
記住我





The life-time prevalence of sciatic (radiating) back pain caused by disk problems is up to 40%,14 and disk herniations most frequently occur between the age of 30 and 50 years.28 Surgery may effectively reverse pain and is considered a viable treatment option for those who do not respond to conservative (nonsurgical) treatment, yet the incidence of surgery varies greatly between countries.16 Surgical treatment for lumbar disk herniation (LDH) is common in adults but rare in adolescents because of low incidence, as it accounts for 0.8% to 2.8% of all LDH surgeries.10,16,23,24 Unfortunately, the point prevalence of LDH in youth is difficult to discern but is estimated to represent 0.5% to 3.8% of all disk protrusions and herniations.8 In contrast to adults with LDH, the aetiology in the paediatric population is related to trauma in up to 70% of the cases.15
Asymmetric gait is a prominent feature in symptomatic LDH, and this alteration can be reduced after surgery.27 It has been suggested that altered gait is a consequence of movement-restricting sciatic pain.4 Furthermore, Huang et al.13 found abnormalities of the trunk coordination in the walking patterns of individuals with LDH. The observed altered gait in these individuals is suggested to result from a chain of adaptations caused by long-term pain.13 This is supported by studies demonstrating that gait instability correlates with pain intensity in individuals with LDH,20 as well as reduced gait asymmetry after pain reduction among those with chronic lower back pain in general.26 To date, it is unclear if gait is related to back morphology, pain, and other health outcomes in LDH.
In a previous study, Lasselin et al.19 demonstrated that gait may serve as an important indicator of general health within individuals because levels of systemic inflammation were associated with altered gait. From this finding, it is possible that long-term degenerative processes after LDH can affect gait parameters in a similar fashion. Thus, walking speed and kinematic characteristics related to the spine, such as head and trunk angles, may potentially be related to objectively measurable spine degeneration, as well as general health measures.
The long-term effects of surgery for LDH in adults have previously been reported.1,6,9 Little is, however, known about the long-term effects of LDH surgery during adolescence. Lagerbäck et al.17 previously found that adolescents who underwent surgery for LDH had increased disk degeneration and worse health outcomes at an average of 13.8 years of follow-up when compared with controls. Whether increased degeneration was caused by the previous herniation, natural progression, or the surgery itself, could not be determined.
At mean 13.8-year follow-up, gait was collected for the analysis of movement related changes, presented for the first time in the present article. The aim of the present study was to compare gait outcomes between individuals who were surgically treated for LDH (“cases”) and age- and sex-matched individuals with no history of back pain (“controls”). We hypothesized that cases and controls would exhibit differential trunk18,22 and head angles19 because of degeneration of the lumbar spine, and related pain, within cases.
2. Materials and methods 2.1. Ethical approvalEthical approvals were obtained from the Ethical Review Board in Stockholm (number 2018/299-31/1 and 2019-01713), and the data collection was performed between May 2019 and January 2020. All participants gave written and oral consent. All assessments took place at the MR center at the Karolinska University Hospital, Stockholm, Sweden. Each participant's data were collected within the same date, whereby 2 cinema tickets were given for compensation.
2.2. ParticipantsCases (n = 23) were registered in the Swedish Spine register (SweSpine) and were 18 years old or younger when operated for LDH (M = 17.51, SD = 0.95, Min = 14.6, Max = 18.6). They had current residence within Stockholm County and were contacted by mail, whereby the time that passed between surgery and data collection was M = 13.8 years (SD = 3.1, Min = 8.6, Max = 20.4). Age- and sex-matched controls (n = 23) were recruited through advertisement in the Karolinska Institutet, the Karolinska University Hospital, and 3 private companies (1 in the mechanical industry and 2 in telecommunications). Exclusion criteria for controls included previous records of LDH or spinal surgery, as well as any contraindication for MRI.
