
記住我





Myopia is a growing public health issue because of its increasing prevalence,1,2 a better understanding of its role in uncorrectable visual impairment,3,4 and the ability to delay its onset5 and to slow its progression.6,7 Optical and pharmaceutical methods have been demonstrated to slow the progression of myopia6,7 and are in use around the world, although various regions are limited by regulatory approval, notably in the United States and Japan, and by the scope of practice of those administering primary eye care. Thus, the practitioner has a range of options to choose from when managing a young myopic patient. Many interventions have similar capacity to slow myopia progression. For example, select soft contact lenses can slow axial elongation by around 0.3 mm over 3 years.8 Similar efficacy can be achieved with some spectacle lenses,9,10 some concentrations of atropine,11,12 and overnight orthokeratology.13 The clinically meaningful efficacy14,15 that can be achieved for a range of modalities means that other factors come into play when discussing the intervention to be applied for a given child.16
COMPLIANCEWhen asked by a parent or colleague which myopia control modality is most effective, the answer should be “the one that the child will use.” Logically, an intervention that is never used will have no treatment benefit. Thus, it could be argued that the preeminent consideration when choosing a treatment is compliance. Of course, compliance is influenced by a range of factors, including comfort, vision, motivation, lifestyle, and the tangible benefits associated with the modality. Compliance is notoriously difficult to assess as it is generally done by questionnaire and subject to response bias.17 Nonetheless, there are clear examples where higher compliance in terms of wearing time has been shown to be associated with greater treatment efficacy.
Soft contact lensesA 2-year randomized clinical trial of 221 children aged 8 to 13 years compared myopia progression between those wearing the Defocus Incorporated Soft Contact (DISC) lens and those wearing a single-vision contact lens.18 Only 128 children completed the study, but myopia progression (0.59 vs. 0.79 D) and axial elongation (0.25 vs. 0.37 mm) were lower in the DISC lens wearers than those in the spectacle wearers, giving an efficacy of 0.20 D and 0.11 mm. The mean wearing time was around only 6.5 hours per day in both groups, around half of that reported in similar studies.19,20 This may be due to the lenses being lathe cut from 2-hydroxyethyl methacrylate, with 38% water content, rather than cast molded in a more contemporary hydrogel material such as omafilcon A8 or a silicone hydrogel such as senofilcon A.21 The low wearing times appear to have contributed to the modest myopia control efficacy of the lens. In a subgroup analysis, when only participants who wore the lenses at least 8 hours per day were considered, the 2-year myopia control efficacy increased from 0.21 to 0.53 D.18
More recently, a 2-year trial followed wearers of four test soft contact lenses and a control soft lens. Those who wore their lenses for 5 days a week or less had similar progression to those in the control group. Those who wore their lenses for 6 or 7 days a week had significantly less progression than those in the control group (0.20 D and 0.12 mm).22 Likewise, a 6-month clinical trial compared two prototype myopia control soft contact lenses with noncoaxial ring-focus designs with dual-focus and single-vision designs.21 While mean wearing time exceeded 12 hours for all four lenses, it was still found to influence axial elongation. In contrast, in a 3-year clinical trial of 109 myopic children aged 8 to 12 years randomized to wear either dual-focus or single-vision soft contact lenses,8 the mean wearing time was around 13 hours per day and “did not provide sufficient variation to evaluate the effect of wearing time on myopia progression.” Another 3-year clinical trial randomized 294 myopic children aged 7 to 11 years to wear soft multifocal contact lenses with either a high or medium add power, or single-vision soft lenses.23 While the high add power lenses significantly slowed myopia progression, longer wearing times did not enhance their effect. Although the latter two studies did not show a relationship between efficacy and wearing time, it is unclear whether there was absence of effect or insufficient spread or sensitivity of recording of wearing times.
SpectaclesCompliance has also been shown to influence the efficacy of myopia control spectacles. An obvious advantage of spectacles is their ease of application, but the counterpoint to this is that they can also easily be removed. Low myopes generally see well for near tasks without correction and may be tempted to remove spectacles for such tasks based on well-meaning, but ill-advised, advice from parents or practitioners or to alleviate, among other things, potential frame-related discomfort. A 2-year clinical trial randomly assigned 170 myopic children aged 8 to 13 years to wear spectacle lenses with highly aspherical lenslets (HALs), spectacle lenses with slightly aspherical lenslets, or single-vision spectacle lenses.24 Myopia progression in those wearing the HALs was significantly lower than those wearing single-vision spectacles (−0.66 vs. –1.46 D), as was axial elongation (0.34 vs. 0.69 mm). Full-time wear, defined as at least 12 hours per day, increased the myopia control efficacy to 0.96 D and 0.41 mm, while efficacy among part-time wearers was still clinically meaningful but only 0.57 D and 0.27 mm. In a similar clinical trial, 183 myopic children aged 8 to 13 years wore either Defocus Incorporated Multiple Segments spectacle lenses or single-vision spectacle lenses for 2 years.25 There was no relation between myopia control efficacy and wearing time, likely because mean wearing time exceeded 15 hours per day in both groups. Finally, in another clinical trial, compliance with spectacle lens wear was reported to be high during the first year,26 but subsequent analysis has been limited to the two-thirds of participants who met the criteria for full-time wearers, again demonstrating the critical nature of compliance (Rappon J, et al. IOVS 2022;63:E-Abstract 408).
