
記住我





Sarcopenia is characterized by the progressive loss of skeletal muscle mass and strength, which can have a negative impact on patients' quality of life, physical function, and overall health.8 The underlying causes of sarcopenia remain unclear, but contributing risk factors include unhealthy lifestyle habits, malnutrition, physical inactivity, and chronic illness.7 Sarcopenia can also affect the occurrence, progression, and prognosis of various diseases and increase the risk of falls, disability, hospitalization, and mortality.21 In addition, patients with sarcopenia are often older adults with limited physical function, which can increase their susceptibility to postoperative complications.9 Given these risks, it is crucial for surgeons and anesthesiologists to closely monitor and manage patients with sarcopenia during and after surgery to mitigate adverse outcomes.
Postsurgical pain is among the commonest adverse events after surgery. Chronic postsurgical pain (CPSP), which is triggered by surgery and lasts for more than 3 months, may occur if acute postoperative pain is not completely relieved.15 The pathogenesis of CPSP remains unclear. In addition to causing physical pain, CPSP can lead to multiple comorbidities, such as sleep disorders, pneumonia, immunosuppression, anxiety, and depression.19 Analgesics are often the first choice of treatment for CPSP. However, the long-term use of analgesics or opioids can cause stomach ulcers, liver damage, blood coagulation abnormalities, drug addiction, and cancer.16,20,24 Therefore, the prevention of CPSP and reduction of the long-term use of postoperative analgesic drugs are crucial goals.
The correlation between sarcopenia and long-term analgesic and opioid use after surgery under neuraxial anesthesia remains not fully understood, and studies with adequate sample sizes and clear definitions of sarcopenia are limited.18 Moreover, no study has investigated the incidence of CPSP and long-term analgesic use in patients with sarcopenia after surgery. Understanding the relationship between sarcopenia and long-term analgesic use is essential, particularly in the context of older patients, who are more vulnerable to sarcopenia. This knowledge is pivotal for tailoring effective pain management strategies while minimizing the potential risks associated with prolonged analgesic, including opioids, use. By investigating this connection, health care providers can achieve a delicate balance between pain relief, improved patient quality of life, and optimized resource allocation. Moreover, given the potential variations in long-term analgesic use between neuraxial and general anesthesia,32 a comprehensive study using real-world data is imperative to explore this complex relationship. To bridge this knowledge gap, we conducted a comparative analysis using propensity score matching (PSM) to evaluate the influence of preoperative sarcopenia on long-term analgesic and opioid utilization in patients undergoing surgery under neuraxial anesthesia, ultimately shedding light on its impact on CPSP development.
2. Patients and methods 2.1. Data sourceData from Taiwan's National Health Insurance Research Database (NHIRD) from January 1, 2016, to December 31, 2019, were used in this study. The follow-up period for patients extended until December 31, 2020. In addition, there was no loss to follow-up within the scope of our study. The Taiwan NHIRD provided comprehensive data until the end of 2020. The NHIRD includes registration and original claims data for all NHI beneficiaries, totaling approximately 27.38 million individuals. To ensure patient privacy, all NHIRD data are encrypted and contain comprehensive outpatient and inpatient claims information, including patient identification numbers, birth dates, sex, diagnostic codes based on the International Classification of Diseases (ICD-9-CM and ICD-10-CM), treatment information, medical costs, dates of hospital admission and discharge, and dates of death.24,25 Patient identification numbers were used to link all data sets.
2.2. EthicsEthical approval for this study (Ethical Committee Tzu-Chi Medical Foundation) was provided by the Ethical Committee Tzu-Chi Medical Foundation, Taiwan (Chairperson Prof Chien-Hsing Wang), on 12 May 2021. The study protocols were reviewed and approved by the Institutional Review Board of Tzu-Chi Medical Foundation (IRB109-015-B). Patient consent was waived because data files are deidentified by scrambling the identification codes of both patients and medical facilities and sent to the National Health Research Institutes to form the original files of NHIRD. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. This study used retrospective data from Taiwan's NHIRD, a comprehensive source of patient information. Owing to its observational nature and reliance on existing data, preregistration was not pursued.
