This real-world retrospective study in patients with severe asthma using data from a large US claims database found that both burst and chronic SCS use, even at low (≤ 6 mg/day) doses, significantly increases the odds of developing SCS-related complications. Similarly, burst and chronic SCS use in this population was linked with significantly higher rates of HCRU due to SCS-related complications, with even low chronic SCS doses associated with more frequent IP and other HCRU visits. These data support existing evidence of the well-documented and wide-reaching adverse effects associated with SCS use by highlighting a dose-dependent increase in the risk of complications among patients with severe asthma who continue to be frequent users of SCS therapy [5,6,7,8,9,10, 29]. They also suggest that even low doses of SCS are associated with complications and that complications occur with both maintenance and burst SCS use. Further, this study provides updated insight into the association between SCS use with related complications and HCRU in the era of biologic therapy.
In patients with a medium SCS dose or higher, including those with continuous high SCS dose and those with ≥ 3 or ≥ 4 SCS bursts, the odds of developing any SCS-related complication were 1.3–1.6 times greater than in the non/burst SCS use cohort. Notably, the increase in the risk of developing SCS-related complications was dose-dependent, with the greatest increase observed for patients with continuous high SCS use. These results build on previous findings that demonstrated the increased risk of SCS-related complications with greater SCS use in patients with asthma [5,6,7,8]. For example, in a retrospective claims analysis conducted in the US between 1997 and 2013, patients with medium (> 6–12 mg/day) and high (> 12 mg/day) SCS exposure had significantly higher risks of several different SCS-related complications versus those with low (≤ 6 mg/day) exposure, with ORs by complication type ranging from 1.29 to 2.12 for medium-dose users and 1.23 to 1.96 for high-dose users [7]. A further analysis of this dataset found a significant dose-response relationship between SCS exposure and any SCS-related complication, with ORs versus non-users increasing from 2.03 in low-dose (≤ 6 mg/day) users to 3.64 in high-dose (> 12 mg/day) users [8]. Similarly, in another retrospective claims analysis conducted in the US between 2003 and 2014, the odds of developing SCS-related complications increased in a dose-dependent manner with ORs compared with non-users ranging from 2.50 in patients with low SCS exposure (< 5 mg/day) to 3.32 in patients with high exposure (> 10 mg/day) [6]. The odds of developing any SCS-related complication reported in our study were lower in comparison to the studies conducted in 1997–2013 and 2003–2014 [6, 8], which may reflect the ongoing shift from regular use of SCS within asthma management. Together these data highlight the significant association between SCS dose and SCS-related complications in the asthma population and support the guideline-recommended aim of minimizing SCS use in these patients [2].
In line with previous findings [6,7,8], the current study found dose-dependent increases in the risk of acute gastrointestinal, cardiovascular and immune-system related complications as well as chronic cardiovascular, metabolic and endocrine, central nervous system, bone- and muscle-related, ophthalmologic, and hematologic/oncologic complications. Notably, even patients with low SCS exposure had increased risk of developing acute gastrointestinal and immune-system related complications as well as chronic bone- and muscle-related and hematologic/oncologic complications compared with the non/burst SCS use cohort. These findings are largely consistent with those from a previous focused literature review observing an increased risk of these complications with low-dose SCS versus no exposure among patients with severe asthma [35]. For other complications with low-dose versus no SCS exposure, results have been more mixed, with two studies finding no increase in the risk of cardiovascular complications, and for metabolic and ophthalmologic events, one study each showing a positive association and no association; [35] this largely accords with the lack of a significantly increased risk for these complications with low-dose SCS use in the current study. However, when patients with any SCS exposure during the follow-up period were excluded from the non/burst-SCS use cohort in a sensitivity analysis, the odds of all except ophthalmologic SCS-related complications were increased in the low-dose SCS subgroup compared with the modified non/burst-SCS use cohort. Overall, these data indicate an increased risk of complications even among those with low SCS use.
In addition to the increased risk of SCS-related complications, this study found higher rates of HCRU associated with SCS-related complications among patients with medium-dose SCS use or greater, with RRs versus non/burst SCS users ranging between 1.14 and 2.12. While there was some indication that higher SCS exposure correlated with higher HCRU than lower exposure, the dose-response relationship was not as clear as for SCS-related complications. An association between increased SCS exposure and higher HCRU due to SCS-related complications has also been found in previous retrospective claim studies [6,7,8]. Two of these studies also found that, compared with no SCS use even low SCS doses were associated with an increased rate of IP and other HCRU visits, consistent with the current study [6, 8]. Interestingly, Dalal et al., also found that low doses of SCS were associated with an increased rate of OP and ER visits compared with no SCS use [6]. Together, these findings indicate that beyond SCS-related complications, even low doses of SCS are associated with higher HCRU, suggesting a need for alternative corticosteroid-sparing management strategies among patients with severe asthma.
In the current study, baseline data generally showed higher comorbidity and concomitant medication use in SCS users versus non/burst-SCS users as well as higher all-cause and asthma-related healthcare costs. The proportion of SCS users without any controller therapy use appeared high at nearly 30%, which may indicate that some patients in the current study were using SCS as their controller therapy. These results appeared to align with other studies in asthma which did not require patients to be taking controller therapy. For example, in one claims analysis of patients with non-allergic asthma, 21.5% received fixed-dose ICS/ long-acting β2-agonists (LABA) during a 12-month baseline period, which was lower than the 42.5% during a 6-month baseline period in the current study [36]. While we did not collect data on healthcare costs during the follow-up period, the baseline differences may indicate that follow-up costs would also have been higher in SCS users, although their relationship with SCS-related complications is unclear. Outside of this study, it has been shown that healthcare costs are higher in SCS versus non-SCS users, with the costs associated with SCS-related complications increasing with SCS dose [5,6,7,8,9]. When combined with the adverse effects associated with SCS use, the higher healthcare costs among SCS users may be a further supporting factor for the use of SCS-sparing medications, such as biologics, in patients with severe asthma [16, 19, 20, 22, 24]. Furthermore, the cost effectiveness of biologic treatments has been demonstrated in a number of studies, particularly when treatment is targeted to specific responder populations [27, 28, 37, 38].