AtropineThere are challenges associated with using atropine as the primary method for myopia management. Unlike optical options, atropine does not correct a patient's refractive error. Thus, the child will still need a refractive correction in addition to their atropine prescription. Furthermore, there may be less incentive for a patient to use the atropine on a regular basis because it does not provide any tangible benefit—it does not improve vision, and it does not make the child's eyes feel better as would an anti-inflammatory or anti-allergy drop. Indeed, atropine may induce discomfort, whether short-term from application of the drops if formulated with the appropriate pH27 or longer-term photophobia due to pupil dilation. The challenges associated with maintaining compliance may explain some of the apparent conflicting results in recent clinical trials of atropine for myopia control conducted in the United States. One 3-year clinical trial of 573 children aged 3 to 16 years found that 0.01% atropine produced a significant, but modest, reduction in myopia progression and axial elongation.28 In contrast, a smaller 2-year clinical trial found no such reduction with 0.01% atropine.29 The atropine in both clinical trials came from the same manufacturer, so the differences cannot be attributed to variations in formulation. One hypothesis is that the contrasting study findings may be due to differences in compliance. Alternatively, the studies may have measured essentially the same treatment effect but appear to have different outcomes because of random variation and the quirks of dichotomizing probability into a positive or negative acceptance of a hypothesis with the smaller study's statistical power possibly being a contributing factor.29 Compliance might also explain the apparent paradoxical finding from the former clinical trial that 0.02% atropine was less effective than 0.01% atropine.28
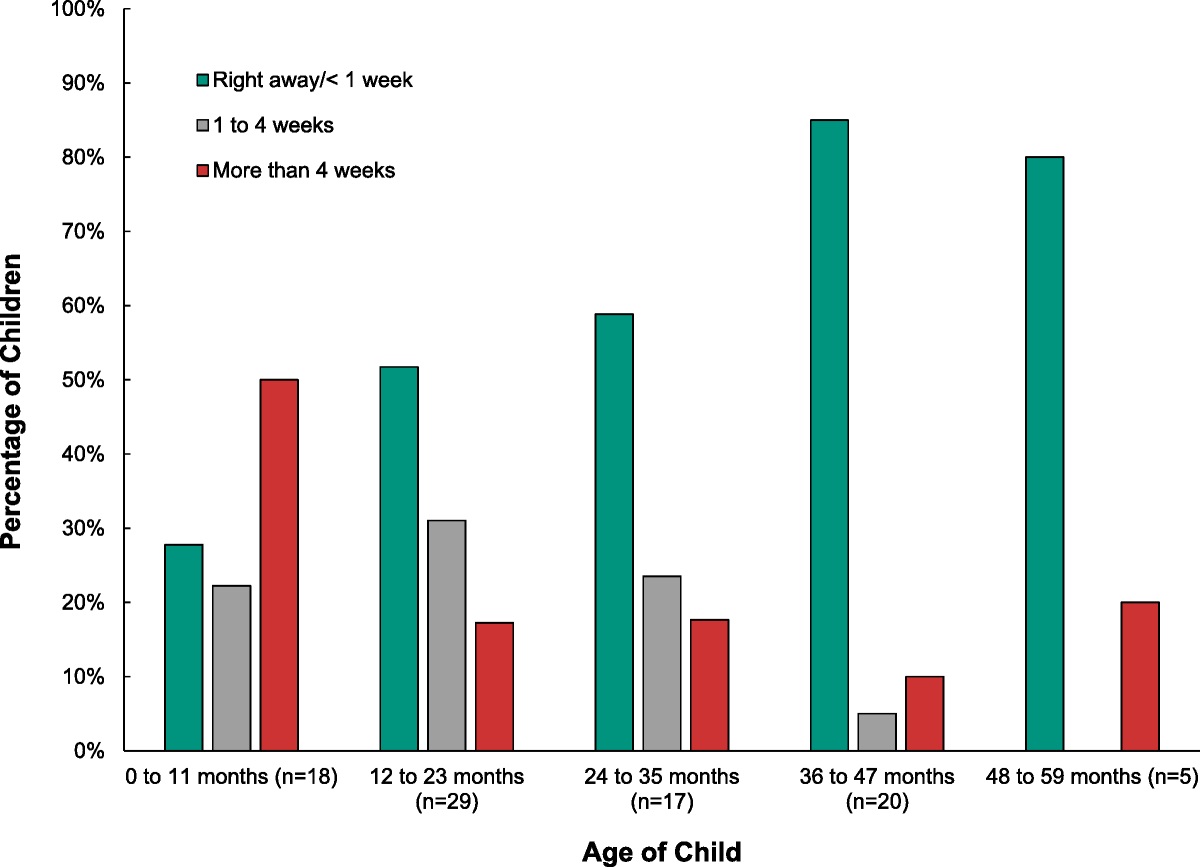
Compliance is a challenge for patients using eye drops for an extended period, and glaucoma management provides some useful insights. A California health maintenance organization study evaluated compliance over a 5-year period in 18,000 newly diagnosed glaucoma patients using computerized data on prescription fill rates in the second year after diagnosis.30 Compliance was calculated using a medication possession ratio—the number of days during which a patient had access to medication divided by the number of days in a period of interest. Compliance was not normally distributed but rather was bimodal (Fig. 1). While 20% of patients had a medication possession ratio close to 1, indicating they always had their drops on hand, over 30% had a medication possession ratio of zero, indicating that they never had a prescription available in the second year following diagnosis. The remaining 50% of patients were relatively evenly distributed among ratios between 0.1 and 0.9. Of course, even a high medication possession ratio does not guarantee compliance, as a patient may still not regularly use the eye drops in their possession. The authors did not evaluate treatment modification or other glaucoma interventions, including surgery, which may explain some of the patients with zero compliance, but the overall low compliance with medications is consistent with the literature.31–33
 FIGURE 1: Distribution of compliance among glaucoma patients in the second year after diagnosis. Replotted from Jones et al.30Orthokeratology
FIGURE 1: Distribution of compliance among glaucoma patients in the second year after diagnosis. Replotted from Jones et al.30Orthokeratology
With orthokeratology, failure to wear lenses on a consistent basis will result in poorer daytime vision, particularly later in the evening. In this regard, infrequent wear appears to result in discontinuation soon after fitting.34 None of the clinical trials of the influence of overnight orthokeratology on axial elongation appear to have assessed frequency and duration of wear.34–36 Studies of compliance with overnight orthokeratology typically focus on lens cleaning and storage rather than wearing time, and available data appear to be limited to cursory reporting of sleep habits.37
