Analysis of our study data showed that the female sex is prevalent among the 2 groups. In fact, CD was more prevalent in female sex, as also reported in literature.
However, there was a significant difference in the distribution between the two sexes about the prevalence of autoimmune comorbidities (type I diabetes mellitus, thyroiditis and JIA). In fact, in the first group the male sex was the one who was more affected by autoimmune comorbidities, while the female sex was more affected in the second group. Since the prevalence of female sex in autoimmune diseases was well known in literature, in particular in thyroiditis [13], it was probably a longer time from disease onset that determined a higher prevalence of autoimmune comorbidities in our group 1, which in our study mainly involved males. The prevalence percentages of autoimmune diseases found in this group are comparable to those present in the literature.
In particular, the development of IDDM in patients with celiac disease was more frequent in males than in females in both our groups. This finding seems to agree with the higher prevalence of male sex in IDDM population.
The single analysis of comorbidity “thyroiditis” showed a significant difference with a P value of 0.02 between the two groups confirming that a longer time since disease onset increased the risk of comorbidity and this affected male and female sex equally (4 M and 4 F) in the first group. In the second group, only one female child had thyroiditis and celiac disease as more frequently reported in literature.
Also, patients affected by oligo articular JIA were females in both groups according to literature data [14].
About the average age at diagnosis there is no significant difference between the two groups, however children belonging to the “biopsy sparing” group may have longest time of disease onset needed to rise the anti-TTG IgA levels to ten times UNL.
Although there was no difference in the age of onset between the two groups, it was more probably that the disease in the subjects belonging to the first group has arisen before the clinical onset.
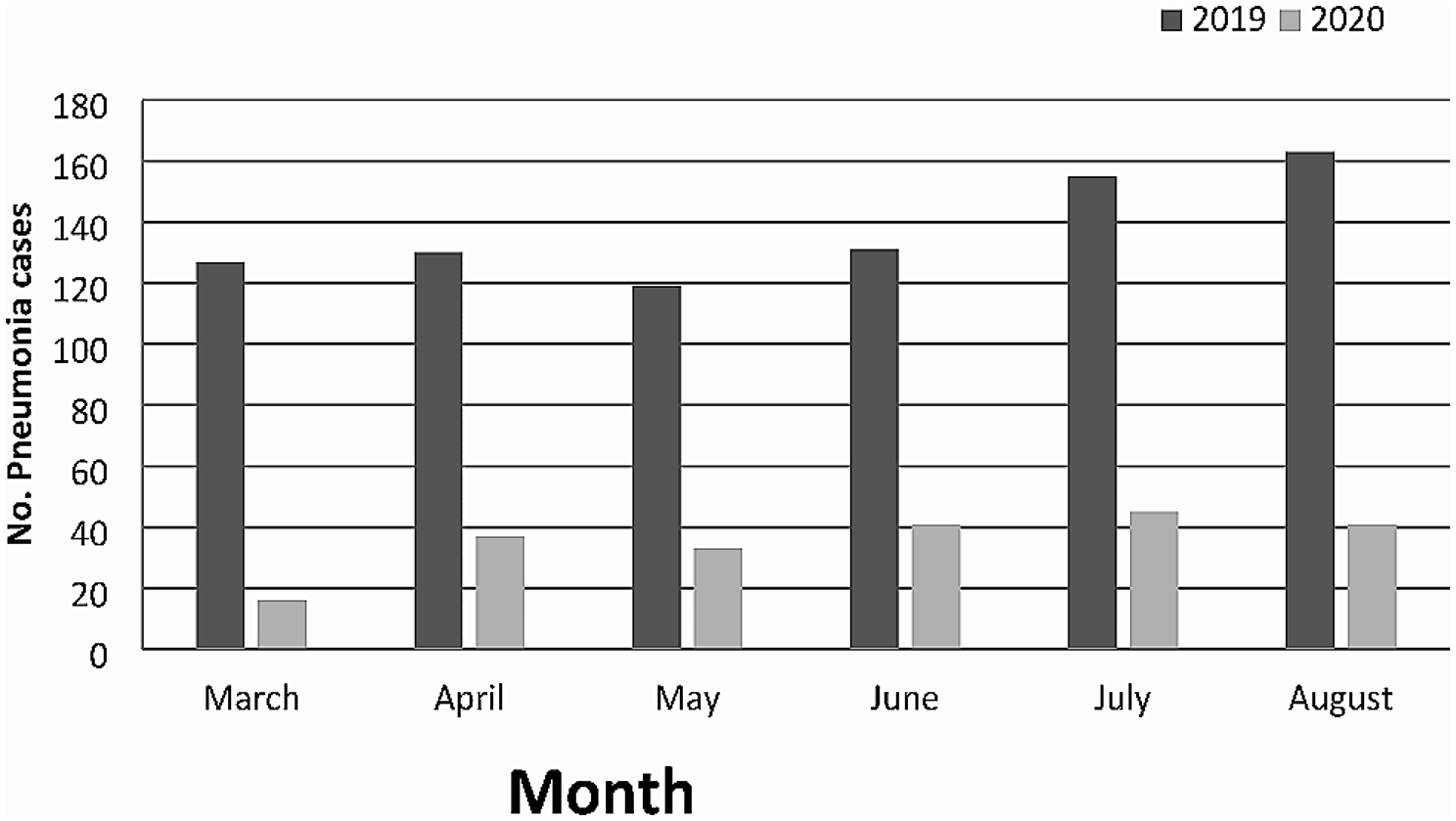
The analysis of symptoms at the onset of celiac disease in the two groups showed no significant differences. In fact, recurrent abdominal pain was the most important symptom in both groups, followed by postprandial hypoglycaemia in patients with IDDM and then by delay of somatic growth. Recurrent hypoglycaemia, in particular postprandial hypoglycaemia, was also increased in IDDM and CD (see Fig. 4). Recurrent