease in EBLL over time in OH was also observed for MI [15]. As with MI, the biggest gains in lowered numbers of census tracts with EBLL in OH were from 2005–2010, with smaller improvements from 2011–2018. Similarly, there was a shift in the BLL distribution to the left, with fewer census tracts identified in the later years as being in the upper percentiles for EBLL. For 2014–2016 with a blood Pb threshold of 5 µg/dL, the percent of census tracts in OH with EBLL of >10% was 10.9% compared to 7.7% for MI and the statewide percentage being 4.5% compared to 4.1%, respectively. The 2017–2018 data for OH puts the number of census tracts with the percent of EBLL > 10% similar to MI at 8.6%. These data can be contrasted to the 2.5% national EBLL percentage that is used by CDC in their blood Pb reference value that was lowered from 5 to 3.5 µg/dL in 2021.
From 2007–2018, over 150,000 children aged 0 to <6 years of age were tested each year for blood Pb in OH [27]. Of those, 2.3 to 2.8% of children tested had a confirmed EBLL of 5 µg/dL or higher [28]. OH requires a confirmation venous draw for any capillary blood Pb result that is ≥5 µg/dL to identify individual children who require follow-up care. In our analysis, the statewide EBLL percentage was 3.5% for 2017–2018 when EBLL was defined as ≥5 µg/dL, which is higher than the 2.3 to 2.8% reported by ODH [28]. This likely reflects the inclusion of both capillary and venous blood Pb data in our methodology. This choice reflects our interest in examining individual BLL data for patterns at the community level, with the goal of providing valuable insights for targeting outreach or mitigation efforts at this broader scale.
In a study that evaluated findings of OH site investigations of children with reported BLL > 10 µg/dL, deteriorated interior paint, deteriorated external paint, dust and bare soil were most identified as hazards [29]. Of the 5% of cases where a bare soil sample was collected, Pb concentrations were often in excess of 400 ppm, with the greatest concentrations occurring closest to building structures where exterior paint and drip lines may be potential Pb sources. These assessments most often occurred in Mahoning County (that contains Youngstown) and Hamilton County (that contains Cincinnati). Interestingly, higher soil Pb concentrations did not necessarily correlate with EBLL where soil was the only detected hazard, indicating that other sources were likely contributing to those cases.
Many of the variables linked to hotspots in the current analysis are also considered as risk factors by ODH (i.e., home age, deteriorated paint, and income level), which provides confidence in the results. OH law requires blood Pb testing for children at ages 1 and 2 years under any of the following circumstances (1) child is on Medicaid; (2) child lives in a zip code distinguished by ODH; (3) child lives or regularly visits a home, child care facility or school built before 1950; (4) child lives or regularly visits a home, child care facility or school built before 1978 that has deteriorated paint; (5) child lives or regularly visits a home, child care facility or school built before 1978 that has recent ongoing or planed renovation/remodeling; (6) child has sibling or playmate that has EBLL; (7) child comes into contact with an adult who has a hobby involving Pb or works with Pb; and (8) child lives near an active or former Pb smelter, battery recycling plant or other industry known to generate airborne Pb dust [30].
The ODH targeted testing plan for Pb screening shows that housing built before 1950, population of non-Hispanic African Americans, population with a high school education, families whose income-to-poverty ratio was greater than two, and population under the age of 6 years were the most significant predictors of EBLL at the census tract scale [18]. This was consistent with earlier work to develop a Pb risk indicator at the census tract scale for OH using 1997 BLL data, which included housing built before 1950, residents of non-Hispanic African American ethnicity, residents with less than a high school diploma, and housing units that are renter-occupied in the final model [31]. Both populations of non-Hispanic African Americans and populations with less than a high school education were much more likely to reside in an identified hotspot (by four or two times, respectively) in our analysis, providing further confirmation of prior findings. These EJ-related indicators appear to be stable over time, with BLL data from the latest analysis highlighting the same variables as those identified over 20 years ago.
LSLs in drinking water distribution systems can be a potential source of household Pb exposure and contributor to children’s EBLL. Although a comprehensive inventory of LSLs across the U.S. does not exist, estimates have been calculated based on individual community water system (CWS) surveys. The midwestern U.S. has the largest share of LSLs, representing over half of those in the entire U.S., with OH and Illinois estimated to have the greatest number of LSLs in the region [32]. Housing age has also been linked to LSL prevalence, with greater percentage of older housing (pre-1960) related to increased percentage of water systems with LSLs [32]. Thus, older housing as an identified risk factor in this region could reflect both presence of Pb-based paint and LSLs.
In the analysis for OH, more census tracts in rural areas away from major metropolitan areas were identified with the top 20th percentile approach than the Getis-Ord Gi* approach. This is consistent with the top 20th percentile results from MI, where 44% of the census tracts with EBLL did not overlap with the hotspots identified using Getis-Ord Gi* and generally were in more rural locations. There were 102 OH census tracts that were not included in the EBLL geospatial analysis, most of which were in urban areas (73 urban, 19 rural, 10 neither). While some rural census tracts were identified with our methodology, it is possible that children in these communities are not regularly screened for blood Pb, resulting in bias toward urban areas. Further evidence may be provided in the OH childhood blood Pb testing requirements [30] that specify high-risk zip codes where screening is mandatory; there are seven OH counties that do not have zip codes on this list (Adams, Fulton, Highland, Jackson, Paulding, Pike, and Union) and six of these are considered “rural”Footnote 2 based on the 2020 CensusFootnote 3. Prior work from ODH demonstrated that both Carrol County and Morrow County (classified as rural by the U.S. Census BureauFootnote 4) had high observed probabilities and low predicted probabilities of BLL ≥ 5 µg/dL in logistic regression modeling that included a limited number of BLL samples from rural areas [18].