In summary, compliance can be an important determinant of myopia control efficacy. Given the relative ease with which spectacles may be removed, common sense suggests that compliance should be higher with contact lenses, particularly overnight orthokeratology where quality of vision and comfort play little role during most of the wear time. Likewise, the relative visual benefit implies that compliance should be expected to be higher with spectacles than with atropine.
QUALITY OF VISION SpectaclesThe effect of any myopia control intervention on vision must also be considered. With regard to spectacles, progressive addition lenses (PALs) offer good vision in primary gaze but have unwanted astigmatism in lateral areas of the lens. Of course, the modest efficacy of PALs renders this something of a moot point.7,38 In contrast, executive bifocals offer wide fields of good vision at distance and at near but are arguably the most cosmetically unacceptable spectacle lens option. Again, the efficacy of bifocal spectacles is, at best, equivocal.7,39–41 Myopia control lenses with peripheral lenslets also yield excellent visual acuity when patients look through the central 10-degree portion of the lenses,25,42 with reports of blurred vision rare and short lived.9 Patients report quality of vision, adaptation, and comfort similar to single-vision controls.25,42 Nonetheless, foveal high-contrast visual acuity through the periphery of the lens is reduced by around one line and slightly more for lower contrasts.43,44
Soft contact lensesContact lenses, in contrast, move with the eye and, in theory, unlike all of the above classes of spectacle lenses, offer the same quality of vision in all directions of gaze. The small increase in retinal image size associated with moving the correction from the spectacle plane to the cornea will have no meaningful influence on visual acuity in low myopia. The benefits are greater for higher myopia, but even with −10 D of myopia, improvement in visual acuity will be less than one line, as that requires a 25% increase in image size. Further, designs with a center distance zone can be expected to provide good visual acuity with high room illumination and consequent pupil constriction. Nevertheless, the simultaneous vision nature of myopia control soft lenses means that some reduction in visual acuity or subjective vision quality might be anticipated under conditions commonly encountered in day-to-day activities.
In the 3-year clinical trial of a dual-focus soft contact lens, visual acuity with the lens and a spectacle overrefraction was no different from that with single-vision soft lenses with an overrefraction.8,19 Presenting visual acuity was often worse with the single-vision lenses than the dual-focus lenses because of greater myopia progression.19 After 6 years of wear, over 90% of participants rated themselves as seeing “kind of well” or “really well” for a range of activities, with “really well” accounting for the vast majority of those responses.19 Likewise, visual disturbances such as ghosting or haloes were reported to be “not noticeable” or “noticeable, but not annoying” in 90% or more of children. Those children assigned to wear single-vision lenses for the first 3 years switched to dual-focus lenses thereafter. There was no significant difference in vision ratings 6 months after switching lens design, although three participants who discontinued at that point cited vision as the main reason, while another gave vision as a secondary reason for discontinuation.19 This suggests that older children may be more discriminating when it comes to their vision. A recent study in adults comparing vision with the dual-focus soft contact lens and a single-vision contact lens found that low-contrast visual acuity and contrast sensitivity were both significantly lower with the dual-focus lens.45
In the 6-month randomized clinical trial comparing three myopia control soft contact lenses with a single-vision lens, there was no significant difference in visual acuity at initial lens fitting for any lens group compared with best-sphere spectacle correction.21 Similar values were observed after 6 months of wear. Furthermore, over 90% of subjects in all wearing groups reported that they were “very happy” with how well they could see with their lenses. The main reported visual symptom was halos, but by 6 months, no more than 7% of any group reported this symptom. In one group, 14% reported usually or always noticing ghost images.
