The results of the present retrospective cohort study provide an epidemiological description of infants at higher risk for severe RSV infection and related hospitalization in Italy. In particular, descriptive analyses focused on socio-demographics at birth and on specific outcomes registered at follow-up during the first year of life: hospitalizations associated with RSV and URA infections, related HCRU, palivizumab administration and drug consumption by specific categories. According to the present findings, mothers’ socio-demographic characteristics appeared similar among the study cohorts, while infants’ socio-demographic characteristics and study outcomes revealed that different levels of vulnerability exist between the study cohorts. Indeed, presence of clinical conditions, especially BPD and/or RDS, is more frequently associated with severe RSV hospitalizations and URA hospitalizations, palivizumab administration and drug consumption, mainly during the first year of follow-up. The exploration of concomitant risk conditions in our sample, showed that BPD (and/or RDS) diagnosis is more frequently associated with other risk conditions, compared to CHD diagnosis and prematurity, suggesting that the poorer clinical outcomes found in BPD-RDS cohort compared to the other cohorts may be also related to the presence of overlapped clinical and risk conditions.
The prevalence of concomitant BPD (and/or RDS), CHD, early and moderate prematurity was differentially distributed among the cohorts. Specifically, while the Preterm cohort was predominantly composed by moderate preterm infants without concomitant BPD (and/or RDS) or CHD, early prematurity condition highly overlapped with the other risk conditions. As a result, early preterm infants were only 1.8% of the Preterm cohort. In particular, a strong association between early prematurity and BPD (and/or RDS) was found in our study. Indeed, considering the overall number of early preterm infants, about 80.0% (366/454) were in BPD-RDS cohort and about 50.0% (219/454) had only BPD (and/or RDS). These findings are in line with previous studies indicating that incidence of BPD increases as gestational age decreases [32,33,34,35]. In particular, Mowitzel and colleagues, using Medicaid databases, found that in a cohort of extremely preterm infants (WGA <28), excluding those with diagnosis of CHD, presence of BPD was found in 61.9% of infants [36]. In previous studies, involving extremely preterm infants with WGA between 22 and 28, BPD diagnosis was performed using clinical database and the resulting percentage was around 50.0% [32, 34]. Despite this value is apparently lower compared to our, percentage rose to 75.0% in infants with WGA 22-24 [34], suggesting that in our sample there might be a huge number of infants born between 22 and 24 WGA, however, since we did not investigate distribution of newborns according to WGA among early preterm infants, this hypothesis is not verifiable. In addition, as already reported in the past [32], different diagnostic criteria used among hospitals, may influence the number of BPD diagnoses, and make comparisons difficult. Moreover, a recent systematic literature review reported a wide range of global BPD incidence in extremely preterm infants, reflecting how different diagnostic criteria and care practices applied across institutions may influence these values [23].
For what concern CHD, our descriptive analyses revealed that this risk condition, in contrast to BPD (and/or RDS), is predominantly found in infants born at term (83.9%), while only 0.6% of infants in CHD cohort were extremely preterm. However, we found a considerable number of infants with CHD among BPD-RDS cohort, especially among preterm infants. These findings are supported by previous works where preterm infants with CHD showed a higher likelihood to have BPD compared to those without CHD [37, 38]. Despite an explanation of the increased frequency of BPD among preterm infants with CHD is still not clear, a literature review focused on preclinical and clinical studies reported that BPD condition is strongly associated with presence of patent ductus arteriosus, one of the most common congenital heart diseases [25]. However, other studies investigating the effect of pharmacological or surgical closure of the patent ductus arteriosus on BPD on set, failed to find a decrease in the incidence of the comorbidity after surgical or pharmacological interventions [39].
Furthermore, we found that BPD-RDS infants were the ones with the lowest birth weight and the longest duration of birth hospitalization, and these results worsened as gestational age decreased. These findings are in line with many previous studies where, in addition to WGA, also low birth weight was found as strong risk factor for developing BPD [40, 41], and prolonged hospitalization stay after birth was found in extremely preterm infants with BPD diagnosis, compared to those without [41, 42].
Our findings regarding sociodemographic information and concomitant risk conditions in study cohorts, supported by previous evidence, suggest that BPD-RDS cohort is the most fragile, however, the contribution of other risk conditions to the higher vulnerability found in this cohort is not negligible, since early prematurity, together with CHD, are strongly associated with BPD (and/or RDS) diagnosis.
