
記住我





In 2020, the rate of persistent chronic pain was 462 per 1000 person-years, making it a highly prevalent public health concern.56 Lumbosacral radiculopathy (LR), sometimes referred to as sciatica or lumbar radiating pain, is a specific type of chronic neurologic pain that involves radiating sensations of pain, burning, tingling, or numbness down 1 or both legs. Many cases of LR will evolve to mixed pain (nociceptive, neuropathic, and nociplastic),23 which can last for years or decades as a result of central sensitization.57 Given the potential for chronicity and the high lifetime prevalence of LR, as high as 43%,46 mitigating the development of nociplastic pain and managing risk factors such as fear avoidance,42 sedentary behaviors,14,36 and social isolation8,44,48 is crucial for patients—especially those with low health-related self-efficacy and worsening disability accentuated during the COVID-19 pandemic.11
Because of risks associated with long-term pharmaceutical pain management, organizations such as the National Institutes of Health HEAL Initiative and the International Association for the Study of Pain have shifted their focus towards integrative and nonpharmacologic management of chronic pain—decisions informed in part by decades of work on the application of mindfulness-based interventions (MBI).1,34,76 The American College of Physicians already recommends nonpharmacologic treatments such as chiropractic manipulations,72 tai-chi, yoga, and mindfulness-based stress reduction as first-line treatment for chronic low back pain (cLBP).65 In addition to LBP,5,12,35 MBIs have been studied for various neuropathic conditions including fibromyalgia,3 diabetic neuropathy,39 and chemotherapy-induced peripheral neuropathy.70
Mindfulness-Oriented Recovery Enhancement (MORE) is a mindfulness-based intervention that is designed as a therapeutic tool for disrupting the bidirectional and self-perpetuating relationship between chronic pain and stress. Mindfulness-Oriented Recovery Enhancement integrates training in mindfulness skills to enhance attentional control over pain, attentional bias, and facilitate a shift from affective to sensory processing of pain; reappraisal skills to decrease catastrophizing and facilitate negative emotion regulation; and savoring skills to enhance positive emotional regulation and amplify reward processing.26,61 Using savoring, MORE targets dysregulated hedonic patterns. To accomplish this, MORE therapists guide participants through a process of phenomenologic self-discovery and external processing that promotes pain reappraisal and encourages social–observational learning.29 Through external processing of meditation experiences through group discussion, participants are encouraged to engage socially, therefore increasing their engagement in mindfulness practice—a process that may augment both quantitative and qualitative outcomes.50,53 In a previous randomized clinical trial by Garland et al.,26 MORE was compared with supportive group therapy for patients with chronic pain and a history of opioid misuse. This design allowed for the control of group factors such as social support and development of therapeutic relationships. The authors found that MORE reduced the occurrence of opioid misuse by 45% at 9-month follow-up, more than doubling the effect of supportive group therapy. In addition, MORE was superior in reducing pain-related functional interference and emotional distress.
Despite the growing body of evidence on MBIs, it remains a small area of interest that is not included in evidence maps and systematic reviews on psychological interventions for chronic pain.9,37,51 This article shares findings from self-report questionnaires in the trial described by Wexler et al.,75 which were collected during the peak of the COVID-19 pandemic. The primary aims of this research are to evaluate the impact of MORE on disability, pain, quality of life, depression, mindful reinterpretation of pain, and trait mindfulness scores as compared to treatment-as-usual (TAU) in patients with LR. We hypothesized that participants undergoing training in MORE would experience improvements relative to TAU participants in disability, pain, quality of life, depression, mindful reinterpretation of pain, and trait mindfulness.
2. MethodsThis study adheres to Consolidated Standards of Reporting Trials (CONSORT) guidelines, is registered at clinicaltrials.gov (NCT04818606), and was approved by the National University of Natural Medicine (NUNM) IRB (IRB#: KP112720). Data were collected following the previously described protocol by Wexler et al. (2022) with only minor protocol modifications; these changes are described in detail below.75
2.1. Recruitment and participantsIn summary, adults with LR were randomized to MORE or TAU for 8 weeks. Patients were eligible if meeting the following criteria: presence of radiculopathy symptoms extending below the knee secondary to LBP for greater than 6 weeks with a painDETECT score greater than 18 or previous diagnosis of LR (ICD-10 M54.16, M54.17, M51.16, M51.17, M47.26, M47.27, M54.40, M54.41, M54.42, M99.53, M99.54, S34.21, S34.22, G54.4, and G55); 18 to 65 years of age; ability to read and understand English; willingness to be randomized to either group; willingness to refrain from self-directed treatment plan changes; daily access to the internet; have not received an epidural steroid injection of LR in the previous 3 months; have not received a surgical intervention for LR in the previous 6 months; ability to complete 20 unassisted gait cycles; does not have a regular mindfulness practice of at least once a week; does not have a diagnosis of cancer; does not have an allergy to adhesive; and does not have an unmanaged or uncontrolled mental illness known to cause psychosis.
