Most cases of trichobezoar present with non-specific symptoms like vomiting, constipation, abdominal pain, weight loss, and loss of appetite. Hence, they are often underdiagnosed and grow considerably to cause complications that include gastric outlet obstruction, hematemesis, gastric ulceration and perforation, intussusception, and protein-losing enteropathy [6]. If large, they can extend into the small intestine causing cholangitis, obstructive jaundice, and pancreatitis [7]. In two case reports, Rapunzel syndrome presented solely with iron deficiency anemia [8, 9]. Generalized edema in the pediatric population is also one of the rare presentations of this syndrome [10].
In our case, generalized edema was the initial presentation with no supporting clue to the diagnosis in the history and examination except alopecia patches. The child’s parents were not inquired specifically about the history of trichophagia and trichotillomania initially. Although child neglect was suspected pertaining to the overall health of the child. Considering the history of Wilson’s disease in the family, initial workup was directed towards it leading to a delay in the diagnosis, a true example of confirmation bias in medical diagnosis [11].
Rapunzel syndrome mostly arises in the context of psychiatric conditions—trichotillomania and trichophagia. In the pediatric population, hair-pulling behavior is mostly autonomic type, so children are often unaware of their act. Parents also do not pay much attention to this behavior. Psychiatric consultation for trichotillomania in the pediatric population is thus, rare, resulting in the development of secondary complaints.
In our case, no stressful life event or child abuse was identified, although child neglect was suspected due to the overall condition of the child and the presence of risk factors like poor socioeconomic status, chronically sick child in the family, and a large number of family members.
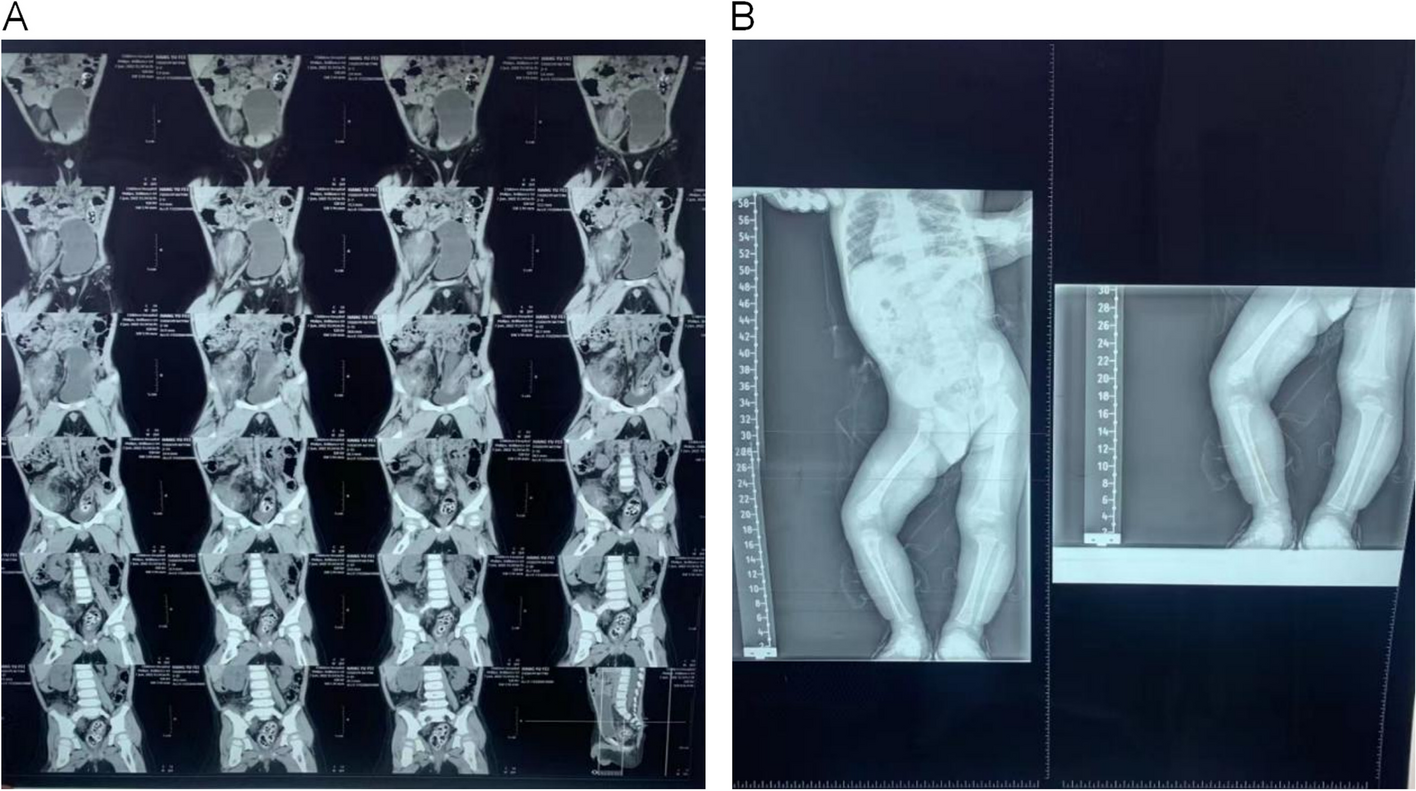
To confirm the diagnosis, imaging modalities like ultrasound and CT scan can be used. X-rays can also provide clues to the diagnosis. CT scan is the most commonly used imaging tool for the diagnosis with a higher detection rate than other imaging modalities. Nevertheless, upper gastrointestinal endoscopy is considered the gold standard for the diagnosis of trichobezoar [12]; however, we used X-rays along with clinical findings to reach a diagnosis.
While phytobezoars can be successfully treated medically using Coca-Cola or cellulase, no such treatment benefits trichobezoar. Endoscopic removal is another option. Various case reports have shown successful removal of trichobezoar in the pediatric population but still success rate of 5% has been reported [13]. It is associated with a higher complication rate causing ulceration, esophagitis, and esophageal perforation. Laparoscopic removal is an attractive option because it is less invasive and associated with shorter hospital stays. To date, many cases have been successfully treated [14]; however, it is not a widespread approach due to its complexity, increased risk of spillage of contents, and difficulty in looking for satellite lesions in the gastrointestinal tract. Laparotomy is considered the gold standard approach with a 100% success rate [15]. In Rapunzel syndrome, laparotomy is the safest and most commonly sought treatment approach. However, in the literature, the combined endoscopy-laparoscopy-gastrostomy approach in Rapunzel syndrome is also documented [16].





留言 (0)