hypoglycaemic events can lower the hypoglycaemic threshold at which symptoms occur in an individual, due to attenuation of the sympathoadrenal response, and may influence brain development and function [15–16]. In the first group one male patient presented Down Syndrome. Feeding problems and gastrointestinal disorders are the most common anomalies in people with Down syndrome [17] and have a significant impact on their daily life: in particular for celiac serology there is no consensus on the starting age and the frequency of screening, but numerous studies propose every year from the age of 2 years.
The risk of autoimmune diseases was approximately twice as high in females who had Turner Syndrome [18] compared to the general female population. The spectrum included Hashimoto’s thyroiditis, CD, IDDM, alopecia areata, inflammatory bowel disease, juvenile rheumatoid arthritis and so on [19]. In this study only one patient was affected by Turner Syndrome and CD with no other comorbidities.
In literature, the rates of extraintestinal manifestations of CD are similar in adults and in children. In children, short stature, fatigue, and headache are more represented [20]. Amongst the neurological manifestations, cerebellar ataxia, peripheral neuropathy and epilepsy, have been recognized as possible complications and/or starting manifestation of CD [21]. In our female patient the neurological manifestation, started at age of nine, was represented by an occipital epilepsy form associated with abdominal pain and anaemia. Patients with CD frequently develop antibodies against antigens related to the endocrine organs and in the same way, some authors described autoantibodies acting as possible “triggers” of neurological manifestations. Also, the risk for developing neurological manifestations, as for other autoimmune disorders seems higher in case of long-standing gluten exposure. In our case the neurological manifestation disappeared after a gluten free diet, according to the hypothesis that an important role could be played by the duration of gluten exposure [22,23,24].
The data analysis showed that four patients, in group 1, have IgA anti TTG levels upper to 30 times the norm, but only one female patient of these presents IDDM. According to our findings, extremely elevated levels of IgA anti TTG do not appear to have increased associated comorbidities in the same patients. A higher title of antibodies does not seem to correlate directly with a higher risk of comorbidity, even if it is related with a high damage in enteropathy [25].





留言 (0)