2.3. DesignThis retrospective population-based case–control analysis focused on patients who underwent elective surgeries under neuraxial anesthesia between January 1, 2016, and December 31, 2019. This study aimed to explore the potential relationship between sarcopenia and long-term analgesic use after surgery. The surgeries included herniorrhaphy, hip and knee replacements, lower-limb open reduction internal fixation, and lower-limb amputation, chosen for their suitability for neuraxial anesthesia. Patient eligibility for neuraxial anesthesia was determined based on a set of established criteria. These criteria encompassed factors such as the type of surgical procedure, patient suitability, informed consent, thorough preoperative assessments, careful monitoring during surgery, comprehensive documentation, and postoperative care. By adhering to these criteria, health care professionals ensured that neuraxial anesthesia was applied when most appropriate and beneficial, considering both patient safety and surgical efficacy. The anesthesia type was ascertained using the corresponding payment code in Taiwan's NHIRD.32 To eliminate the influence of underlying chronic pain and pain from other sources, patients who used analgesics, opioids, or nonopioids for more than 1 month before surgery were excluded. Patients with cancer that may have significantly affected their recovery from surgery or cancer-related pain were also excluded. Patients who passed away within 6 months of surgery were excluded, and the surgeries were performed until December 31, 2019, with follow-up until the end of 2020. The index date was the day of surgery.
In October 2016, the formal recognition of sarcopenia as a disease and its classification as M62.84 in ICD-10-CM was announced by the US Centers for Disease Control and Prevention.1 The diagnosis of sarcopenia in our study adhered to the ICD-10-CM code,25 which was established after 2016. We used a criterion of at least 2 claims for patients with a principal diagnosis of sarcopenia within the 12-month preoperative period to diagnose sarcopenia.6 The coding of sarcopenia in our study was based on a previous research investigation. The definition of sarcopenia was a skeletal muscle mass index (SMI) that was 2 or more standard deviations below the mean values of young individuals of the same sex. Computed tomography images provided the relevant measurements, and the SMI was calculated using the following formula: SMI = L3 skeletal muscle cross-sectional area (cm2)/height2(m2).30 Sarcopenia diagnoses made by orthopedic physicians, rehabilitation physicians, family medicine specialists, and geriatricians were included in the sarcopenia group.
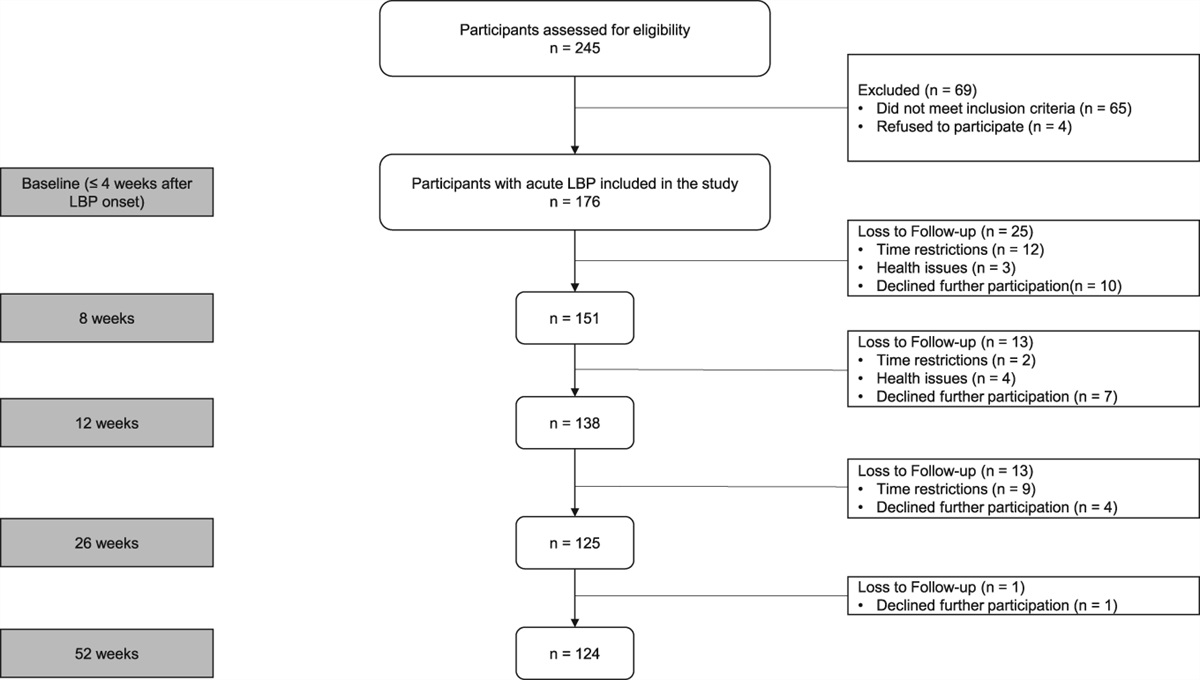
The study size in our research was determined based on the retrospective available data within the Taiwan NHIRD over the specified timeframe, in accordance with our inclusion and exclusion criteria. We have included a flow diagram that illustrates the patient selection process, including the number of patients at each stage, which provides clarity regarding our study size determination (Supplemental Figure 1, https://links.lww.com/PR9/A217).