The 3-year clinical trial of high and medium add power soft contact lenses found that visual acuity with spherical overrefraction was no different from that with single-vision soft lenses with an overrefraction.23 Visual acuity was also measured using low contrast charts, where both high and medium add power lenses gave significantly poorer visual acuity, but the differences were less than two letters and considered by the authors to be “not clinically meaningful.”
OrthokeratologyWith regard to overnight orthokeratology, early careful studies in adults found no significant changes in high-contrast best-corrected visual acuity.46 Conversely low-contrast best-corrected visual acuity was reduced by 0.07 and 0.12 logMAR (around one line) with natural and dilated pupils, respectively, with the latter correlating with an increase in spherical aberration. One benefit of overnight orthokeratology is the temporary reduction of myopia and the associated elimination of a need for optical correction. Adults undergoing overnight orthokeratology show excellent uncorrected visual acuity and little change throughout the day.47–50 Corresponding data on visual performance and stability of vision in children undergoing overnight orthokeratology are scarce.51
A further important consideration in overnight orthokeratology wearers is presenting uncorrected visual acuity. The improvements in uncorrected visual acuity are relatively stable throughout the day, with very little regression in the 8 to 12 hours following lens removal, although these studies are limited to adult wearers.47–50 Consistent with findings in soft lens myopia control,19 presenting visual acuity in children wearing overnight orthokeratology was better than in single-vision wearers because of less myopia progression. For example, at the conclusion of a 2-year clinical trial, presenting visual acuity was +0.02 logMAR in the 37 children wearing overnight orthokeratology and +0.07 in the 41 spectacle wearers, a difference of half a line.34
A recent large school-based study examined 72,920 Chinese children aged 6 to 18 years, of whom 32,259 were myopic and 1021 were overnight orthokeratology wearers (3.1%).52 Among those wearing overnight orthokeratology, 127 participants (12%) had presenting visual acuity of 0.3 logMAR (20/40) or worse. It is unknown whether this is due to myopia progression, poor compliance, inadequate lens fit, or some combination, although these children tended to have higher levels of myopia and slept less. Corresponding data for spectacle-wearing myopes are not presented, but a previous paper from the same study found that presenting visual acuity was 0.3 logMAR or worse in 34,298 of 189,349 myopic children, a rate of 18%.53 Again, the reasons for this are unclear. Thus, reduced presenting visual acuity appears to better in overnight orthokeratology wearers than those uncorrected or corrected with spectacles. Indeed, compliance with spectacle wear is consistently low among Chinese children, particularly boys.54 The challenge of spectacle compliance is not limited to China. A recent meta-analysis of 23 studies from 14 countries found a mean compliance of 40%,55 although some studies found better compliance in myopic children than those with hyperopia. It is unclear whether these values would be higher for myopia control spectacles. Finally, when removed, spectacles can be lost. Indeed, broken or lost spectacles are among the main reported causes of lack of compliance.55
Comparisons among modalitiesA recent study compared central and peripheral vision with three different myopia control modalities—HAL spectacle lenses, DISC soft contact lenses, and overnight orthokeratology—with single-vision spectacles in 20 myopic children aged 8 to 16 years.56 Central contrast sensitivity was lower with the DISC lenses than with single-vision and HAL spectacle lenses. Peripheral findings were equivocal, with differences among lenses varying with both the visual field quadrant and the task. For example, HALs reduced contrast sensitivity in the temporal visual field compared with orthokeratology. Likewise, orthokeratology increased contrast sensitivity in the superior visual field relative to single-vision and HALs. HALs also reduced peripheral motion sensitivity relative to orthokeratology for contraction but not the other three directions of motion. When considering the improvements in performance with orthokeratology, it is important to note that participants were first tested with the other three lenses and again after 1 month of overnight orthokeratology wear. Thus, training effects may have played a role.
Vision-specific quality-of-life questionnaires have also been applied to myopia-control soft lenses and orthokeratology and are discussed below in the “Quality of Life” section.
AtropineAtropine drops affect near vision and create photophobia due to the mydriatic and cycloplegic actions in a dose-dependent fashion. At the lowest concentrations (<0.1%), these effects have been observed to be modest in Asian populations. In a clinical trial of 400 myopic children aged 6 to 12 years randomized to different concentrations of atropine, accommodative amplitude was reduced to 2.2, 3.8, and 11.3 D among those receiving 0.5%, 0.1%, and 0.01% atropine, respectively.57 Correspondingly, among the 234 children aged 8 to 10 years, 70%, 61%, and 6% required progressive addition lenses. Near visual acuity was reduced by around three lines in those receiving 0.5% atropine, but best-corrected distance visual acuity was unchanged in any of the groups. All children received photochromic lenses. While symptoms were not reported, both photopic and mesopic pupil sizes in those receiving 0.01% increased by 1 mm compared with around 3 mm in the other groups.