2.3. Gait measuresGait can be defined as “a movement consisting of a translation of the whole body permitted by a repetition of movements of body segments while keeping the balance, [whereby] a gait cycle is divided […] in a period of stance phase [ie, the foot is in contact with the ground], and in a period of swing [ie, the foot is lifted and moved], of the lower limbs”].5 If any tissues or joints involved in gait are injured, eg, in LDH, movement efficiency can be expected to decrease as a result of the disturbance of these complex mechanisms.20 Microsoft Kinect is a depth camera technology, which tracks human gait by estimation of skeletal joint locations.7 Kinect is clinically useful to identify gait abnormalities and postural disorders, as well as for tracking progress within patient rehabilitation.3 Its suitability is mostly reported for gait discrimination of patients with and without Parkinson disease11,12 but is also used in stroke rehabilitation2 as well as in the context of cerebellar ataxia.7
This study used a similar protocol to the previous investigation of gait in systemic inflammation.19 We used the Microsoft Kinect for Windows (system v.1, Microsoft, Redmond, WA), the Microsoft Software Development Kit (v1.8), and Microsoft Visual Studio Express 2013 (Microsoft) to obtain 3-dimensional coordinates of skeletal joints during a walking paradigm. The walking procedure adhered to a standardized protocol with 2 walking trials, each walking trial included a minimum of 4 to 5 series, and each series consisted of one back-and-forth walk after a 5.5-m-long walking path (Fig. 1). Participants were instructed to walk as naturally as possible, while looking straight ahead. Gait parameters were calculated by a blinded assessor (coauthor J.L.), who was unaware of group allocation. For our analyses, the mean head and trunk angle across each individual trial was calculated (Fig. 2).
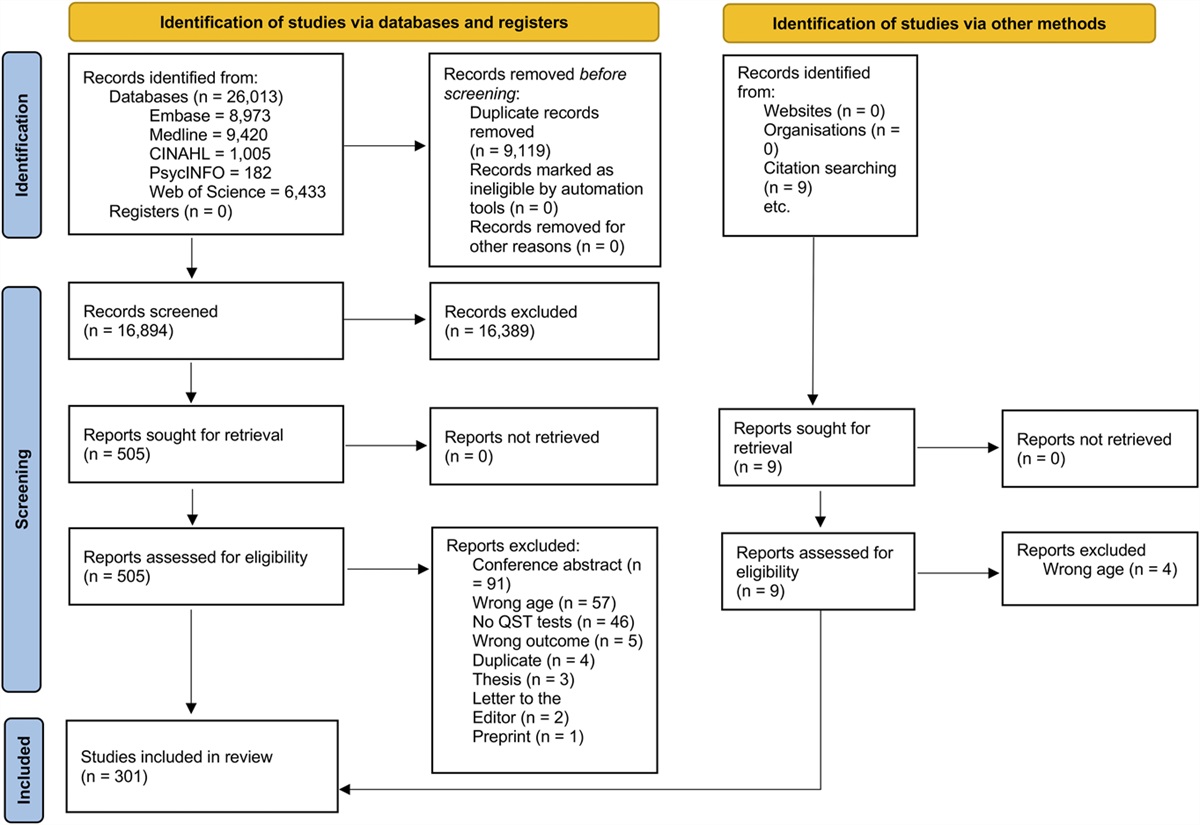
 Figure 1.:
Figure 1.: Study flowchart. Each group comprised 23 participants. Two subjects in each cohort (n = 4) did not take part in the walking test. Additionally, 2 control participants only had data from 1 or 3 series, respectively, because of technical issues. The remaining sample (n = 40) proceeded into gait analysis.
