
記住我





Chronic pain is a common condition in the general population and is often associated with other diseases but could also be a disorder of its own with a multifactorial background. This is especially the case when chronic pain is widespread in the body. This view on chronic widespread pain has also been implemented in the latest 11th revision of the International Classification of Diseases (ICD-11).
Chronic widespread pain (CWP) has previously and most commonly been defined as included in the ACR1990 criteria for fibromyalgia. This definition requires pain for at least 3 months in the left side and right side of the body, above and below the waist, and in the axial skeleton. In addition, for fibromyalgia, pain must be present in at least 11 of 18 specified tender points on digital palpation.22 The ACR1990 definition of CWP has been criticized for being too including, and updated versions of the CWP definition have been proposed.18–20 The most recent of these definitions, the WP2019,18 requires that pain must be present for at least 3 months in 4 of 5 main pain regions: the upper and lower quadrants of the body and the spine. The 5 main pain regions is further divided into 3 pain sites, and pain must be present in at least 7 of these 15 pain sites. The requirement of 4 of 5 regions is also consistent with the definition of CWP in ICD-11.
The prevalence of CWP in the general population based on the ACR1990 criteria vary in the literature, with most measures in the range of 10% to 15%.11 A prevalence of 11.4% has previously been reported from the EPIPAIN cohort,4 the base for the study in this article. Pain for at least 3 months not fulfilling CWP criteria is usually referred to as chronic regional pain (CRP), with a prevalence of 23.9% in the EPIPAIN cohort.4 In terms of the WP2019 definition, the prevalence of CWP and CRP in the population is yet to be investigated.
Chronic widespread pain defined according to ACR1990 is more common in the female population4,11,16 and amongst elderly adults.4,11 Also, socioeconomic status4,11 and sleep disorders1,6 are associated to CWP. Factors associated to CWP defined according to WP2019 remain to be studied.
Previous studies have suggested that people with CWP have an excess mortality,5,9,10 because of not only cardiovascular diseases9,13,14,17 and malignant tumors9,12,13 but also pulmonary diseases,7,9 and chronic kidney disease.23 There are also diverging results, showing no excess mortality.2,3 Definitions of CWP, and if the results are controlled for different confounders, varies between studies, making direct comparisons difficult. It is also yet to be investigated how the more stringent WP2019 definition compares with the ACR1990 definition regarding excess mortality and certain causes of death.
The aim of this study was to determine whether overall mortality and known common causes of death (neoplasms and diseases of the circulatory system) were increased among people with CRP and CWP in a 25-year follow-up of a cohort of general population. In addition, to find out whether the definition of CWP, according to ACR1990 or WP2019, influenced these outcomes.
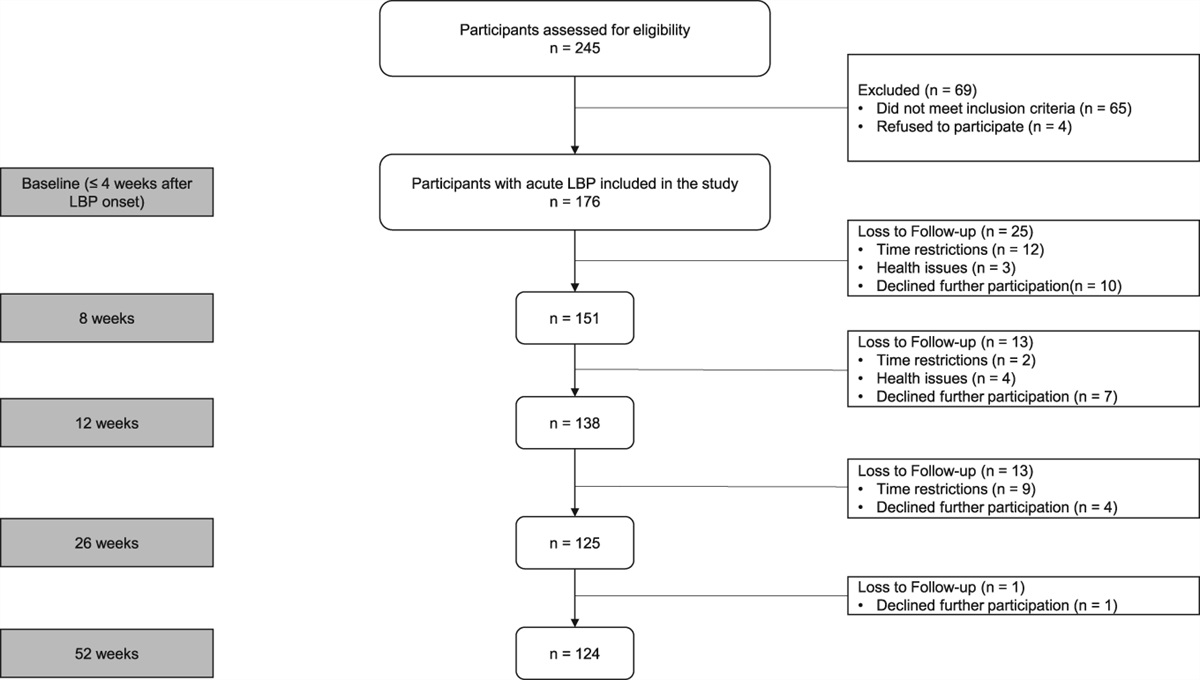
2. Materials and methods 2.1. Study population and study designThis longitudinal cohort study is based on baseline data from the EPIPAIN postal survey in 1995 and a 25-year follow-up of mortality data from the Swedish national registry. The EPIPAIN cohort is based on a representative sample of 3928 persons from the general population in southwest of Sweden. Based on the digital population register, a questionnaire was mailed to every 18th male and female aged 20 to 74 years in 2 municipalities (population 70 704). The 2425 persons who answered the postal survey in 1995 constitute the study cohort. Data from all participants was sent to the Swedish National Board of Health and Welfare and linked to the National Cause of Death Register.