In a subsequent clinical trial, 438 myopic children aged 4 to 12 years were randomly assigned to receive 0.05%, 0.025%, and 0.01% atropine or placebo eye drops.58 Pupil dilation averaged only 1 mm in the highest concentration, with an accompanying 2-D reduction in accommodative amplitude. Neither best-corrected distance visual acuity nor near visual acuity was reduced in any of the groups. Participants were offered photochromic spectacles, and around a third of those using atropine requested them—but so did 41% of those in the placebo group. Progressive addition lenses were available to those experiencing difficulty with near vision, but only four children (less than 1%) requested them, including one in the placebo group. Subsequently, in a recent randomized clinical trial of 0.01% and 0.02% atropine versus placebo, in 573, mostly White, myopic children aged 3 to 16 years, neither photochromic nor progressive addition lenses were offered.28 Photophobia was rarely reported (20 total, 4.5% of 0.02% atropine group), as was blurred vision (6 total). In summary, low-concentration atropine appears to have a modest influence on near vision and minimal effect on distance vision.
QUALITY OF LIFEA further factor that applies to all facets of refractive care is quality of life. Indeed, much has been written regarding the benefits of laser refractive surgery in this regard.59,60 For all quality-of-life instruments, higher scores represent better performance and perceptions. In a prospective study using the National Eye Institute Refractive Error Quality of Life (NEI-RQL) instrument, the largest improvements following surgical correction of myopia or hyperopia were seen for expectations, activity limitations, dependence on correction, appearance, and satisfaction with correction.59 In a cross-sectional study using the Quality of Life Impact of Refractive Correction questionnaire, the largest differences between those who had undergone refractive surgery and spectacle or contact lens wearers were for convenience followed by functioning, symptoms, economic concerns, and health concerns.60
Soft contact lensesA number of studies have assessed quality of life in children wearing different refractive error correction modalities—both single vision and those used in myopia management. The Adolescent and Child Health Initiative to Encourage Vision Empowerment study randomly assigned 484 myopic children aged 8 to 11 years to wear spectacles or soft contact lenses for 3 years.61 Global self-worth, assessed with the Self-Perception Profile for Children Global Self-Worth scale,62 was not affected by contact lens wear. In contrast, perceptions of physical appearance, athletic competence, and social acceptance were all greater among contact lens wearers. The authors also assessed vision-related quality of life using the Pediatric Refractive Error Profile (PREP).63 During the 3-year study, overall PREP scores improved significantly more for contact lens wearers than for spectacle wearers (14 ± 18 vs. 2 ± 15 units on a 100-point scale).64 The 3 of the 11 scales with the greatest improvement in quality of life for contact lens wearers were activities, appearance, and satisfaction with correction, while academics and symptoms showed the least change.
Two studies have assessed vision-related quality of life in children wearing myopia control soft contact lenses, both using versions of the PREP. The first was part of a 2-year study comparing dual-focus soft contact lenses and single-vision spectacles in myopic children aged 8 to 12 years.65 The PREP questionnaire was administered at 12 and 24 months. Among the 74 children completing the study, those wearing dual-focus contact lenses had higher scores than those wearing spectacles for appearance, satisfaction, activities, handling, and peer perceptions but lower scores for near vision. A 6-year study of the dual-focus contact lenses did not formally assess vision-related quality of life but found satisfaction with the lenses to be substantially higher than with spectacles.19
A more recent study recruited myopic children aged 7 to 12 years, who had been wearing DISC lenses or single-vision spectacles for at least 6 months.66 Vision-related quality of life was assessed with the Chinese version of the PREP questionnaire.67 The 54 participants wearing DISC lenses scored significantly higher than the 56 wearing single-vision spectacles for five of the seven scales: vision, appearance, activities, peer perception, and overall.
In summary, soft contact lenses, be they single vision or for myopia control, improve vision-related quality of life in children compared with spectacles, particularly in the areas of activities and appearance.
OrthokeratologyVision-related quality of life has also been evaluated in overnight orthokeratology—initially in adults. The first study administered the National Eye Institute Refractive Error Quality of Life Instrument (NEI-RQL-42) to 20 myopic adults before and 1 month after being successfully fit with overnight orthokeratology.68 Significant improvements were found in 2 of the 13 NEI-RQL-42 subscales: symptoms and dependence on correction, while there was a worsening for the glare subscale.
The same instrument was used to compare vision-related quality of life between overnight orthokeratology and soft contact lenses in a randomized crossover clinical trial.69 Eighty-one myopic adults, aged 18 to 40 years, were randomly assigned to wear one mode of contact lens for 8 weeks. After a washout period, they wore the other mode for 8 weeks. Of the enrolled patients, 65 completed the study. Similar to the earlier report,68 wearing overnight orthokeratology was associated with higher subscale scores for activity limitations, symptoms, and dependence on correction but poorer scores for the glare subscale.69
More recently, studies have been conducted on children wearing overnight orthokeratology. The first was part of a longitudinal comparison of overnight orthokeratology and spectacles in myopic children aged 6 to 12 years.70 The PREP questionnaire was administered at 12 and 24 months. For 31 children fitted with orthokeratology and 30 with spectacles, those wearing orthokeratology rated overall vision, far vision, symptoms, appearance, satisfaction, activities, academic performance, handling, peer perceptions, and the overall score significantly higher than those wearing spectacles. Conversely, near vision was rated higher by those wearing spectacles.