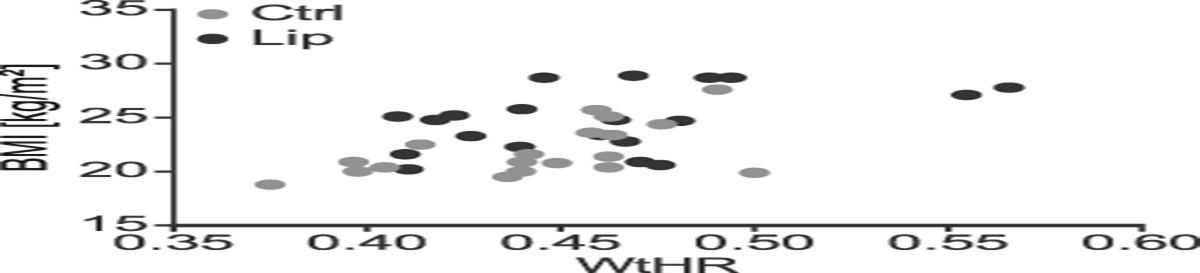
 Figure 2.:
Figure 2.: Head angle (left) and trunk angle (right) in cases (black) and controls (gray). Outcome measures related to gait were estimated by means of a Microsoft Kinect camera, tracking joint locations and estimating gait.
2.4. Lumbar back MRIImaging data were acquired with identical lumbar back sequences for all participants, using a 3.0-Tesla scanner (Discovery MR750; GE Healthcare, Chicago, IL) at MR-center, Karolinska University Hospital, Stockholm, Sweden. Images included sagittal T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences of the lumbar spine, using the surface coil implemented in the scanner bed. Disk degeneration was assessed with the morphologic and semi-quantitative Pfirrmann grading system. According to the Pfirrmann grading system, each segment was scored 1 (normal disk) to 5 (severe disk degeneration). The Modic system was used to determine changes in the vertebral endplate and body, it ranges from 0 (normal anatomical appearance with absence of Modic changes) to 3 (subchondral bony sclerosis). For each participant, the lumbar segments with Modic changes were counted to derive an indicator of overall vertebral endplate/body quality. The groups were compared for differences in Modic changes (present/not present) or Pfirrmann grading at level L4–L5 and L5–S1, which are most typically degenerated in LDH, and the sites of surgery among cases in this study. For the linear regression models, an average value of the Pfirrmann grading of L4–L5 and L5–S1 as well as the total number of segments of the lumbar spine with the presence of Modic changes were used as indicators for the degree of lumbar spine degeneration. Degenerative changes on level L5–S1 were not assessed for one surgically treated participant who had received fusion treatment at that location. Both Modic changes and Pfirrmann grading have sufficient intraobserver and interobserver reliability and were determined by an experienced radiologist (coauthor M.S.) who was masked to age, sex, and group assignment. To further reduce possible bias, the lumbar spine images were presented in a random order.
2.5. Questionnaire dataPatient-reported outcome measures were collected at the day of gait and MRI data acquisition. These included the Oswestry Disability Index (ODI), measuring disability because of back pain, and a visual analogue scale (VAS) measurement of perceived back and leg pain during the last week. These 3 parameters were missing for one participant in the control group. Furthermore, participants completed the EuroQol-5 Dimension-3 Levels (EQ-5D-3L) questionnaire, indicative for health-related quality of life, and the Short Form-36 health survey (SF-36), assessing health status. From the latter, the subscales (physical functioning, role limitations because of physical health, role limitations because of emotional problems, energy/fatigue, emotional well-being, social functioning, pain, and general health) were analyzed, as well as the overall mental and physical component summary scores were calculated.