2.2. CovariatesThe EPIPAIN questionnaire had a focus on chronic pain with a pain mannequin for registration of pain experience in 18 predefined areas,4 but it also included questions regarding sociodemographic factors and lifestyle habits. Chronic pain (duration for at least 3 months during the last year) at baseline in 1995 was the main explanatory variable in this study. Based on the pain mannequin, pain was classified as CWP, CRP, or no experience of chronic pain (NCP). Both the ACR1990 and the WP2019 classifications were used, giving 2 sets of 3 pain groups: (1) CWPACR1990, CRPACR1990, and NCPACR1990 and (2) CWPWP2019, CRPWP2019, and NCPWP2019. There was no attempt to classify the CWP subgroup fibromyalgia because this would have required tender point count (ACR1990)22 or a more extensive questionnaire.18
Age, sex, smoking habits, and socioeconomic status were included as cofactors or confounders. Smoking habits at inclusion were divided into 3 groups: never smoking, previous smoking, and smoking.
Based on occupation at inclusion, socioeconomic status was classified according to the Swedish socioeconomic classification system15 and divided into 4 groups: intermediate/higher nonmanual employees, assistant nonmanual employees, manual workers, and other. The group other included self-employed, farmers, housewives, and students.
The follow-up time was from baseline, June 1, 1995, to end of the study (May 31, 2020) or until the participant died.
2.3. Main outcome variableMain outcome variable was cause of death, derived from the National Cause of Death Register at the Swedish National Board of Health and Welfare, classified according to International Classification of Diseases (ICD-9 and ICD-10). This register gives a full coverage of all deaths in Sweden, including information on cause and date of death. A translation table from the National Board of Health and Welfare was used to convert the ICD-9 codes into ICD-10 codes. Eighteen of the deaths were not coded in the register or had incorrect codes and were set as “unknown.”
Causes of death were divided into primary and contributing causes of death. Causes of death were then divided into chapters and blocks according to ICD-10. Results are presented separately for primary causes of death and for total causes of death (including both primary and contributing causes). The focus in this study was on neoplasms and diseases of the circulatory system, but all causes of death in the study population were included in the analyses.
2.4. Statistical methods and analysesChi-square tests were used to test for differences in proportions between the groups. Cox regression analyses were used to analyze the primary outcomes, such as overall deaths and different causes of deaths, and their associations to pain group belonging (defined by ACR1990 or WP2019) controlled for age, sex, smoking habits, and socioeconomic status. Due to the small number of primary causes of death in some of the ICD-10 chapters and most of the blocks (subgroups within chapters), and because a contributing cause could be important, primary and contributing cause of death were combined in a secondary set of analyses. A threshold value of more than 50 study participants in an outcome was set to allow for 10 participants for each cofactor in the regression analyses. The time of survival was measured from the start of the study to the study participant deceased or until the study ended, giving a span from 0 to 25 years. The associations to the studied possible predictors are presented as hazard ratio (HR). IBM SPSS statistics version 26 was used to analyze the data. All tests were 2 tailed and conducted at the 0.05 significance level.
2.5. EthicsThis study was approved by the Regional Ethics Review Board Lund, Sweden (Dnr 2016/132). This provided the possibility to collect the information of deceased and the causes of death of the study participants from the National Board of Health and Welfare. All the data of the study participants were encrypted so that the data could not be traced back to the individual. The participants had at baseline given their written informed consent to participate in the study.
