
記住我

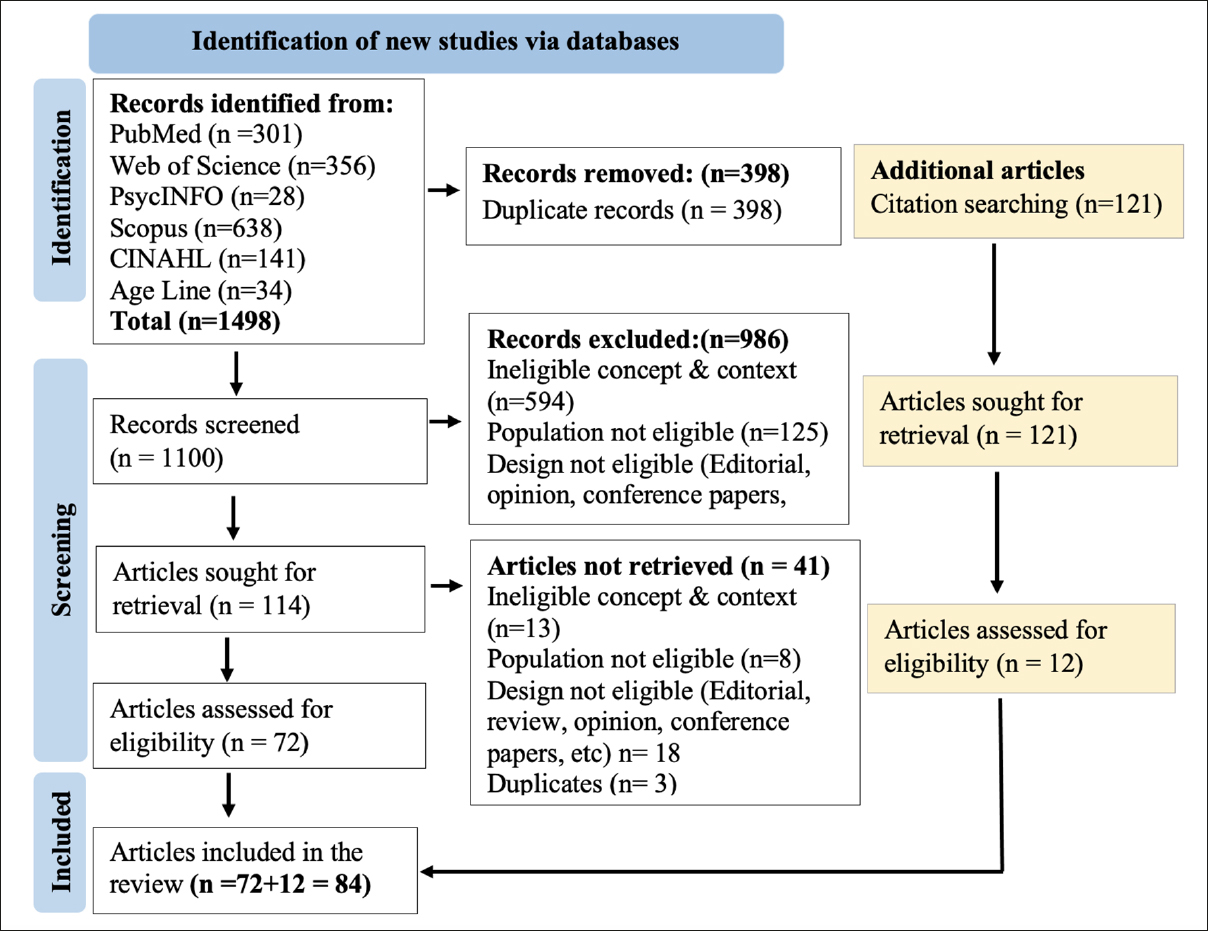
Seven databases were searched yielding a total of 51,001 papers, of these, 138 articles reporting unique interventions were included. Study references are provided in the supplementary material. Searches for associated texts to assess exercise types (e.g. reports of protocols, pilots and development work) resulted in a total of 259 articles.
Study characteristicsGeneral characteristicsCharacteristics of included studies are provided in Supplementary Tables 2 to 5. Studies were conducted from the period 1988 to 2020 and were predominantly undertaken in Europe and North America (75.3%). Almost half (44%) had another report associated with the study. Only 12 (8%) described themselves as multi-component and only four specifically stated they were targeting multi-morbidity. Most used randomised controlled designs (75.4%).