2.6. Statistical analysisThe analyses of the present study followed a preregistered analysis plan (https://osf.io/36qxc). We hypothesised that cases, ie, participants with a history of LDH surgery in adolescence, would show significant differences in their gait parameters compared with controls. The analysis plan was preregistered within the scope of the parent study, a 3-armed MRI study including an additional participant group that had been conservatively treated because of a lumbar disk herniation in adolescence (with no Kinect data).
After drop-outs and data quality assurance (Fig. 1), the final sample consisted of 21 cases and 19 controls. These had between 4 and 13 walking series available for analyses, whereby no outliers were detected for head or trunk angle (< mean – 3.5 SD). This sample exhibited identical significant differences as previously reported by Lagerbäck et al.,17 except for a now significant difference in disk degeneration at the L4–L5 level, as measured by total endplate score (P = 0.032), previous P-value was P = 0.055.
First, group differences in pain and back degeneration, as well as in behavioural outcomes, were analysed using t-tests. They were one-sided as the cases were hypothesized to exhibit higher levels in pain and lower levels in mental and physical health measures as compared with the controls. The back-degeneration measures (Pfirrmann, Modic) were expected to be larger for the cases as compared with the controls as well. For the gait data, 1-sided tests were performed in the case of head angle because lower values have been previously shown to be associated with acute inflammation,12 whereas trunk angle was tested 2-sided because there was no hypothesized a priori directionality. The categorical variables asking about occupational strains, physical activity, and smoking habits were tested using Mann–Whitney tests.
Second, we analysed whether head and trunk angles were associated with any of the independent variables. Again, one-sided tests were used in the case of head angle because smaller angles, ie, larger deviation from 90°, were expected to be associated with more severe back degeneration as well as worse subjectively reported health outcomes (ie, lower physical/mental health according to SF-36, greater current back/leg pain, more disability according to ODI, and worse general health according to EQ-5D-3L). For the trunk angle, a possible association with any of these measures was exploratorily examined. Pearson correlation coefficients (r) were calculated for the questionnaire outcomes. For the MRI back-degeneration measures, ie, Pfirrmann grading and Modic changes at segment L4–L5 and at L5–S1, as well as Pfirrmann grading across both segments and number of lumbar spine segments with Modic changes, Spearman rank coefficients (Rs) were used.
To determine factors that explain variance in gait outcomes, both the factors “group” and “objective back degeneration,” ie, Pfirrmann grading across both lower segments and number of lumbar segments with Modic changes, as continuous variables, were added into hierarchical linear models, separated for head and trunk angle. As this part was an exploratory investigation without any clear a priori hypotheses, the other parameters to be included in these models were chosen based on their correlation coefficients with gait, or associated group differences. Before reporting the final model with best fit, all rejected models including the variables with nonsignificant variance will be reported stepwise.
3. Results 3.1. DemographicsThere were no significant group differences regarding age, height, weight, or BMI in the current study sample (Table 1). The sex distribution was comparable in the 2 groups. Additionally, participants in both groups showed similar physical activity levels, occupational strains, and smoking habits.
Variable Cases Controls P n = 21 n = 19 Sex Male 11 (52.4%) 9 (47.4%) Female 10 (47.6%) 10 (52.6%) Age 31. y (3.4) 31.2 y (3.6) 0.847 Height 177.6 cm (10.9) 174.4 cm (6.8) 0.269 Weight 76.5 kg (6.8) 73.2 kg (11.6) 0.398 BMI 24.2 kg/m2 (3.6) 24.0 kg/m2 (2.8) 0.792 Physical activity (this year) 0.838 High 13 (61.9%) 13 (68.4%) Moderate 6 (28.5%) 5 (26.3%) Low 1 (4.8%) 1 (5.3%) Missing data 1 (4.8%) 0 (0%) Occupational strains 0.259 Sedentary 12 (57.1%) 13 (68.4%) Mild strain 8 (38.1%) 3 (15.8%) Moderate strain 1 (4.8%) 1 (5.3%) Missing data 0 (0%) 2 (10.5%) Smoker 0.636 Yes 2 (9.5%) 1 (5.3%) No 15 (71.5%) 15 (78.9% Previous smoker 4 (19%) 3 (15.8%) Walking speed 1.4 m/s (0.1) 1.5 m/s (0.1) 0.638 Head angle 84.3° 89.7° 0.023 Trunk angle 88.2° 86.3° 0.008 VAS leg pain 8.8 (12.4) 3.8 (6.4) 0.066 VAS back pain 20.0 (20.8) 2.5 (3.9) 0.001 EQ5D index 0.81 (0.18) 0.96 (0.074) 0.001 ODI Score 12.7 (9.1) 1.5 (2.7) <0.001 SF-36 Physical score 49.4 (6.9) 56.5 (3.3) <0.001 SF-36 Mental score 49.0 (7.7) 49.9 (8.5) 0.73Displayed are the mean values (SD) and proportions (%).