3. Results 3.1. Descriptive dataAt baseline there were a total of 2425 participants, 1132 (46.7%) male and 1293 (53.3%) female, with a mean (SD) age of 46.5 (15.4) years. The prevalence of CWP was 12.5% (n = 303) when defined according to the ACR1990 and 8.2% (n = 200) when defined according to WP2019. Corresponding prevalence of CRP was 24.2% (n = 599) and 28.3% (n = 686), respectively. The distribution of studied cofactors in relation to pain groups defined according to ACR1990 and WP2019 is presented in Table 1.
Table 1 - Demographic factors at baseline 1995 in relation to pain groups defined according to ACR1990 or WP2019. NCP CRP CWP Total ACR1990 % (n) % (n) % (n) % (n) Sex Male 49.7 (729) 46.3 (272) 31.4 (95) 46.5 (1096) Female 50.3 (737) 53.7 (316) 68.6 (208) 53.5 (1261) 100 (1466) 100 (588) 100 (303) 100 (2357) Age 20–33 30.7 (450) 19.9 (117) 9.9 (30) 25.3 (597) 34–46 24.9 (365) 23.8 (140) 19.5 (59) 23.9 (564) 47–58 22.8 (334) 27.6 (162) 32.7 (99) 25.2 (595) 59–74 21.6 (317) 28.7 (169) 38.0 (115) 25.5 (601) 100 (1466) 100 (588) 100 (303) 100 (2357) Socioeconomic status A 28.2 (413) 21.9 (129) 11.2 (34) 24.4 (576) B 13.8 (202) 13.3 (78) 15.2 (46) 13.8 (326) C 43.2 (634) 52.9 (311) 61.4 (186) 48.0 (1131) D 14.8 (217) 11.9 (70) 12.2 (37) 13.7 (324) 100 (1466) 100 (588) 100 (303) 100 (2357) Smoking habits Never 54.8 (797) 45.3 (264) 48.2 (145) 51.6 (1206) Previous 24.3 (353) 30.2 (176) 27.9 (84) 26.2 (613) Smoker 21.0 (305) 24.5 (143) 23.9 (72) 22.2 (520) 100 (1455) 100 (583) 100 (301) 100 (2339) WP2019 Sex Male 49.7 (729) 45.5 (312) 26.0 (52) 46.5 (1093) Female 50.3 (737) 54.5 (374) 74.0 (148) 53.5 (1259) 100 (1466) 100 (686) 100 (200) 100 (2352) Age 20–33 30.7 (450) 18.7 (128) 9.0 (18) 25.3 (596) 34–46 24.9 (365) 23.6 (162) 18.5 (37) 24.0 (564) 47–58 22.8 (334) 28.7 (197) 31.5 (63) 25.3 (594) 59–74 21.6 (317) 29.0 (199) 41.0 (82) 25.4 (598) 100 (1466) 100 (686) 100 (200) 100 (2352) Socioeconomic status A 28.2 (413) 21.1 (145) 8.5 (17) 24.4 (575) B 13.8 (202) 13.4 (92) 15.5 (31) 13.8 (325) C 43.2 (634) 53.6 (368) 63.5 (127) 48.0 (1129) D 14.8 (217) 11.8 (81) 12.5 (25) 13.7 (323) 100 (1466) 100 (686) 100 (200) 100 (2352) Smoking habits Never 54.8 (797) 46.2 (314) 45.5 (91) 51.5 (1202) Previous 24.3 (353) 29.5 (200) 29.5 (59) 26.2 (612) Smoker 21.0 (305) 24.3 (165) 25.0 (50) 22.3 (520) 100 (1455) 100 (679) 100 (200) 100 (2334)A = intermediate/higher nonmanual employees, B = assistant nonmanual employees, C = manual workers, D = other (self-employed, farmers, housewives, and students).
CRP, chronic regional pain; CWP, chronic widespread pain; NCP, no chronic pain.
A total of 608 (25.1%) out of 2425 study participants had died at the end of the study, 337 of the males and 271 of the females (29.8% vs 21.0%; P < 0.001), with a mean age of 77.6 years (males 75.9 vs females 79.7; P < 0.001).
Within the pain groups according to the ACR1990 definition, the unadjusted mortality was 21.4% in NCPACR1990, 28.8% in CRPACR1990, and 35.5% in CWPACR1990 (P < 0.001). With pain groups defined according to WP2019, the unadjusted mortality was 21.4% in NCPWP2019, 27.8% in CRPWP2019, and 39.5% in CWPWP2019 (P < 0.001). Cox regression analysis with death as outcome in relation to pain group according to the ACR1990 criteria showed no significant associations for CRPACR1990 (HR 1.05, P = 0.600) or CWPACR1990 (HR 1.08, P = 0.484) in relation to NCPACR1990, adjusted for age, sex, socioeconomic status, and smoking habits (Table 2 and Fig. 1). When pain groups were classified according to WP2019, there was a significant association for CWPWP2019 (HR 1.32, P = 0.033) but not for CRPWP2019 (HR 0.98, P = 0.860), adjusted for age, sex, socioeconomic status, and smoking habits (Table 2). Figure 1 displays the result visually as Kaplan–Meier curves for the different pain groups.