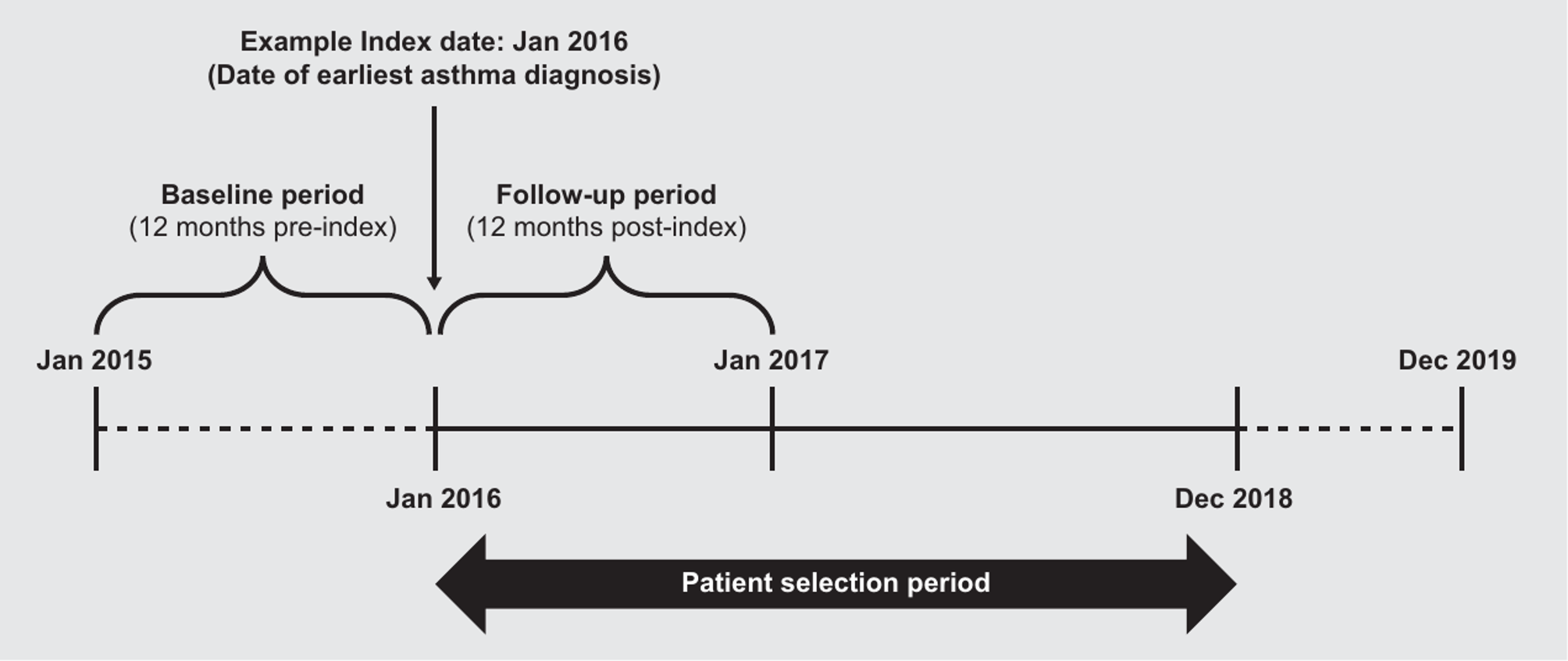
There are several limitations to the current study. As with other claims-based analyses, the data used were collected for payment rather than research purposes and are subject to coding limitations and may contain data entry errors. In particular, the categorization of complications as acute or chronic was based on the presence of an associated diagnosis code, which is contingent upon the treating physician’s judgement. As noted previously, the same caveat applies to HCRU given that encounters with a diagnosis code indicative of an SCS-related complication could also be due to uncontrolled asthma. Also, the presence of a dispensed medication does not indicate that the medication was taken as prescribed, nor that it was taken on the date of dispensing. In addition, patients with SCS bursts only or no bursts were not evaluated separately in this analysis. It should also be noted that eligibility for the non/burst-SCS use cohort precluded continuous SCS exposure for ≥ 6 months (the same criteria that defined patients in the SCS cohort as having severe asthma); consequently, differences in asthma severity between cohorts may have potentially impacted outcome differences between cohorts. Next, as ICS was not included in the definition of SCS use, it is possible that corticosteroid exposure was underestimated. However, since the bioavailability of ICS is lower than that of SCS, the impact of this exclusion is expected to be small. Additionally, the claims database used in this analysis includes data from 2014, prior to approval of several biologics for severe asthma in the US [11, 15, 17, 18]. However, the vast majority of patients included in the study had index dates after 2015. Therefore, the inclusion of data from 2014 may not have had a substantial effect on the relevance of this data for understanding the impact of SCS use since the introduction of biologic therapies. Finally, results may not be generalizable beyond the commercial and Medicare insurance population used. Nonetheless, these data provide valuable information on the burden of SCS use in patients with severe asthma and support a reduction of their use wherever possible in this population.









留言 (0)