EQ5D, EuroQol-5 Dimension; ODI, Oswestry Disability Index; SF-36, Short Form-36 health survey; VAS, visual analogue scale.
Among the 21 cases analysed, 12 were operated for LDH once, ie, only index surgery was performed. Nine participants had additional surgery (7 at index disk level and 2 at an adjacent level from index). Among these, 3 participants had a third surgery (2 at the index disk level and 1 at the same adjacent level from index). During the first LDH surgery, most of the cases were operated at the L5–S1 level (n = 15) as compared with the L4–L5 level (n = 6). As previously reported by Lagerbäck et al.,17 the prevalence of severe degeneration of the lumbar spine was higher for cases compared with controls at follow-up. Cases also had an overall worse health state, including lower health-related quality of life (EQ-5D), higher back pain ratings (VAS), more disability (ODI) and lower physical health (SF-36 physical component score) (Table 1).
3.3. Gait measuresThe head angle was on average 5.4° lower in cases (84.3°) compared with controls (89.7°; t (38) = −2.144, P = 0.021). Additionally, trunk angle was on average 1.9° higher in cases (88.2°) than controls (86.3°; t (38) = 2.788, P = 0.008). The groups showed no differences in their walking speed.
3.4. Associations between gait, back morphology, and questionnaire outcomesAcross groups, head and trunk angles showed a strong, negative association (r = −0.511, P < 0.001, 2-sided). In other words, individuals who had the head more tilting downward, had a straighter trunk. Additionally, head angle was positively correlated with the SF-36 physical component (r = 0.288, P = 0.036) and the SF-36 subscale role limitations due to physical health (r = −0.266, P = 0.048). In other words, a head that is more tilting downward is associated with decreased physical health and more disability because of according limitations in everyday life. From the self-reported measures of exercise, the amount of moderate exercise within the preceding week was correlated with both angle of the head (r = 0.300, P = 0.030) and trunk (r = −0.398, P = 0.011). However, trunk angle was not associated with any of the questionnaire or pain rating outcomes. The back-degeneration measures showed no significant association with gait, neither with head nor with trunk angle. Yet in case of a one-sided test, degeneration measures would be correlated with trunk angle, ie, the number of lumbar levels with Modic changes present (r = 0.306, P = 0.029), Pfirrmann grading at L5–S1 (r = 0.290, P = 0.043), and the average Pfirrmann grading across the lower levels L4–L5 and L5–S1 (r = 0.279, P = 0.037).
3.5. Hierarchical linear models of gaitTwo stepwise hierarchical modelling procedures were performed to assess parameters affecting head and trunk angles, respectively. First, age, sex, and BMI were included as covariates; however, none of these variables could explain any variance in gait and were therefore omitted.
Secondly, group was added at the first stage of both hierarchical models, which gave an adjusted R2 of 0.148 for trunk angle (∆F = 7.774, P = 0.008) and 0.077 for head angle (∆F = 4.255, P = 0.046).
Back-degeneration variables Pfirrmann across L4–L5 and L5–S1 and number of lumbar levels with Modic changes present were added at the second stage of the gait models. Taken together, these parameters did not yield any significant results and were therefore omitted (∆R2head = 0.020, ∆Fhead = 0.398, P = 0.675; ∆R2trunk = 0.004, ∆Ftrunk = 0.093, P = 0.911).
Questionnaire outcomes with significant differences between the groups were added in the second stage of the 2 models, as well as outcomes that demonstrated significant correlations with gait data (see above).