Table 2 - Cox regression analysis with hazard ratio for death during the 25-year follow-up time in relation to the 2 studied definitions of chronic widespread pain/pain groups. Pain group ACR1990 Pain group WP2019 Deceased*Cases with missing data, thus excluded from the analysis.
A = intermediate/higher nonmanual employees, B = assistant nonmanual employees, C = manual workers, D = other (self-employed, farmers, housewives, and students).
95% CI, 95% confidence interval; CRP, chronic regional pain; CWP, chronic widespread pain; HR, hazard ratio; NCP, no chronic pain.
 Figure 1.:
Figure 1.: Cumulative survival reported as a percentage of the total number of study participants in the analysis, 2339 for ACR1990, and 2334 for WP2019. Time in years is the follow-up time. Adjusted for age, sex, smoking habits, and socioeconomic status.
3.3. Primary and total cause of deathCause of death for all 608 deceased divided into chapters according to the ICD-10 codes is presented in Table 3. The most common causes were diseases of the circulatory system, neoplasms, and diseases of the respiratory system. Also, regarding total causes of death, including both primary and contributing causes of death, the major causes of death were within diseases of the circulatory system, neoplasms, and diseases of the respiratory system (Table 3).
Table 3 - All causes of death according to international classification of diseases-10 A00-Z99 codes. Causes of death, chapters according to ICD-10 codes A00-Z99 Primary cause of death Total cause of death n % N % A00-B99 certain infectious and parasitic diseases 12 0.5 44 1.8 C00-D48 neoplasms 204 8.4 231 9.5 D50-D89 diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism 2 0.1 13 0.5 E00-E90 endocrine, nutritional and metabolic diseases 16 0.7 71 2.9 F00-F99 mental and behavioural disorders 25 1.0 87 3.6 G00-G99 diseases of the nervous system 21 0.9 54 2.2 H00-H59 diseases of the eye and adnexa — — 2 0.1 I00-I99 diseases of the circulatory system 207 8.5 349 14.4 J00-J99 diseases of the respiratory system 38 1.6 136 5.6 K00-K93 diseases of the digestive system 16 0.7 43 1.8 L00-L99 diseases of the skin and subcutaneous tissue 2 0.1 12 0.5 M00-M99 diseases of the musculoskeletal system and connective tissue 5 0.2 20 0.8 N00-N99 diseases of the genitourinary system 8 0.3 67 2.8 Q00-Q99 congenital malformations, deformations,s and chromosomal abnormalities 2 0.1 2 0.1 R00-R99 symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified 14 0.6 158 6.5 S00-T98 injury, poisoning and certain other consequences of external causes 3 0.1 44 1.8 V01-Y98 external causes of morbidity and mortality 17 0.7 58 2.4 Z00-Z99 factors influencing health status and contact with health services — — 21 0.9 Unknown. Study participants without ICD-code, or with a nontranslatable ICD-9 code into ICD-10 16 0.7 20 0.8One column includes only the primary cause of death, and the other column includes both primary and cause of death as the total cause of death. The total study population was 2425 people.
ICD-10, international classification of diseases-10.
Cox regression analysis with all neoplasms (ICD-10 codes C00-D48) as the primary cause of death as outcome controlled for age, sex, smoking habits, and socioeconomic status, did not show any significant associations for the pain groups CRPACR1990 or CWPACR1990 in relation to NCPACR1990. Age, sex, and smoking showed significant associations (Table 4). Also, when the pain groups were classified according to WP2019, no significant associations were seen for CRPWP2019 or CWPWP2019, but age, sex, and smoking habits showed significant associations (Table 4). Figure 2 displays the result visually as Kaplan–Meier curves for the different pain groups.
Table 4 - Cox regression analysis with neoplasms as the primary cause of death according to international classification of diseases-10 codes over a 25-year follow-up time. Data from inclusion Pain group according to ACR1990 Pain group according to WP2019 C00-D48 as the primary cause of death*Cases with missing data, thus excluded from the analysis.
†Deceased because of other cause of death before the first participant deceased of the current cause of death, thus excluded from the analysis.
A = intermediate/higher nonmanual employees, B = assistant non-manual employees, C = manual workers, D = other (self-employed, farmers, housewives, and students).
95% CI, 95% confidence interval; CRP, chronic regional pain; CWP, chronic widespread pain; HR, hazard ratio; NCP, no chronic pain.
 Figure 2.:
Figure 2.: Survival function with neoplasms as the primary cause of death. Cumulative survival reported as a percentage of the total number of study participants in the analysis, 2339 for ACR1990, and 2334 for WP2019. Time in years
留言 (0)