Most eligible participants were identified and contacted through electronic medical records systems queries within the NUNM Health Center, the Oregon Health & Science University Spine Center, and the Oregon Health & Science University Comprehensive Pain Center. Electronic health records queries were conducted using the aforementioned eligibility criteria as filters. Patients were initially contacted through email and followed up through phone 1, 2, and 4 weeks thereafter. A final email was sent to all patients not reached through phone before closing recruitment. In total, this search strategy included patients under the care of providers from at least 8 health care specialties, including acupuncture, chiropractic, interventional radiology, massage, naturopathy, nurse practitioner, psychology, and psychiatry.
2.2. Study visitsAll baseline study visits were conducted in-person at Helfgott Research Institute at NUNM in Portland, Oregon. Baseline visits included a review of participant eligibility, a discussion and signing of the informed consent, completion of self-report questionnaires, and surface electromyography testing (to be reported elsewhere). Baseline study visits lasted between 30 and 75 minutes, depending on participant questions and timeliness in survey completion. Follow-up visits contained, at most, the self-report questionnaires and surface electromyography testing; because of the nature of the ongoing COVID-19 pandemic at the time of study implementation, participants were offered the opportunity to complete follow-up visits virtually, with self-report questionnaires delivered remotely through Research Electronic Data Capture (REDCap). Study data were collected and managed using REDCap electronic data capture tools hosted at NUNM.31,32,47 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.
2.3. Interventions 2.3.1. Treatment-as-usualParticipants in the control group, TAU, were asked to maintain their current treatment regimen, including but not limited to physical therapy, oral anti-inflammatories, acupuncture, chiropractic, massage, etc., and asked to report treatment plan changes made while enrolled in the study. Treatment plan changes were made reportable through a daily survey containing a visual analogue scale (VAS) for pain intensity that was delivered by text using Twilio16 or email, dependent on participant preference. Altogether, TAU group participants received a daily survey containing 3 questions: (1) the daily VAS, (2) any treatment plan changes made, and (3) if treatment plan changes were made, please describe them. Treatment-as-usual group participants were added to a waitlist to participate in the MORE program after cessation of data collection, as is conventional in mindfulness studies.
2.3.2. Mindfulness-Oriented Recovery Enhancement + treatment-as-usualMindfulness-Oriented Recovery Enhancement is an 8-week mindfulness intervention with once-weekly 2-hour sessions and regular “homework” throughout the week. Mindfulness-Oriented Recovery Enhancement equips participants with 3 tools or tenets through which to view and manage pain: mindfulness, reappraisal, and savoring.28 As noted in session descriptions available in Appendix A, https://links.lww.com/PR9/A223, all 3 of these tools are introduced within the first 4 weeks of the program and then built upon in subsequent sessions. During sessions, participants are guided through mindfulness practices, group discussion, and pain education as manualized (instructor training and qualifications are described in the study protocol).28 Participants were sent weekly reminders about synchronous sessions before class each week and followed up through phone, if absent, to troubleshoot technology challenges and barriers to participation. As this study was conducted at the height of the COVID-19 pandemic, MORE was delivered virtually each week. To join the session, participants joined a Zoom meeting using an anonymized screen name, which was self-selected at the participants' baseline visit. Participants were encouraged to keep their video on during class but were provided the option to remain off camera for comfort or anonymity, if preferred.
Participants who were unable to attend sessions were provided with recorded session audio to review on their own, to stay on schedule with educational content. Participants were also provided with recorded guided meditations from the MORE instructor and homework to complete throughout the week. These instructions were provided in regular follow-up emails after the weekly session.