2.4. Covariates and propensity score matchingAfter adjustment for potential confounding factors, a multivariable logistic regression model was used to analyze the use of analgesics 3 or 6 months after surgery under neuraxial anesthesia, comparing patients with and without preoperative sarcopenia. To reduce potential bias when comparing analgesic use between sarcopenia and nonsarcopenia groups, we used PSM to match all patients based on age, sex, surgery type, medical center level, American Society of Anesthesiology (ASA)–derived physical status, coexisting comorbidities, smoking status, alcohol-related diseases (ARDs), Charlson Comorbidity Index (CCI) score, and adapted Diabetes Complications Severity Index (aDCSI) score. We matched the cohorts using a 1:4 ratio and a caliper of 0.1,2 and comorbidities were identified using ICD-9-CM and ICD-10-CM codes in the main diagnosis records of inpatients, or with at least 2 outpatient visits within 1 year. Comorbidities that occurred 1 year before the index date were considered. The hospital accreditation level was also taken into account. Medical centers were defined as facilities with 1000 to 2500 beds, providing tertiary medical services and conducting most staff training within the center, as well as having research facilities, in accordance with the Taiwan Joint Commission on Hospital Accreditation.32 Owing to the comprehensive nature of the covariates in the Taiwan National Health Insurance Research Database (NHIRD), the occurrence of missing data was minimal, with all covariates containing less than 1% missing data. Consequently, patients with missing data in any of these covariates were excluded from the analysis to ensure data completeness and accuracy.
In our PSM study, we used methods to examine subgroups and interactions, including stratifying the study population into distinct subgroups based on specific covariates of interest for subgroup analysis. Interaction terms were incorporated into our regression models to formally test interactions between treatment variables and key covariates. Sensitivity analyses using different PSM techniques and caliper widths were performed to assess the robustness of our findings.10 Forest plots were created to visually present effect sizes and confidence intervals for different subgroups. Formal interaction tests based on interaction terms were conducted to assess the statistical significance of treatment–covariate interactions.34
Appropriate continuous variables are presented as means ± standard deviations. To minimize differences among participants, we used a PSM ratio of 1:4 for the preoperative sarcopenia and nonsarcopenia groups, which is commonly used to select controls with identical background covariates. To determine whether preoperative sarcopenia is an independent predictor of high rates of long-term analgesic use in surgical patients, a multivariable logistic regression model was used. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated by performing the multivariable logistic regression analysis. The analysis was conducted for all analgesics, including opioids.
2.5. OutcomesAs CPSP is pain that is specific to surgery and lasts for more than 3 months,15 we defined the primary outcome as the combined rate of analgesic prescriptions given 3 and 6 months after surgery. To be classified as a long-term analgesic user, patients needed to receive one or more prescriptions for analgesics, which included acetaminophen, nonsteroidal anti-inflammatory drugs, phenytoin, carbamazepine, pregabalin, gabapentin, and opioids, from outpatient clinics at 3 months or later after surgery. Those who were prescribed opioids such as morphine, fentanyl, oxycodone, buprenorphine, hydromorphone, tramadol, codeine, and meperidine were classified as long-term opioid users.32
2.6. StatisticThe descriptive findings pertaining to age, sex, surgery type, medical center level, ASA-derived physical status, coexisting comorbidities, smoking status, ARDs, CCI score, and aDCSI score were presented as absolute frequencies with percentages, while standardized differences were used to evaluate the baseline information between the 2 groups. The potential confounders linked to the occurrence of persistent analgesic use were considered as covariates in the predicted model to explore the association between the sarcopenia and nonsarcopenia groups that underwent elective surgery under neuraxial anesthesia. Despite applying PSM using SAS PROC PSM, the residual imbalance might still persist in a population due to a large sample size33; hence, we used multivariable logistic regression with SAS PROC LOGISTIC to assess the probability of long-term analgesic use between the groups by estimating adjusted ORs (aORs) and 95% CIs. All statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc, Cary, NC).