3.5.1. Head angleDespite previous correlations with gait, no significant variance could be explained by SF-36 physical component (∆R2 = 0.071, ∆F = 0.758, P = 0.390) nor the SF-36 subscale item role limitations because of physical health (∆R2 = 0.029, ∆F = 1.240, P = 0.273). The same applied to the parameters previously shown to differ between groups (see Appendix, https://links.lww.com/PR9/A225). However, back pain rating explained a significant amount of variance (∆R2 = 0.129, ∆F = 5.984, P = 0.019), beyond group.
3.5.2. Trunk angleIn line with the results for head angle, the outcome measures with significant differences between cases and controls did not explain a significant amount of variance (see Appendix, https://links.lww.com/PR9/A225). However, the self-reported moderate exercise in the preceding week (∆R2 = 0.083, ∆F = 4.128, P = 0.049) as well as the EQ-5D index (∆R2 = 0.102, ∆F = 5.185, P = 0.029) were found to explain a significant amount of variance. The final models can be found in Table 2.
Table 2 - Final hierarchical linear models of gait. Model R R 2 R 2 adj SE ∆R 2 ∆F df 1 df 2 P Head angle 1. Group 0.310 0.096 0.072 8.420 0.096 3.933 1 37 0.055 2. Group, back pain 0.474 0.225 0.182 7.904 0.129 5.984 1 36 0.019 Trunk angle 1. Group 0.412 0.170 0.148 2.188 0.170 7.774 1 38 0.008 2. Group, mod. exercise 0.503 0.253 0.213 2.103 0.083 4,128 1 37 0.049 3. Group, mod. exercise, EQ5D index 0.603 0.364 0.311 1.967 0.111 6.273 1 36 0.017Displayed is the model with best model fit for each of the dependent variables, ie, mean head and trunk angles across participants and trials.
EQ5D, EuroQol-5 Dimension.
We have previously reported that individuals who underwent surgery for LDH during adolescence had worse health-related quality of life, more pain, and increased disk degeneration at 13.8 years of follow-up compared with controls.17 To deepen the understanding of factors that contribute to the maintenance of persistent pain and disability, we analyzed the relationship between gait, back morphology, and other health outcomes in the same cohort of individuals treated surgically because of lumbar disk herniation, compared with controls.
4.1. GaitIn our initial between-group analysis, we found that the head and trunk angles, respectively, were different between cases and controls. It has previously been reported that individuals with untreated LDH have a different gait compared with healthy controls.4,20 However, the long-term effects of surgery on gait have not yet been demonstrated. We assessed gait on average 13.8 years after surgery for LDH. As predicted, cases in the present study had a reduced head angle, ie, head tilting more downward, compared with controls. This partly aligns with the findings by Lasselin et al., where sickness response to systemic inflammation was associated with altered mean head angles as well, although not trunk angle.19 In our study, cases had a more upright gait (higher trunk angle), which could reflect rigidity because of postural compensation for earlier lumbar disk herniation or possibly a higher degree of current disk degeneration. Additionally, the gait differences could be side effects of the surgical procedure itself because it is an invasive procedure that may have long-term effects. This could be investigated further by comparing the current findings with gait from a cohort of individuals who received nonsurgical treatment for LDH in adolescence. Taken together, these findings may act as a subtle marker of residual symptoms or consequences from surgery.
In contrast to our hypothesis, which was based on the study of gait changes during acute systemic inflammation,19 we did not observe significant group differences in walking speed. Bonab et al. previously demonstrated that patients with ongoing LDH had significantly longer step duration and slower walking speed than healthy controls.4 In contrast to Bonab et al., the cases in the present study were treated for LDH more than a decade ago, and the reason for the lack of difference between cases and controls likely represents the remission among cases, even if we did find lingering postural differences at follow-up. Alternatively, cases may have adapted longitudinally because their LDH was acute on average 13.8 years ago. Because they were younger (≤18 years) than most individuals with LDH, they may have used compensatory resources to regain a walking speed on par with healthy controls, in spite of the altered head and trunk angles. A longitudinal investigation of gait after treatment could conclude whether regained walking speed stems from compensation or recovery.