As extensively reported in the literature [15, 43,44,45], the first year of life, corresponding to the first year of follow-up of our population, was a more critical period in terms of RSV hospitalizations compared to the second year. Furthermore, over the first 12 months of life, the first 6 months resulted as even more crucial, since more than 70.0% of RSV hospitalization in each cohort occurred during this period, and this evidence is supported by previous studies [15, 44]. Notably, in the study by Kuhdari and colleagues, where RSV hospitalizations were evaluated during the period 2001-2014 in the overall Italian population, it was estimated that 93.0% of RSV hospitalizations in infants and children between 0 and 2 years, occurred in infants with less than 1 year of age and was calculated a rate of 674/100,000 inhabitants versus 1.5/100,000 inhabitants for infants less than 1 years of age and children between 1 and 4 years of age respectively. Compared to our results, the value obtained was slightly lower, since we obtained a rate of 2/100 infants. However, this discrepancy is understandable because Kuhdari's study included the entire Italian population under 1 year of age, whereas our study was limited to the high-risk population, further confirming how risk conditions can influence clinical outcomes. Future studies examining healthy populations in parallel with high-risk populations may provide more comparable results. Focusing on hospital admission events occurring in each study cohort, the presence comorbidity, especially BPD (and/or RDS) was associated with a higher severity of RSV hospitalizations and a higher frequency and severity of URA hospitalizations. Overall, none of the RSV and URA hospitalizations detected were fatal.
Although RDS, CHD, BPD and prematurity are known factors that increase the risk of severe hospitalizations following RSV infections [21, 46], few studies have examined different levels of risk among these vulnerable populations. Similar to our findings, BPD condition has been associated with HCRU during RSV hospitalization in terms of higher ICU access rate, mechanical ventilation utilization and longer length of hospitalization than those without BPD [17]. Probably, the higher prevalence of early preterm infants in BPD cohort, compared to the others, in addition to the respiratory problems related to the clinical condition itself, drive this greater HCRU during RSV hospitalizations. In the study of Lapcharoensap and colleagues, it has been shown that infants with very low birth weight and BPD, besides to higher HCRU and longer birth hospitalization stay, were also more frequently hospitalized (for any causes) during first year of life, than those without BPD and required greater HCRU, and related costs increased as gestational age decreased [41]. According to our results, also HCRU associated to RSV hospitalizations of CHD infants was not negligible, suggesting that presence of this clinical condition, in the absence of a prevalent prematurity (given the low number of preterm infants in this cohort), may increase severity of RSV infections. Relevant HCRU associated with RSV hospitalizations among CHD infants has emerged also from previous works [47,48,49].
As regards to palivizumab administration, our results showed that percentages of infants treated in each cohort from 0 to <6 months of age were higher compared to those between 6 and 12 months of age, and this is in line with the well-documented higher impact of RSV infection during the first 6 months of life. However, while most of the CHD and preterm infants received prophylaxis during the first 3 months of life, the majority of BPD-RDS infants received the first dose of prophylaxis between 3 and <6 months of age. This discrepancy is probably due to the longer hospital stay after birth found in this cohort compared to the CHD and Preterm cohorts. Considering the burden of RSV infection over the first 6 months of life, as also confirmed by our analyses, we believe that a timelier distribution of first palivizumab doses during the first months of life, may further improve the benefits produced by prophylaxis. As we aimed to estimate drug consumption, including palivizumab administration, among high-risk infants, we only evaluated total number of infants in each cohort treated with palivizumab during the RSV season, and no specific prophylaxis eligibility criteria for moderate preterm infants without clinical conditions (which can receive palivizumab only if < 6 months old at the start of RSV season) were considered. According to the values obtained, in BPD-RDS cohort palivizumab administration was significantly higher compared to CHD and Preterm cohorts. This finding is in line with the remarkable fragility shown by this cohort in our exploration and with the higher risk of severe RSV hospitalization associated with this diagnosis found in the literature [15, 17]. Palivizumab administration results, stratified by gestational age, showed that early preterm infants of each cohort received more frequently prophylaxis compared to the remaining sub-cohorts and proportions increased with the number of concomitant risk conditions.
However, since we found lower palivizumab administration proportions than expected, we decided to perform an in-depth evaluation of study outcomes (including palivizumab administration, drug consumption and RSV and URA hospitalizations). In particular, in order to have a more defined population that may even more represent the regional health-care management, we repeated same analysis only on infants covered by the regional healthcare system up to 24 months after birth date. While results concerning drug consumption and RSV and URA hospitalizations did not differ from the main results, proportions of palivizumab administration slightly increased by ~ 8.0, 1.0 and 1.5 percentage points in BPD-RDS, CHD and Preterm cohorts respectively, rising to the following values: 56.9%, 8.2% and 12.5%. Similarly, also results stratified by gestational age increased, especially in early preterm sub cohorts where the percentages rose by ~ 10 points increment, reaching these values: 87.2%, 78.9% and 59.3%.