3. Results 3.1. Study cohortThis study analyzed data from 3805 surgical patients undergo neuraxial anesthesia, with 761 in the sarcopenia group and 3044 in the nonsarcopenia group. Table 1 presents their characteristics, including age, sex, surgery type, medical center level, ASA-derived physical status, coexisting comorbidities, smoking status, ARD, CCI score, and aDCSI score. After PSM, there were no significant differences in these characteristics between the groups. The 3-month analgesic and opioid prescription rates were higher in the sarcopenia group compared with the nonsarcopenia group, with rates of 62.3% and 57.1% (P = 0.009) and 2.9% and 0.8% (P = 0.014), respectively. Similarly, the 6-month analgesic and opioid prescription rates were also higher in the sarcopenia group, with rates of 30.8% and 26.3% (P = 0.013) and 1.7% and 0.3% (P = 0.030), respectively (Table 1).
Table 1 - Demographic characteristics of patients receiving elective surgery under neuraxial anesthesia, grouped according to the presence of sarcopenia (after propensity score matching). Nonsarcopenia Sarcopenia SMD N = 3044 N = 761 N % N % Age Age (mean ± SD) 64.14 ± 15.94 64.07 ± 15.86 0.0040 Age, median (IQR), y 67.00 (56.00, 75.00) 67.00 (55.00, 76.00) Age group, y 0.0190 <30 131 4.3% 34 4.5% 30–50 398 13.1% 102 13.4% 51–70 1,287 42.3% 315 41.4% >70 1,228 40.3% 310 40.7% Sex −0.0020 Female 1,586 52.1% 395 51.9% Male 1,458 47.9% 366 48.1% Surgery type 0.0340 Herniorrhaphy 723 23.8% 182 23.9% Hip replacement 130 4.3% 36 4.7% Knee replacement 845 27.8% 207 27.2% Lower-limb ORIF 1,284 42.2% 318 41.8% Lower-limb amputation 62 2.0% 18 2.4% Medical center 0.0039 No 2,332 76.6% 586 77.0% Yes 712 23.4% 175 23.0% ASA-derived physical status 0.0180 1 670 22.0% 167 21.9% 2 435 14.3% 107 14.1% 3 1,525 50.1% 379 49.8% 4 414 13.6% 108 14.2% Coexisting comorbidities Dysthymic disorder 304 10.0% 76 10.0% 0.0000 Peripheral vascular diseases 244 8.0% 61 8.0% 0.0000 Osteoporosis 760 25.0% 190 25.0% −0.0667 Gout 561 18.4% 180 23.7% −0.0522 Headache 1292 42.4% 323 42.4% 0.0000 Diabetic neuropathy 176 5.8% 49 6.4% −0.0066 Rheumatoid arthritis 150 4.9% 51 6.7% −0.0177 Pressure ulcer 82 2.7% 29 3.8% −0.0112 Current smoking 72 2.4% 27 3.6% −0.0118 ARD 143 4.7% 45 5.9% −0.0122 CCI score Mean (SD) 0.79 ± 1.17 0.81 ± 1.20 0.0220 Median (Q1–Q3) 0.00 (0.00, 1.00) 0.00 (0.00, 1.00) CCI Score −0.0028 0 1,812 59.5% 452 59.4% ≧1 1,232 40.5% 309 40.6% CCI Congestive heart failure 226 7.4% 48 6.3% 0.0112 Dementia 99 3.3% 30 3.9% −0.0069 Chronic pulmonary disease 550 18.1% 146 19.2% −0.0112 Rheumatic disease 30 1.0% 14 1.8% −0.0085 Liver disease 375 12.3% 99 13.0% −0.0428 DM with complications 224 7.4% 56 7.4% 0.0000 Hemiplegia and paraplegia 0 00.0% 0 0.0% 0.0000 Renal disease 165 5.4% 44 5.8% −0.0036 AIDS 0 0.0% 0 0.0% 0.0000 aDCSI score Mean (SD) 0.54 ± 1.24 0.60 ± 1.39 0.0460 Median (Q1–Q3) 0.00 (0.00, 0.00) 0.00 (0.00, 0.00) aDCSI score 0.0440 0 2,320 76.2% 577 75.8% 1 303 10.0% 70 9.2% 2 192 6.3% 49 6.4% ≧3 229 7.5% 65 8.5% aDCSI Retinopathy 110 3.6% 38 5.0% −0.0138 Nephropathy 223 7.3% 61 8.0% −0.0069 Neuropathy 170 5.6% 43 5.7% −0.0007 Cerebrovascular disease 149 4.9% 35 4.6% 0.0030 Cardiovascular disease 378 12.4% 108 14.2% −0.0177 Peripheral vascular disease 117 3.8% 31 4.1% −0.0023 Metabolic disease 20 0.7% 6 0.8% −0.0013 Outcomes 3-mo analgesic prescription 0.009 No 1,307 42.9% 287 37.7% Yes 1,737 57.1% 474 62.3% 3-mo opioid prescription 0.014 No 3,021 99.2% 739 97.1% Yes 23 0.8% 22 2.9% 6-mo analgesic prescription 0.013 No 2,243 73.7% 527 69.3% Yes 801 26.3% 234 30.8% 6-mo opioid prescription 0.030 No 3,035 99.7% 756 99.3% Yes 9 0.3% 13 1.7%aDCSI, adapted Diabetes Complications Severity Index; AIDS, acquired immune deficiency syndrome; ARD, alcohol-related disease; ASA, American Society of Anesthesiology; CCI, Charlson Comorbidity Index; IQR, interquartile range; N, number; ORIF, open reduction internal fixation; SMD, standardized mean difference.