4.2. Gait and its relation to other measuresOur hierarchical linear models revealed that there was no significant effect of age, BMI, or sex on gait outcomes. In the case of age and BMI, the limited variability likely accounts for this phenomenon. However, concerning sex, differences are frequently observed in the presence of long-term pain, with women being more often affected than men. Also, women generally experience more recurrent pain, more severe pain, and longer lasting pain than men.21 LDH, however, has less pronounced sex differences according to the Swedish Spine Register 2012 report. Thus, LDH is not a pain condition with distinct sex differences and may therefore not have a significant effect on our outcomes.
The trunk and back angles were not associated with measures of back morphology. Hence, the gait was unrelated to MRI-based measures of disk degeneration. In fact, our model revealed very low gait variance explained by Modic and Pfirrmann. It is known that the intensity of long-term back pain is not linear to objective findings of tissue damage using MRI,25,29 and here, we demonstrate that objective measures of gait seem unrelated to assessments of MRI back morphology too.
Even if head and trunk angle measures correlated with physical health scores, the hierarchical statistical model showed a limited amount of variance explained by health questionnaires. For head angle, only back pain rating explained a significant amount of variance beyond group, furthering the notion that pain perception per se is a key contributor to gait, rather than the actual disk morphology. In contrast to head angle, the trunk angle was associated with level of exercise and EQ-5D index. The EQ-5D index is generally considered a measure of health-related quality of life; however, one of 5 items is a direct question about pain, and another question is about negative affect. We interpret the association between gait and the EQ-5D index as a link between gait and pain and potentially also negative affect. The level of exercise is likely to have a direct effect on gait and will thereby explain significant variance in our statistical model above and beyond group.
4.3. General healthCases displayed more disk degeneration than controls, and they also reported worse health on several different physical health parameters, such as disability because of back pain (ODI), back pain, and physical pain, as reported in Table 1. However, the mental health indicator from SF-36 was not different between cases and controls. Long-term pain is generally associated with negative affect and anxiety, yet our data suggest that individuals with LDH learn to cope well with their pain and disability. Our data cannot link the follow-up scores to the mental score at the time of surgery, which would have been an interesting association to analyse.
4.4. Strengths and limitationsLong-term follow-ups for treatments such as surgery for adolescent LDH are uncommon, which is one of the strengths of this study, because it reveals differences between cases and controls that may have been overlooked if only studied at the time of surgery. Yet, the sample size in this study was small and the results should be interpreted with caution. Replication of these findings is therefore warranted. The addition of a conservatively treated cohort for LDH could also help in concluding whether the differences observed were caused by complications from surgery or current LDH symptoms. In conclusion, it would be beneficial to assess the effect of time on treatment by including baseline gait data.
Because of lack of correlations between lumbar MRI morphology and clinical measures, gait may be a cheap and convenient way to provide objective outcome measures in LDH clinical trials as a means to quantify differences over time and across interventions.
4.5. SummaryAt 13.8 years of follow-up, the head and trunk angles among individuals who were surgically treated for LDH during adolescence were different compared with healthy controls. The difference may be associated with residual pain, causing longitudinal change in postural movement patterns. However, the present study cannot discern if differences in gait were there before surgery, as a vulnerability factor for LDH. All the same, self-rated pain and exercise habits seem to predict postural variance better than corresponding lumbar spine MRI morphology in the surgically treated cohort, but the underlying cause will remain unknown until a comparison is made with conservatively treated LDH.
DisclosuresThe authors have no conflict of interest to declare.
Appendix A. Supplemental digital contentSupplemental digital content associated with this article can be found online at https://links.lww.com/PR9/A225
AcknowledgmentsS.B. has received financial support from the Sven Jerring Foundation.
Data availability: deidentified data can be provided on request.