These findings further confirm the greater contribution of concomitant early prematurity and presence of comorbidities, especially BPD (and/or RDS), to the definition of fragility in this population. Defining the vulnerable sub-groups of infants is a crucial aspect for prophylaxis administration strategies and definition of related guidance. In accordance with our finding, a recent study conducted in the USA [36] found that, over a period of 2 years corrected age, 73.1% of extremely preterm infants and children diagnosed with BPD were treated with at least one dose of palivizumab in contrast to 31.9% of those without, these percentages are similar to ours, where 78.7% of early preterm infants with BPD (and/or RDS) and 47.8% of those without received administration of palivizumab. The slightly higher percentages found in our study may be partially related to different gestational age considered, indeed while in the study of Mowitz and colleagues, extreme prematurity indicates WGA <28, in our study early preterm infants have WGA ≤29. In a further study, investigating palivizumab administration in infants and children at high risk of RSV complications, was reported that infants with chronic lung disease, or extreme prematurity (WGA <28) were more likely to be treated with palivizumab [50]. Moreover, in line with our findings, several studies indicated that infants with diagnosis of BPD are more likely to receive palivizumab compared to those with diagnosis of CHD [50,51,52].
In accordance with their higher fragility, BPD-RDS infants were also those more frequently exposed to the following drug categories: adrenergics inhalants, and glucocorticoids for systemic use. Although previous investigations of drug consumption in this population are scarce, the higher drug consumption found in this cohort can be related to the higher presence of extremely preterm infants, as well as the greater respiratory problems related to the diagnosis itself. In a population-based study analyzing drug prescriptions in preterm children (WGA < 37) was reported that these children had higher risk of being prescribed/dispensed with anti-asthmatic drugs (beta-2 agonists and glucocorticoids) compared to full-term children [53]. In addition, a recent study has demonstrated that the use of inhaled bronchodilators and systemic corticosteroids is higher in extremely preterm infants with BPD compared to those without [36], and these findings are in line with our findings, considering the prevalence of early prematurity in BPD-RDS cohort.
Strengths
Our study has several strengths. To the best of our knowledge this is one of the few studies in Italy investigating from an epidemiological point of view the populations at highest risk for severe RSV infections and prevalence of concomitant risk conditions. Our descriptive results suggest that early prematurity is strongly associated with BPD (and/or RDS) condition and that preterm infants with CHD seem to be more frequently associated with BPD (and/or RDS) compared to those born at term. This evidence provides important information concerning the level of fragility of different high-risk populations. In addition, it is one of the few studies that broadly investigates drug consumption in these populations from birth to 24 months. Through the integration of several administrative database, this real word study describes from different point of views a very frail population of infants born in Lazio Region, which represents ~ 10.0% of Italian population with these characteristics.