A subsequent study compared vision-related quality of life using the Chinese version of the PREP in myopic children aged 8 to 12 years who had been wearing overnight orthokeratology or single-vision spectacles for at least the prior 12 months.71 Among 40 children (20 in each group), overall vision, far vision, appearance, satisfaction, activities, and peer perception scores were all higher in the overnight orthokeratology wearers than in the spectacle wearers. In contrast, the handling of optical correction score was worse in the overnight orthokeratology group. It is worth noting that the PREP was minimally modified for orthokeratology wearers; for example, “when I wear my glasses” was replaced with “after I wore ortho-k lenses.” The same instrument was used in a subsequent cross-sectional study of 45 myopic children wearing overnight orthokeratology lenses and 25 wearing spectacles (mean age, 10.9 ± 0.7 years).72 The mean scores were higher in the overnight orthokeratology wearers than the spectacle wearers for all the scales except peer perception.
Comparisons among modalitiesA recent study compared quality of life in myopic adults and children who were established spectacle, soft contact lens, or orthokeratology using the PREP2 (a modified version of the original PREP survey designed to improve repeatability and to reduce bias).73 Among the 49 children, only the activities score differed with correction type, with those of the spectacle wearers lower than those of both contact lens groups. Finally, a recent cross-sectional study reported broader health-related quality of life in myopic children aged 7 to 17 years wearing overnight orthokeratology, myopia control spectacles with peripheral lenslets, and single-vision spectacles.74 Of the 648 participants, there were over 200 in each of the three groups, and the average utility score derived from the Child Health Utility—Nine Dimensions questionnaire was 0.94. Children wearing myopia control spectacles had significantly higher utility scores (0.96) than those wearing single-vision spectacles (0.93) and orthokeratology (0.93), although these differences are small, and the scores for all groups are very high.
SAFETYThe final consideration to be discussed is safety. While the risk of adverse events is small with all major myopia control interventions, they should not be ignored.
AtropineWith atropine, photophobia and near vision difficulties may be anticipated, but as discussed above, they are concentration dependent. The most common other ocular side effect in one clinical trial was allergic conjunctivitis, occurring in 3 to 7% of children in each arm, including those receiving placebo, suggesting that the preservative or other excipient may be the causative agent.58 There may be a risk of systemic absorption, but in a large number of clinical trials for myopia control57,58,75 and for penalization therapy for amblyopia,76–79 involving hundreds of children, there have been no reports of systemic adverse events related to topical atropine. Nonetheless, it should be noted that data for long-term use, say over a decade, at effective concentrations are not available. A report by the American Academy of Ophthalmology on “Atropine for the Prevention of Myopia Progression in Children” is silent regarding safety.80
SpectaclesSpectacles could be considered the safest of myopia control modalities, particularly as, in the United States, children are prescribed polycarbonate lenses. The minimal physical risks from lens breakage are unlikely to be increased by these novel designs. There are, nonetheless, some caveats. Spectacle wear has been associated with increased bicycle crashes in children, but there was no association with myopia per se,81 suggesting any increased risk may be due to peripheral visual field restrictions. It is unclear whether some spectacle designs for myopia control would exacerbate this effect. Multifocal spectacle lenses are associated with an increased risk of falls in the elderly,82–84 but the spatial distortion (swim) and prismatic effects (jump) that are a hallmark of those lenses should not be present in myopia control lenses with peripheral lenslets.
Soft contact lensesThe adverse events associated with soft contact lens wear are well documented, and those affecting the cornea are collectively termed “corneal infiltrative events.”85–87 Over 90% are easily managed and pose little threat to vision.86,88 Microbial keratitis is a rare subset of these events, with an incidence of between 2 and 4 per 10,000 patient-years for daily-wear patients,89 with an average of 5% resulting in vision loss.90–93 Most myopia control contact lenses are daily disposable replacement schedule,8,21 and the elimination of contact lens storage and solutions removes two important risk factors for microbial keratitis from consideration.94 Regardless, the risks associated with myopia control lenses should not be any different from conventional single-vision contact lenses.