As with TAU, MORE participants were asked to maintain other elements of their treatment plan the same as at baseline and report changes made during enrollment. In addition to the 3 questions asked of TAU participants in the daily survey, MORE participants were also provided a space to share reflections from their practice and asked to report their daily practice time. As described in the study protocol, all study participants received a copy of the pain education handout, “Understanding Pain,” provided publicly by the Oregon Pain Management Commission, at the time of intervention initiation.60
2.4. Outcome measures and data collectionThe present analysis includes all 7 self-report outcome measures used in this study: Modified Oswestry Disability Index (ODI), painDETECT Questionnaire (PDQ), Pain VAS, Major Depressive Inventory (MDI), SF-12 Quality of Life Questionnaire (SF-12), Mindful Reappraisal of Pain Scale (MRPS), and the Five-Facet Mindfulness Questionnaire (FFMQ). Participants completed questionnaires at the baseline and follow-up study visits, whereas the VAS was completed daily through automated REDCap emails or Twilio texts based on participant preference. All study visits were conducted at Helfgott Research Institute or remotely. The ODI was selected as the primary outcome measure for this study because it is frequently used for the assessment of improvement in LR symptoms in studies of steroid injection efficacy—one of the most common treatments for LR.4,13,20,58,59 In addition to symptom-specific questionnaires, a demographics and health history questionnaire was designed by the study team to capture information on diagnosis, condition duration, and past and current treatments. With the exception of the MRPS, all questionnaires are described in detail in the original study protocol,75 including their rationale for use in this subpopulation.
The MRPS is a self-report questionnaire designed to quantify participant mindfulness practices as it relates to mindful reappraisal of pain.27 The MRPS is adapted from the reinterpreting pain sensations subscale of the Coping Strategies Questionnaire66 to use language relevant to the teaching content common to MBIs. In addition to questions adapted from the Coping Strategies Questionnaire, additional questions were built into the MRPS specific to meditation practices, such as focusing attention on the breath and changing body sensations. Evaluated in samples of opioid-treated patients with chronic pain, the MRPS is a 9-item survey measured on a scale from 0, “never do that,” to 6, “always do that,” with responses summed to create a composite score. It was found to have good convergent and discriminant validity with various mindfulness and coping questionnaires, to be highly sensitive to change in participants undergoing mindfulness training, and to mediate the effect of MORE on pain severity as measured by the brief pain inventory.27
2.5. Sample sizeApplying estimates of a minimal clinically important difference for the primary outcome measure (ie, the ODI) of 10 points,17 an effect size of d = 0.83,19,24,25 and alpha = 0.05, with power = 80% yielded a required sample size of 48 total participants. At protocol development, an 80% retention rate was assumed, resulting in a necessary recruitment of 60 participants. Sample size calculations are described in detail in the previously published protocol.75
2.6. Adverse eventsAdverse events were evaluated through regular monitoring of daily participant reports and classified as anticipated, unanticipated, and medical emergency. In addition, the mindfulness instructor was informed of the need to communicate adverse events occurring during weekly sessions to the study coordinator and principal investigator. Weekly session audio recordings were reviewed by the study coordinator for potential adverse events. Adverse events occurring during the intervention were logged in a REDCap form and reported to the NUNM IRB. Expected adverse events included mental health exacerbations related to mindfulness practices or to completion of the self-report questionnaires at the study visits. Any adverse events reported directly to the study coordinator or found in weekly audio sessions were subsequently reported to the principal investigator for follow-up with the study participant.
2.7. Randomization and blindingRandomization adhered to the previously published protocol.75 Three sequential cohorts of 24 to 46 (12–23 per group) participants were recruited into the study and underwent group assignment through simple randomization using a random number generator. Although this deviates from optimal cohort volume for psychotherapeutic interventions, larger cohorts were necessary because of study resource limitations.22 Once maximum enrollment had been reached for a given cohort, randomization was conducted, and subsequent cohort enrollment began. Methods for allocation concealment were previously reported and adhered to.75
2.8. Statistical analysis planStatistical analyses were conducted using SPSS Version 29.0.0.40 and adhered to the described protocol.75 Briefly, linear mixed modeling with maximum likelihood estimation and random participant intercept was used to assess changes in ODI, MDI, SF-12, MPRS, and FFMQ scores from baseline to follow-up using an intention-to-treat (ITT) design with group × time interaction as the main effect of interest. Potential covariates included age, sex, change in treatment during study enrollment (as a binary variable), disease etiology, duration of symptoms before study enrollment, previous condition-specific surgery, and baseline instrument score. Multilevel modeling with maximum likelihood estimation of missing data was used for growth curve analysis of daily pain VAS data, which has a nested hierarchical structure with both between- and within-subject predictors. The group × time interaction was the primary fixed effect of interest. Models included a random intercept, and the covariance structure for repeated effects (diagonal or AR1) was also evaluated by -2LL fit statistics.