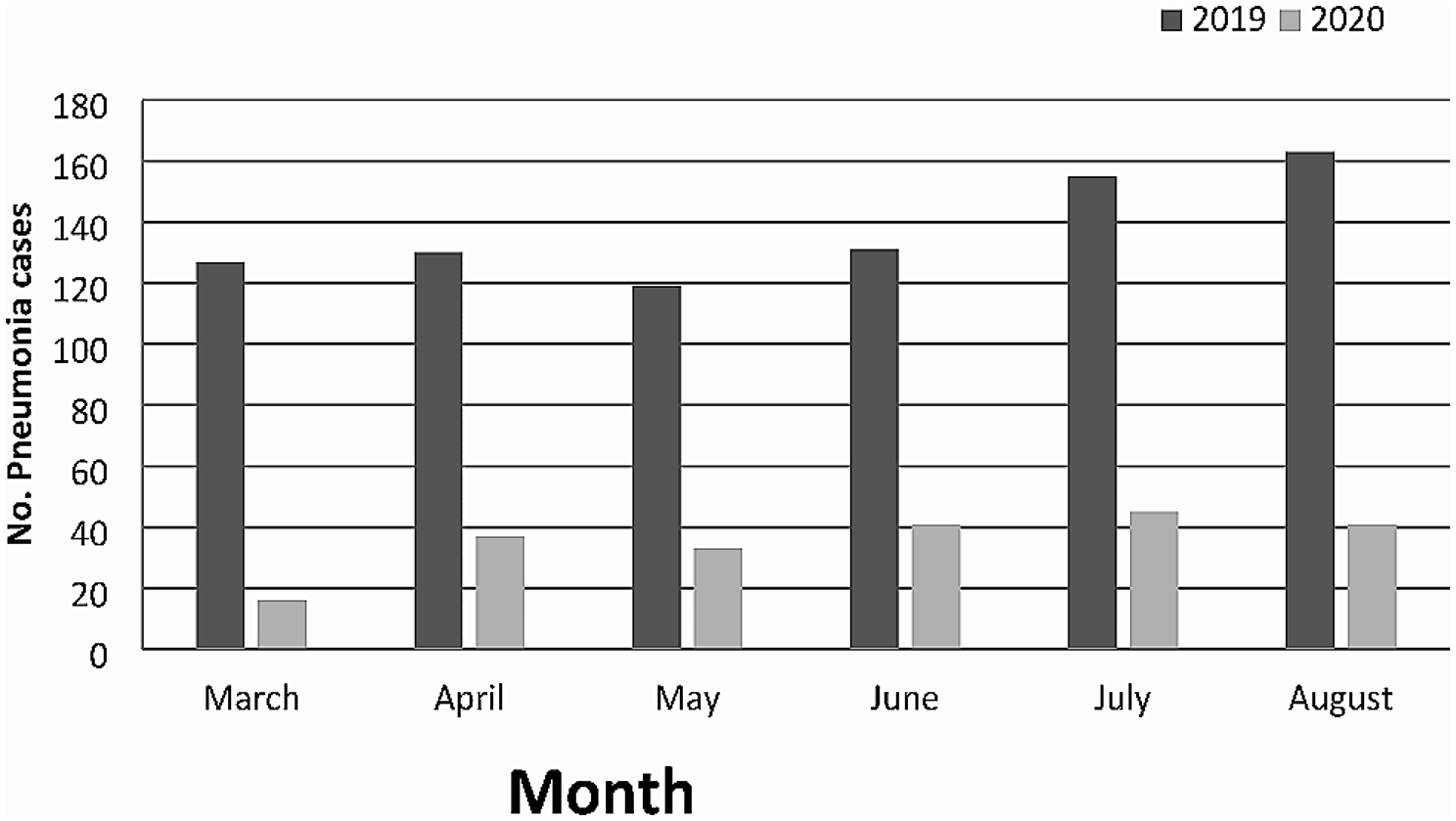
Furthermore, an additional strength of our study is to have highlighted the importance of monitoring the impact of RSV epidemic in a population that, in the future, would be even more affected by the influence of environmental factors related to climate change [54, 55] and concomitant circulation of new viruses, like SARS-CoV-2 [56, 57], on the incidence and severity of RSV and other viral respiratory pathogens. In this context, it is important to mention the consequences of the significant change in RSV seasonality registered during and after the COVID-19 pandemic, which produced first a strong reduction in RSV transmission and a subsequent unexpected increase of RSV-associated hospitalizations starting from late spring 2021 and during the summer and autumn months [58,59,60,61]. In Italy admissions for bronchiolitis sharply increased between September and November 2021, by four folds as compared to pre-pandemic year 2019 [57].
Limitations
Our study presents some limitations that are mostly related to the source of the data. Indeed, our analyses are based on data retrieved from administrative database, where several clinical characteristics and information are not available. For instance, in Italy, where the molecular diagnosis of infectious agents is not routinely done during hospitalization and an RSV surveillance system, similar to the one present in other countries, has not been implemented yet, many cases of hospitalization are probably classified as URA, instead of RSV. As a consequence, in the present study there might be an underestimation of RSV hospitalizations, even if the extraction of both RSV and URA hospitalizations gave us the possibility to distinguish RSV from other respiratory tract infections. In addition, the analysis is based on data from one single Italian Region and results obtained may not reflect trends about similar outcomes of other geographical area. However, Lazio is one of the most populated regions in Italy with around 40,000 newborns per year. Furthermore, the use of ICD-9 codes to identify diagnosis from hospital discharge records, may has approximated actual diagnoses and may has not captured all relevant medical diagnoses, especially for BPD. Being this a study that adopts administrative data from secondary care (excluding drug prescriptions which were analyzed from both primary as well as secondary setting), a limitation of the analysis is the lack of data which are not recorded in such data sources, in particular outpatient data regarding medical visits for respiratory infections. Lastly, possible resolution of CHD (especially the presence of patent ductus arteriosus in CHD cohort) or BPD (and/or RDS) comorbidities after birth were not detectable and as a consequence, this aspect may have overestimated the persistence of comorbidities after birth in the cohorts





留言 (0)