Soft contact lens wear appears to be safer in 8- to 12-year-olds than in adolescents and young adults. For example, in a retrospective study of 3549 patients with an average of 20 months of lens wear, the risk of a corneal infiltrative event increased in a nonlinear fashion up to age 21 years and then decreased, with the peak years at risk from age 15 to 25 years.86 The low rates of corneal infiltrative events and microbial keratitis in patients 8 to 12 years old are supported by prospective studies, comprehensively reviewed elsewhere.95,96
OrthokeratologyIn the early years of the millennium, there were a large number of reports of microbial keratitis associated with overnight orthokeratology.97 Nearly all of these cases were from East Asia, notably China, Taiwan, and Hong Kong, and most occurred in children. These cases decreased substantially after 2002, when the Chinese Food and Drug Administration introduced regulations covering inspection and registration for manufacturers, training and certification of practitioners, and minimal requirements for instrumentation and management.98 Subsequently, the incidence of microbial keratitis associated with overnight orthokeratology in children was quantified, although not in East Asia. A retrospective study of 1317 randomly selected overnight orthokeratology wearers in the United States identified eight corneal infiltrative events, of which two were classified as microbial keratitis.99 Both occurred in children, but neither resulted in a loss of visual acuity. The overall estimated incidence of microbial keratitis was 8 per 10,000 patient-years. For children, the estimated incidence was 14 per 10,000 patient-years. A second study in Russia identified five cases of microbial keratitis without permanent loss of vision in children wearing overnight orthokeratology lenses and estimated the incidence as 5 per 10,000 patient-years.100
In conclusion, microbial keratitis is rare in contact lenses wear and highly unlikely to result in permanent loss of vision, particularly in children. Furthermore, the benefits of myopia control far outweigh these risks.89 The risk can be mitigated by daily disposable lenses and frequently reinforcing the importance of good hygiene and compliance.94
SUMMARY AND OTHER CONSIDERATIONSWe have reviewed some important considerations when deciding among different myopia control options. Professional, regulatory, and cultural differences mean that some approaches are favored in some regions,101 and biases on the part of practitioners, parents, or both play a role. Parental opinion is of particular importance in determining which modality practitioners will prescribe. For example, among Hong Kong Chinese parents responding to two advertisements for myopia control studies—one for overnight orthokeratology and one for soft lenses—86% of them were aware of overnight orthokeratology as a myopia control modality.102 Overnight orthokeratology was the preferred approach for 49% of the parents responding to the orthokeratology advertisement and 38% for the soft lens advertisement. The parents were open to the use of contact lenses for myopia control in young children and regarding myopia control contact lenses as a “treatment” rather than a visual aid. They were more conservative in using contact lenses solely for vision correction in children. In contrast, a recent online survey of Spanish parents found that 52% were unaware of any myopia control method, and orthokeratology was the least well known (22%).103 While 93% of parents would consider at least one myopia control strategy for their child, only 18% would entertain overnight orthokeratology. Notwithstanding the different survey methods and the 8 years between publications, the differences in parental attitudes between countries are profound.102,103 Ophthalmologists sometimes make glib statements in publications regarding contact safety104,105 that are not supported by the data presented above.95,96,99,100 This may be driven by their own professional experience and seeing only the most serious cases of microbial keratitis.
Other considerations will influence a practitioner's recommendation. Treating higher myopes is a challenge; soft contact lens parameter availability may be a limiting factor; orthokeratology can only provide reversal of a certain amount of myopia, and supplementary correction with spectacles may be necessary; and higher myopes may be reluctant spectacle lens wearers because of lens thickness, and myopia control designs may not be available in high refractive index spectacle lens materials. Furthermore, some soft contact lenses may not be available in toric form for those with significant astigmatism. While most myopia control modalities have an optical design and thus efficacy, which is independent of refractive error, an exception is overnight orthokeratology where efficacy is less in lower myopia.106,107 This may be attributed to the fact that the central corneal flattening and thus the induced peripheral myopic defocus are directly proportional to the level of myopia.
Contact lenses will ultimately require more practitioner time, including insertion and removal training.108 With overnight orthokeratology, a parent may insert, remove, and clean the lenses, even in older children, which may introduce an inconvenience factor.109 On the other hand, the cleaning and storage of lenses are obviated with daily disposable soft contact lenses. Contact lenses are an attractive option for active children, although, for swimmers, orthokeratology is more convenient. A final, but by no means insignificant, consideration is cost. While atropine drops plus single-vision spectacles may be the cheapest of all myopia management options, this needs to be weighed against the relative lack of efficacy of 0.01% atropine plus the compliance challenges mentioned above.
The availability of a range of effective modalities enables the clinician to exercise their judgment when discussing the treatment plan with the patient and their parents. While discussing four key parameters—compliance, quality of vision, quality of life, and safety—one could make a case for compliance being the most important, but quality of vision and comfort will clearly influence compliance, which, in turn, drives efficacy. Most clinical trials of myopia control soft contact lenses report high daily wear times.8,21,23 The rare instance where all-day wear was difficult to achieve was likely due to quality of vision, comfort, or both.18 Thus, daily disposal myopia control contact lenses and overnight orthokeratology are an attractive option. They also provide better vision-related quality of life than spectacles and carry a very low risk when used appropriately. A further benefit of overnight orthokeratology is the elimination of a need for optical correction throughout the day. Compliance data suggest that some spectacle lenses may be less well tolerated than others, leading to removal for near vision activities (Rappon J, et al. IOVS 2022;63:E-Abstract 408) and likely reducing efficacy. Folklore may lead parents to encourage removal of spectacles for reading, and they should be counseled that full-time wear will lead to the best results.24 Finally, we would argue that successful myopia control relies on motivation on the part of both patient and parents.