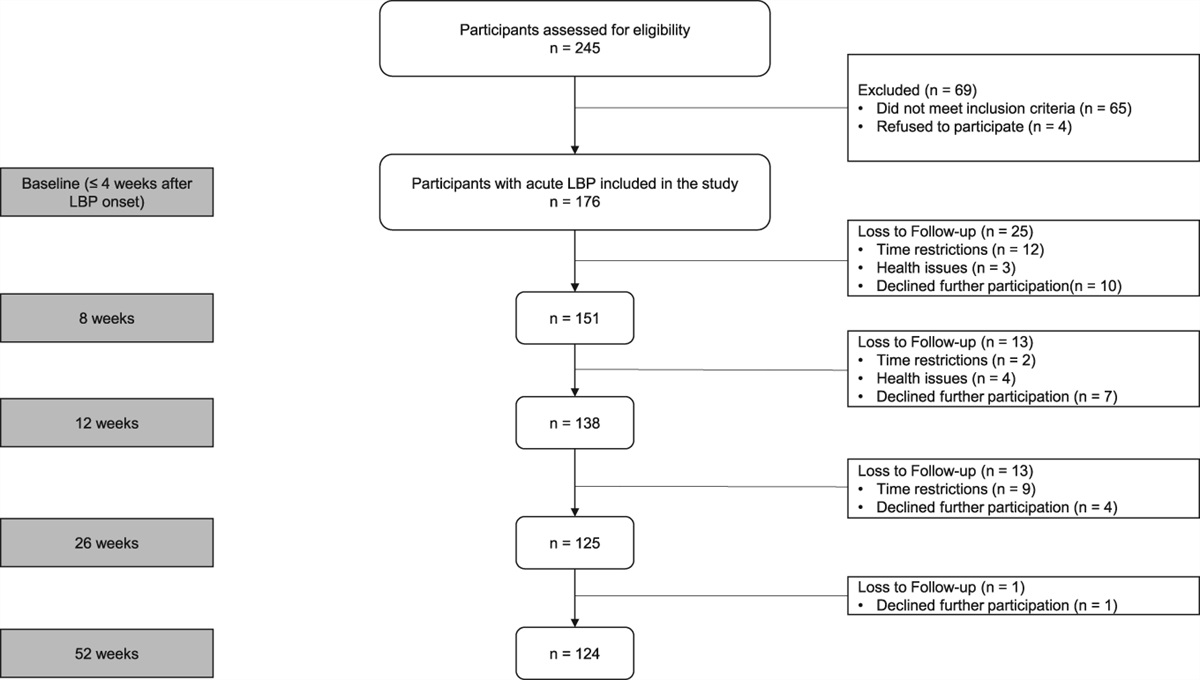
3. ResultsBetween January 2021 and January 2022, a team of 8 research staff contacted 139 patients from NUNM and 906 patients from Oregon Health & Science University. Of these 1045 patients contacted, 523 (50%) were assessed for eligibility, and 71 (6.8%) were enrolled in the trial. Dropout and lost to follow-up was 28 (39%). Eleven (15%) patients were recruited from NUNM, 31 (44%) from the SPC, 27 (38%) from the CPC, and 2 (2.8%) from community advertising. Participant dropout and group assignment can be seen in the CONSORT diagram (Fig. 1). Fourteen participants (9 MORE and 5 TAU) were lost to follow-up, and another 14 (10 MORE and 4 TAU) dropped out of the study. Nineteen MORE group participants completed follow-up surveys. Amongst these participants, mean session attendance was 5.28 (±1.99) with 14 participants (74%) receiving the minimal intervention dose. Upon randomization, no significant differences were found between the MORE and TAU groups regarding age, condition duration, sex, race, and scores on any self-report outcome measures. Baseline demographic characteristics, prevalence of disease etiology, and number of patients with common LR symptoms can be seen by group in Table 1 with group comparisons for each outcome measure in Table 2. In addition, because of the high dropout rate in this study, a separate assessment of baseline characteristics was conducted on participants who completed the trial (ie, attended a follow-up visit), vs those who did not (Table 3).
 Figure 1.:
Figure 1.: CONSORT diagram. CONSORT, Consolidated Standards of Reporting Trials.