As shown by the urban/rural categorization, the geospatial hotspot approach is better at detecting urban communities of multiple census tracts where housing age is more homogenous. Older housing is found in greater quantities in urban areas of OH, with 89% of units build prior to 1980 and over 57% built before 1950 [17]. A study in Toledo, OH reported age of housing as a key indicator for children’s BLL > 5 µg/dL in the urban core but was not a strong indicator for more rural areas [33].
By visual inspection, the high BLL zip codes specified by ODH in their blood Pb screening criteria [30], contain nearly all the Pb hotspots identified using our geospatial approach, including the largest cities of Cleveland and Toledo. The mapped results from the Pb indices/models compared well with EBLL data using 3.5 µg/dL at the threshold for these two cities, as well as Youngstown, Mansfield, Springfield, Elyria, and Canton. Thus, old housing and demographics are good predictors of Pb exposure in these cities and in the absence of any measured blood Pb data, these tools could be used to target education or mitigation efforts.
In contrast, the reference locations of Troy and East Liverpool that collectively contain nearly 20 census tracts and over 5000 children aged 0 to <6 years were not identified in maps produced from the Pb indices/models. The zip codes containing Troy and East Liverpool are included as high risk by ODH that require blood Pb testing for young children who reside in these areas [30]. In these communities, sources of Pb exposure are not readily explained by housing age, race/ethnicity, or income variables in our analysis, suggesting that community wide environmental Pb sources or other risk factors may be contributing. One possibility is exposure from Pb ammunition, which has been shown to result in high soil Pb concentrations [34] and elevated EBLL [35], including at firing ranges. Take-home Pb dust adhered to shooters may result in a residential exposure pathway for children [34, 35] that would not be captured herein. It is noteworthy that ODH does include casting ammunition as a listed hobby for adults who are in frequent contact with children less than 6 years of age on their survey instrument for required blood Pb testing [30]. Non-environmental sources could also be contributing, particularly for refugees who settled in OH and were exposed to Pb prior to immigration [36]. While the existing Pb indices/models do relatively well to predict census tracts containing a few key Pb exposure determinants (largely in urban areas), there will be locations containing differing Pb risk factors that will prohibit identification. Without widespread investigation or a comprehensive screening program, it could be challenging to identify children in these communities who are at increased risk for blood Pb levels above CDC reference values.
The statistical agreement between the Pb indices/model and OH EBLL hotspot data in this study ranged between 0.54 and 0.64, with the Schultz et al. [24] model having the highest kappa value. Both EJ Screen Pb Paint EJ index and the HUD DPI had weaker agreement with the observed OH data (kappa = 0.58 and 0.54, respectively), demonstrating that the Schultz et al. [24] regression model derived with BLL measurements was a better predictor of hotspots despite being developed using data from other states. It is also noteworthy that the HUD DPI is a household-level predicted risk metric for homes that may contain large areas of peeling paint [14], and not intended specifically for identifying EBLL hotspots for young children. When the same comparison between the Pb indices/model was done for MI EBLL hotspots (albeit using 5 µg/dL for the blood Pb reference value), kappa values were quite similar (i.e., between 0.54 and 0.55) [15]. Possible explanations for the slightly higher kappa values for OH may be more census tracts being included for EJSCREEN and Schultz et al. [24] and the lower threshold for the blood Pb reference value. Regardless, the findings for OH and MI are consistent and provide evidence that many locations of potential Pb exposure can be identified using these approaches.
Our results suggest that the generalizable methodology previously developed [15] is helpful to inform further investigation and other actions in response to potential high-risk Pb exposures for children living in hotspots in OH. The successful application of the approach and the moderate agreement with public Pb indices (i.e., EPA EJ SCREEN Pb paint EJ Index and HUD DPI) provide additional confidence that these indices can be used in the absence of sufficient available blood Pb testing data to screen for potential Pb exposure risk [37]. This brings us closer to having a consistent approach (i.e., whole-of-government systematic roadmap or blueprint as described in [14]) that can be applied on the national scale or state-specific scale to target those areas where Pb continues to be problematic. However, census tracts affected by environmental sources that are not associated with housing age or demographics will likely not be identified by these indices.
Universal blood Pb testing can inform targeted actions to help children after they are exposed and identify places needing more attention; surrogate Pb indices can inform preventative efforts before exposure occurs. For states with robust and representative BLL data at the community scale, investigations to pinpoint Pb hazards and on-the-ground knowledge of contamination or other risk factors could provide insight into exposure drivers. Future work could enhance existing statistical methodologies by incorporating environmental sources to this approach that can be applied in states without extensive BLL data.
Inequities in EBLL prevalence persist, despite the progress in reducing sources of Pb exposure. Non-Hispanic African American, less than a high school education and income less than two times the federal poverty level are indicators of much greater risk of residing in an identified hotspot in both OH and MI. It is important to recognize that these overlapping characteristics are often found in environmental justice communities who experience disproportionate and cumulative exposures that may magnify the health impacts from Pb. OH has prioritized testing for Pb exposure, particularly for those children in high EBLL prevalence communities and of low income [38]. Continued and expanded screening for BLL is essential for mapping and targeting high Pb exposure risk locations and exposure disparities and for tracking progress as the U.S. strives to achieve primary and secondary prevention of Pb exposure [11].



留言 (0)