REFERENCES 1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016;123:1036–42. 2. Vitale S, Sperduto RD, Ferris FL 3rd. Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol 2009;127:1632–9. 3. Tideman JW, Snabel MC, Tedja MS, et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol 2016;134:1355–63. 4. Bullimore MA, Brennan NA. The underestimated role of myopia in uncorrectable visual impairment in the United States. Sci Rep 2023;13:15283. 5. Yam JC, Zhang XJ, Zhang Y, et al. Effect of low-concentration atropine eyedrops vs placebo on myopia incidence in children: The LAMP2 randomized clinical trial. JAMA 2023;329:472–81. 6. Jawaid I, Saunders K, Hammond CJ, et al. Low concentration atropine and myopia: A narrative review of the evidence for United Kingdom-based practitioners. Eye (Lond) 2024;38:434–41. 7. Logan NS, Bullimore MA. Optical interventions for myopia control. Eye (Lond) 2024;38:455–63. 8. Chamberlain P, Peixoto-de-Matos SC, Logan NS, et al. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci 2019;96:556–67. 9. Li X, Huang Y, Yin Z, et al. Myopia control efficacy of spectacle lenses with aspherical lenslets: Results of a 3-year follow-up study. Am J Ophthalmol 2023;253:160–8. 10. Lam CS, Tang WC, Lee PH, et al. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: Results of a 3-year follow-up study. Br J Ophthalmol 2022;106:1110–4. 11. Yam JC, Zhang XJ, Zhang Y, et al. Three-year clinical trial of Low-concentration Atropine for Myopia Progression (LAMP) study: Continued versus washout: Phase 3 report. Ophthalmology 2022;129:308–21. 12. Bullimore MA, Brennan NA. Efficacy in myopia control: The Low-concentration Atropine for Myopia Progression (LAMP) study. Ophthalmology 2023;130:771–2. 13. Hiraoka T, Kakita T, Okamoto F, et al. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: A 5-year follow-up study. Invest Ophthalmol Vis Sci 2012;53:3913–9. 14. Bullimore MA, Brennan NA. Myopia control: Why each diopter matters. Optom Vis Sci 2019;96:463–5. 15. Brennan NA, Toubouti YM, Cheng X, et al. Efficacy in myopia control. Prog Retin Eye Res 2021;83:100923. 16. Bullimore MA, Brennan NA. Juvenile-onset myopia—who to treat and how to evaluate success. Eye (Lond) 2024;38:450–4. 17. Horn CR. The assessment of therapeutic compliance by asthmatic patients. Eur Respir J 1992;5:126–7. 18. Lam CS, Tang WC, Tse DY, et al. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: A 2-year randomised clinical trial. Br J Ophthalmol 2014;98:40–5. 19. Lumb E, Sulley A, Logan NS, et al. Six years of wearer experience in children participating in a myopia control study of MiSight® 1 day. Cont Lens Anterior Eye 2023;46(4):101849. 20. Ruiz-Pomeda A, Perez-Sanchez B, Valls I, et al. MiSight Assessment Study Spain (MASS). A 2-year randomized clinical trial. Graefes Arch Clin Exp Ophthalmol 2018;256:1011–21. 21. Cheng X, Xu J, Brennan NA. Randomized trial of soft contact lenses with novel ring focus for controlling myopia progression. Ophthalmol Sci 2023;3:100232. 22. Sankaridurg P, Bakaraju RC, Naduvilath T, et al. Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomised clinical trial. Ophthalmic Physiol Opt 2019;39:294–307. 23. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: The BLINK randomized clinical trial. JAMA 2020;324:571–80. 24. Bao J, Huang Y, Li X, et al. Spectacle lenses with aspherical lenslets for myopia control vs single-vision spectacle lenses: A randomized clinical trial. JAMA Ophthalmol 2022;140:472–8. 25. Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: A 2-year randomised clinical trial. Br J Ophthalmol 2020;104:363–8. 26. Rappon J, Chung C, Young G, et al. Control of myopia using diffusion optics spectacle lenses: 12-month results of a randomised controlled, efficacy and safety study (CYPRESS). Br J Ophthalmol 2023;107:1709–15. 27. Richdale K, Skidmore KV, Tomiyama ES, et al. Compounded 0.01% atropine—what's in the bottle? Eye Contact Lens 2023;49:219–23. 28. Zadnik K, Schulman E, Flitcroft I, et al. Efficacy and safety of 0.01% and 0.02% atropine for the treatment of pediatric myopia progression over 3 years: A randomized clinical trial. JAMA Ophthalmol 2023;141:990–9. 29. Repka MX, Weise KK, Chandler DL, et al. Low-dose 0.01% atropine eye drops vs placebo for myopia control: A randomized clinical trial. JAMA Ophthalmol 2023;141:756–65. 30. Jones JP, Fong DS, Fang EN, et al. Characterization of glaucoma medication adherence in Kaiser Permanente Southern California. J Glaucoma 201
留言 (0)