Table 1 - Demographic characteristics at baseline presented as mean (SD) or n (%). MORE (n = 37) TAU (n = 34) Demographics Sex P = 0.313* Male 11 (30%) 14 (41%) Female 26 (70%) 20 (59%) Race P = 0.219* Anglo-American 30 25 Black 2 — Asian — 2 Hispanic/Latino 2 2 Middle Eastern 1 1 More than 1 race 1 4 Other 1 — Age, mean (SD) 48.59 (±11.59) 44.94 (±11.47) P = 0.187 Previous back surgeries P = 0.368* One surgery 5 (14%) 4 (12%) Two surgeries 1 (3%) — Three or more surgeries 2 (5%) — Condition duration (yr), mean (SD) 13.72 (±20.28) 12.76 (±11.28) P = 0.718 Etiology L3-L4 disc herniation 1 — L4-L5 disc herniation 4 2 L5-S1 disc herniation — 1 Disc herniation of unknown level 1 2 Osteoarthritis 1 — Bone spur 1 — Degenerative disc disease 4 4 Spondylolisthesis 2 0 Vertebral fracture 1 2 Inflammation 2 — Scoliosis 1 — Congenital 1 — Central canal stenosis 1 2 Failed back surgery syndrome 1 1 Etiology unknown 17 19 Visual analogue scale for pain intensity 5.14 (±1.78) 5.00 (±2.06) P = 0.770 painDETECT Questionnaire (PDQ) P = 0.170* PDQ > 18 18 (48.64%) 22 (64.70%) PDQ > 12 and ≤18 11 (29.72%) 4 (11.76%) PDQ ≤ 12 8 (21.62%) 8 (23.52%) Symptoms Numbness 27 (73.0%) 25 (73,5%) Tingling 27 (73.0%) 24 (70.6%) Weakness 24 (64.9%) 23 (67.6%) Burning/Electric 27 (73.0%) 26 (76.5%)*P-value calculated using χ2.
MORE, Mindfulness-Oriented Recovery Enhancement; TAU, treatment-as-usual.
FFMQ, Five-Facet Mindfulness Questionnaire; MCS, mental component score; MDI, Major Depressive Inventory; MRPS, Mindful Reappraisal of Pain Scale; ODI, Oswestry Disability Index; PCS, physical component score; SF-12, Short-Form Quality of Life Questionnaire.
*P-value calculated using χ2.
FFMQ, Five-Facet Mindfulness Questionnaire; MCS, mental component score; MDI, Major Depressive Inventory; MRPS, Mindful Reappraisal of Pain Scale; ODI, Oswestry Disability Index; PCS, physical component score; PDQ, painDETECT Questionnaire; SF-12, Short-Form Quality of Life Questionnaire.
Because no potential covariates met the prespecified criterion of correlation r ≥ 0.3 with any outcome measure, models described below are unadjusted. The group × time interaction was the primary fixed effect of interest. Regarding ODI scores, the main effect of time was significant, F(1,46.77) = 7.54, P = 0.009. The group × time interaction was nonsignificant F(1,46.73) = 3.00, P = 0.09, indicating that change in ODI scores did not differ significantly between MORE and TAU groups.
Regarding daily pain intensity, the main effect of time was significant, B = −0.006 (SE = 0.002), P = 0.002. Importantly, the group × time interaction was significant, group × time B = −0.007 (SE = 0.003), P = 0.039, such that compared with TAU, participants in MORE reported significantly greater decreases in daily pain VAS over 8 weeks (14.0% decrease in pain intensity in MORE compared with a 6.8% decrease in TAU).
Regarding MDI scores, the main effect of time was significant, F(1,43.35) = 5.23, P = 0.027, with MDI scores improving across both groups. The group × time interaction was nonsignificant F(1,43.45) = 1.28, P = 0.26, indicating that change in MDI scores did not differ significantly between MORE and TAU groups.
Regarding SF-12 physical component scores (PCS), the main effect of time was significant, F(1,43.78) = 15.27, P < 0.001, with SF-12 PCS scores improving across both groups. The group × time interaction was nonsignificant F(1,43.78) = 0.00, P = 0.99, indicating that change in SF-12 PCS scores did not differ significantly between MORE and TAU groups. Regarding SF-12 mental component scores (MCS), the main effect of time was nonsignificant, F(1, 42.72) = 0.091, P = 0.764. The group × time interaction was nonsignificant F(1, 42.72) = 0.019, P = 0.890, indicating that change in SF-12 MCS scores did not differ significantly between MORE and TAU groups.
Regarding FFMQ-Total scores, the main effect of time was significant, F(1,44.13) = 11.90, P = 0.001, with FFMQ scores improving across both groups. Importantly, the group × time interaction was significant F(1,44.13) = 4.72, P = 0.035, such that patients in MORE
留言 (0)