
記住我




This study initially included 33 patients with AHT diagnosis. A total of 10 cases had to be excluded since the legal files were not accessible (n = 5), the legal procedure was still pending (n = 4) or the parents rejected the access to file (n = 1). A total of 23 cases were enrolled in this study. The cohort was divided into two groups according to the judicial outcome: indictment (10/23) or dismissal (13/23).
The characteristics and the diagnosis of the patients in the indictment (10/23) versus the dismissal (13/23) groups are detailed in Table 1.
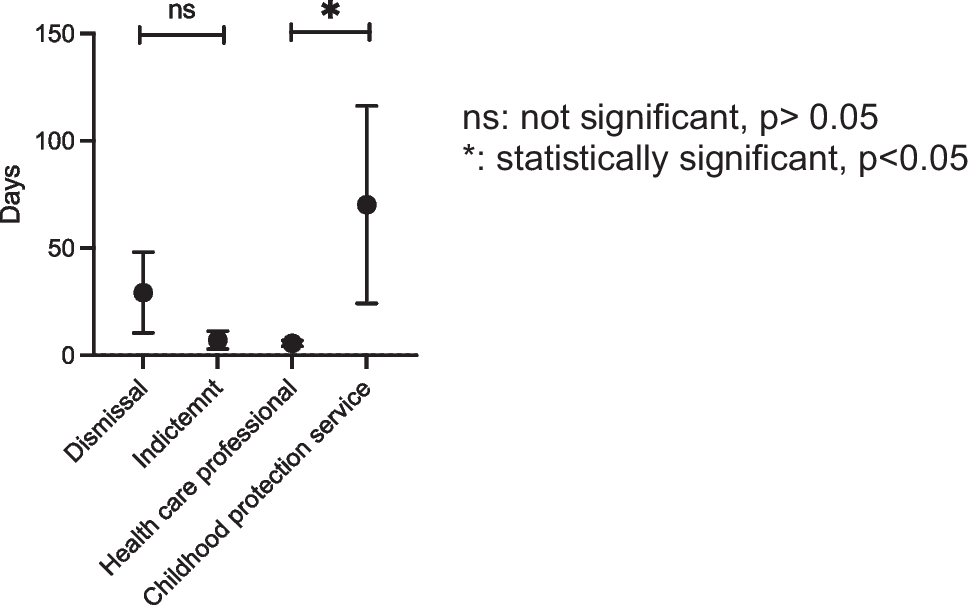
Table 1 Distribution and AHT diagnosis of patientsTimespan between diagnosis and reporting suspicion of AHTThe time span between AHT diagnosis and the filing of a police report for dismissed cases (29 ± 19 days, mean ± SEM) was not different from cases that led to indictments (7 ± 4 days) (p = 0.32; student’s t-test) (Fig. 1).
Once AHT is diagnosed, the police is notified directly by health care professionals or indirectly by the childhood’s protection service following a notification from a physician. After a first investigation, the cases move ex officio to public prosecution. When a report was filed by physicians, the time between diagnosis and reporting was 6 ± 1 days. The time span was considerably longer (70 ± 46 days) when the report was filed by the childhood protection service (p = 0.01; student’s t-test) (Fig. 1).
Fig. 1
Time span between diagnosis and filing a report depending on judicial outcome or author filing the report. ns: not significant, p > 0.05. *: statistically significant, p < 0.05
Health care professionals filed reports directly in 18/23 (78%) cases, while reports were filed by the childhood protection service in 5/23 (22%) cases. In the first group, 9/18 cases were dismissed and 9 led to an indictment (50%) (Fig. 2). In the second group, 4/5 cases were dismissed and only 1 resulted in an indictment (20%) (p = 0.23; chi squared test) (Fig. 2). Even though these data are not statistically significant, they nevertheless raise the possibility that an accelerated reporting increases the rate of cases that result in indictments.
Fig. 2
Author filing criminal complaint
Relation of medical documentation to judicial outcomeJudicial files were analysed for number and types of medical.
One of 13 patients in the dismissal group had to be excluded as the judicial file had been transferred to a foreign country during data collection. The charges had been dismissed in Switzerland. In the remaining 12 dismissed cases only 3/12 had a forensic report, while 6/10 cases in the indictment group included forensic reports (p = 0.096, chi-squared test) (Fig. 3).
Further, 3 of the 12 dismissed cases had no additional medical documentation, while all cases in the indictment group included at least one additional medical documentation (Fig. 3). Conversely, 5/10 cases in the indictment group had multiple documentations, which was only the case for 2/12 dismissed cases (p = 0.11, chi squared test) (Fig. 3). There is thus a trend to better medical documentation in the indictment group. For more details see Table S1 (Appendix).
Fig. 3
Type and number of medical documentations in judicial files. Other: no forensic report
Admission of shaking and judicial hypothesis for medical lesions and justification for judicial outcomesDismissalIn 4 of the 13 cases that were dismissed shaking was admitted. In these cases, shaking was explained by an attempted reanimation following a sudden loss of consciousness of the infant (4/13). Legally the dismissals were justified by insufficient evidence of intentional shaking or neglect (2/13) and exceeded limitation period (legal period during which the justice system must act, once passed, it is no longer possible to prosecute a suspect) (2/13).
Shaking was not admitted in 9/13 dismissed cases. Despite the fact that AHT diagnosis was certain to the physician, alternative explanations for the lesions seemed plausible to the public prosecutor. These explanations included accidental head trauma 30.8% (4/13), a game 15.4% (2/13), birth trauma resulting from the use of forceps and/or the side effects of vaccines (1/13). Legal files did not include any explanation for the symptoms in 2/13 cases.
The legal justification for dismissals were: the inability to prove the identity of the offender (7/13) or insufficient proof of guilt (2/13).
Court ProceedingsIn all cases that resulted in court proceedings (10/10), shaking was admitted.
Nine of the court proceedings resulted in convictions. In these cases, children were shaken based on crying (6/9), justified by an attempt to reanimate a child (1/9) or no obvious reason (2/9). Legally, perpetrators were convicted for negligent homicide (1/9) or simple body injury, grave bodily harm (by neglect), assault, violation of the duty to assist or educate and/or exposure offences (8/9).
One of the court proceedings ended in an acquittal (1/10). Here, the child was known to suffer from apnoea due to gastroesophageal reflux and resuscitations measures by shaking seamed plausible to the court in the context of the stressful situation.
In summary, during the judicial process shaking was admitted in 65% of all cases (14/23), 10 of which resulted in court proceedings. In all 10 cases, the court proceedings were the consequence of confessions. For more details see Appendix (Figure S1).
Limitations and strength of the studyThe most limiting factor of this study is the small number of cases, which is partly due to the small number of suspected AHT cases. In addition, AHT diagnosis may be uncertain, and we deliberately decided to only include cases with certain diagnosis in order to assess the fate of certain AHT diagnoses in court proceedings. These limitations reduced the number of victims to n = 23 that were treated at the CHUV over a period of 15 years.
This study, unique in Switzerland, made it possible for the first time to compare medical records with judicial records. This type of research is key to improve the collaboration between medical and legal communities to improve childhood protection by identifying the abuse and thus preventing possible recurrences. This study should be expanded to other centers to confirm and extend of our results.
留言 (0)