To evaluate the rate of long-term analgesic use between sarcopenia and nonsarcopenia patients undergoing neuraxial anesthesia, we examined outpatient clinical records and postoperative analgesic usage for 6 months after surgery. The aORs and corresponding 95% CIs of 3-month analgesic and opioid use for the sarcopenia and nonsarcopenia groups undergoing elective surgery are presented in Tables 2 and 3. The rate of analgesic prescription was significantly higher in the sarcopenia group than in the nonsarcopenia group 3 months after surgery (aOR, 1.27; 95% CI, 1.05–1.52; Table 2). After adjusting for potential confounding factors, including age, sex, surgery type, medical center level, ASA-derived physical status, coexisting comorbidities, smoking status, ARD, CCI score, and aDCSI score, the aORs (95% CIs) of 3-month analgesic use for patients aged 51 to 70 years, those aged older than 70 years, those who underwent hip replacement, and those who underwent knee replacement were 2.07 (1.42–3.02), 2.04 (1.37–3.04), 7.12 (6.47–16.55), and 8.58 (5.82–16.77), respectively, when compared with patients aged younger than 30 years and those who underwent herniorrhaphy (Table 2).
Table 2 - Logistic regression model of analgesic prescription 3 months after surgery under neuraxial anesthesia. 3-mo analgesic prescription Crude OR (95% CI) P Adjusted OR* (95% CI) P Sarcopenia Nonsarcopenia (ref.) Sarcopenia 1.24 (1.06, 1.46) 0.0091 1.27 (1.05, 1.53) 0.015 Age group, y (ref. < 30 y) 30–50 1.37 (0.96, 1.96) 0.0551 1.61 (1.09, 2.37) 0.969 51–70 2.15 (1.55, 2.98) <0.0001 2.07 (1.42, 3.02) 0.001 >70 2.21 (1.6, 3.07) <0.0001 2.04 (1.37, 3.04) 0.005 Sex (ref. = female) Male 0.42 (0.37, 0.48) <0.0001 1.04 (0.87, 1.24) 0.669 Surgery types (ref. = herniorrhaphy) Hip replacement 11.52 (7.85, 16.91) <0.0001 7.12 (6.47, 16.55) 0.001 Knee replacement 20.18 (16.03, 25.41) <0.0001 8.58 (5.82, 16.77) <0.001 Lower-limb ORIF 6.52 (5.38, 7.89) 0.1031 7.40 (5.96, 9.2) 0.092 Lower-limb amputation 4.23 (2.65, 6.76) 0.0923 6.54 (3.68, 11.64) 0.944 Medical center (ref. = nonmedical center) Medical center 0.76 (0.66, 0.89) 0.000 0.84 (0.71, 1.01) 0.062 ASA physical status (ref. = 1) 2 1.27 (1.02, 1.58) 0.5202 1.01 (0.76, 1.32) 0.279 3 1.80 (1.53, 2.12) <0.0001 0.93 (0.73, 1.19) 0.744 4 1.38 (1.1, 1.71) 0.6634 1.14 (0.54, 1.22) 0.332 CCI (ref. = 0) 1.08 (0.95, 1.23) 0.2405 1.08 (0.9, 1.29) 0.412 ≧1 1.08 (0.95, 1.23) 0.2405 1.08 (0.9, 1.29) 0.412 aDCSI (ref. = 0) 1 1.28 (1.03, 1.6) 0.1024 1.01 (0.78, 1.33) 0.137 2 1.23 (0.94, 1.61) 0.321 0.76 (0.55, 1.05) 0.288 3 0.94 (0.74, 1.2) 0.1025 0.73 (0.51, 1.03) 0.170 Coexisting comorbidities
留言 (0)