References [1]. Aihara T, Kojima A, Urushibara M, Endo K, Sawaji Y, Suzuki H, Nishimura H, Murata K, Konishi T, Yamamoto K. Long-term reoperation rates and causes for reoperations following lumbar microendoscopic discectomy and decompression: 10-year follow-up. J Clin Neurosci 2022;95:123–8. [2]. Almasi S, Ahmadi H, Asadi F, Shahmoradi L, Arji G, Alizadeh M, Kolivand H. Kinect-based rehabilitation systems for stroke patients: a scoping review. Biomed Res Int 2022;2022:4339054. [3]. Bawa A, Banitsas K, Abbod M. A review on the use of Microsoft Kinect for gait abnormality and postural disorder assessment. J Healthc Eng 2021;2021:4360122. [4]. Bonab M, Colak TK, Toktas ZO, Konya D. Assessment of spatiotemporal gait parameters in patients with lumbar disc herniation and patients with chronic mechanical low back pain. Turk Neurosurg 2020;30:277–284. [5]. Bonnefoy-Mazure A, Deslandes J. Normal gait. In: Canavese AF, Stéphane, editors. Orthopedic management of children with cerebral palsy: a comprehensive approach. New York: Nova Biomedical, 2015. p. 199–214. [6]. Burkhardt BW, Grimm M, Schwerdtfeger K, Oertel JM. The microsurgical treatment of lumbar disc herniation: a report of 158 patients with a mean follow-up of more than 32 years. Spine (Phila Pa 1976) 2019;44:1426–34. [7]. Cabaraux P, Agrawal SK, Cai H, Calabro RS, Casali C, Damm L, Doss S, Habas C, Horn AKE, Ilg W, Louis ED, Mitoma H, Monaco V, Petracca M, Ranavolo A, Rao AK, Ruggieri S, Schirinzi T, Serrao M, Summa S, Strupp M, Surgent O, Synofzik M, Tao S, Terasi H, Torres-Russotto D, Travers B, Roper JA, Manto M. Consensus paper: ataxic gait. Cerebellum 2023;22:394–430. [8]. Cahill J, Frost G, Solanki GA. Paediatric lumbar disc herniation in the very young: a case-based update. Childs Nerv Syst 2011;27:687–91. [9]. Cunha M, Basto D, Silva PS, Vaz R, Pereira P. Long-term outcome of redo discectomy for recurrent lumbar disc herniations. Eur Spine J 2023;32:534–41. [10]. Durham SR, Sun PP, Sutton LN. Surgically treated lumbar disc disease in the pediatric population: an outcome study. J Neurosurg 2000;92:1–6. [11]. Eltoukhy M, Kuenze C, Oh J, Jacopetti M, Wooten S, Signorile J. Microsoft Kinect can distinguish differences in over-ground gait between older persons with and without Parkinson's disease. Med Eng Phys 2017;44:1–7. [12]. Galna B, Barry G, Jackson D, Mhiripiri D, Olivier P, Rochester L. Accuracy of the Microsoft Kinect sensor for measuring movement in people with Parkinson's disease. Gait Posture 2014;39:1062–8. [13]. Huang YP, Bruijn SM, Lin JH, Meijer OG, Wu WH, Abbasi-Bafghi H, Lin XC, van Dieen JH. Gait adaptations in low back pain patients with lumbar disc herniation: trunk coordination and arm swing. Eur Spine J 2011;20:491–9. [14]. Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine (Phila Pa 1976) 2008;33:2464–72. [15]. Kurihara A, Kataoka O. Lumbar disc herniation in children and adolescents. A review of 70 operated cases and their minimum 5-year follow-up studies. Spine (Phila Pa 1976) 1980;5:443–51. [16]. Lagerback T, Elkan P, Moller H, Grauers A, Diarbakerli E, Gerdhem P. An observational study on the outcome after surgery for lumbar disc herniation in adolescents compared with adults based on the Swedish Spine Register. Spine J 2015;15:1241–7. [17]. Lagerback T, Kastrati G, Moller H, Jensen K, Skorpil M, Gerdhem P. MRI characteristics at a mean of thirteen years after lumbar disc herniation surgery in adolescents: a case-control study. JB JS Open Access 2021;6:e21.00081. [18]. Lamoth CJ, Meijer OG, Daffertshofer A, Wuisman PI, Beek PJ. Effects of chronic low back pain on trunk coordination and back muscle activity during walking: changes in motor control. Eur Spine J 2006;15:23–40. [19]. Lasselin J, Sundelin T, Wayne PM, Olsson MJ, Paues Goranson S, Axelsson J, Lekander M. Biological motion during inflammation in humans. Brain Behav Immun 2020;84:147–53. [20]. Lee K, Kim ES, Jung B, Park SW, Ha IH. Association between pain and gait instability in patients with lumbar disc herniation. J Int Med Res 2021;49:3000605211039386. [21]. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth 2019;123:e273–83.
留言 (0)