Participant characteristicsAcross studies, 22,610 participants with a mean age of 72.1 years (range 60–92) were enrolled. Studies largely did not report mean number of comorbidities; combining statistics from those that did (n=36, 26%) gives a mean of 3.4 comorbidities (range: 2–6.6). Twelve reports described assessing multi-morbidity via validated measures. Most frequently used (n=9) was the Charlson Comorbidity Index (CCI);(30) however the actual score was only reported in seven studies (mean CCI: 3.39).
The majority of studies targeted either one, two or three chronic diseases (n=79, 57.2%; n=8, 5.8%; n=2, 1.4% respectively). Activity (n=20, 14.5%), risk factors (n=19, 13.8%), social care settings (n=7, 5.1%) or body composition (n=3, 2.2%) were other target criteria. By chronic disease, the most frequently represented were cardiovascular (n=24, 17.4%), followed by respiratory (n=14, 10.1%), cerebrovascular (n=11, 8%) and metabolic conditions (n=9, 6.5%). Physical function disorders were relatively regularly targeted (n=12, 8.7%) as were geriatric conditions (n=10, 7.2%) and frailty (n=10, 7,2%.) Only a limited number of comorbid conditions were counted by most studies and it is likely the burden of disease was significantly higher.
Exercise intervention characteristicsOverall, 22 different multi-component combinations were identified, see Figure 2. Few studies featured respiratory training (n=7, 5%). Seventy-three percent of studies were delivered twice per week and studies favoured a delivery duration of 60 minutes (n=51, 36%) for 12 weeks (n=24, 17%). Across programmes, the total exercise delivery time ranged from 4 to 430 hours with the average amount of exercise time prescribed being 180 minutes/week. Fifty-seven studies (41%) delivered interventions that did not meet recommended thresholds of 150 minutes a week (14).
Figure 1 Figure 2
Figure 2
Diversity of exercise combinations in multi-component exercise interventions
Most interventions were centre based (n=78, 57%), followed by a combination of home and centre (n=29, 21%), exclusively home based (n=24, 17%) or delivered in a care home (n=7, 5%). Physiotherapists were the deliverer of choice across studies (n=66, 48%), followed by the multi-disciplinary team (MDT) (n=25, 18%) then exercise therapists (n=23, 17%). A group approach was favoured (n=106, 77%). Whilst this may indirectly provide socialisation benefits (31), few studies specifically described socialisation activities as part of the intervention (n=7, 5%). Group based studies generally require transportation, however only 11 studies gave details of transportation support; in most cases transportation arrangements were not clear (n=86); 11 studies were judged to have not provided transportation support.
Descriptions of the formula for exercise intensity could be extracted from 92 of 138 studies (67%) (Figure 3). The most commonly used method to inform exercise intensity was the Borg rating of perceived exertion scale (RPE), followed by cardiopulmonary exercise testing and maximal heart rate (MHR). Based on studies reporting intensity by RPE or MHR, moderate intensity exercise was most commonly prescribed. Ninety-seven studies (70.2%) stipulated that the prescribed exercises were titrated, for the remaining programs (n=41, 29.7%) it was unclear whether exercise prescriptions were modified across the duration of the intervention.
Figure 3
Exercise intensity overview
Choice of exercise type (Figure 4), frequency, intensity and duration were most frequently judged to be based on practitioner intuition/local practice (n=64, 46%). Of those citing a published study (n=38, 28%), twelve (35%) were based on four established programmes (Otago, Enhance Fitness, Sunbeam, High-Intensity Functional Exercise [HIFE]). For guideline-based studies (n=29, 21%), the most commonly referenced were recommendations from the American College of Sports Medicine that were contemporary to the research. Very few of the exercise programs were described as being based on developmental work (n=7, 5%); as is recommended for complex interventions (32, 33); like the programs described here.
Figure 4
Assessment of rationale behind inclusion of exercise types
Two-component studiesStudies largely favoured a 2-component exercise intervention (n=62, 45%) with the traditional combination of aerobic and resistance exercises being most common (n=49, 80.3%). Forty-four percent of 2-component studies included a non-exercise element, chiefly education (24.6%) or nutrition (8.2%). Most were centre based (n=37, 60.7%) or a combination of centre and home (n=13, 21%) and delivered by physiotherapists or exercise therapists (52.4%). Mean frequency was 3 times/week, giving an average exercise time of 152 minutes/week, for a duration of 138 days (range: 21–1095).
Three-component studiesThe volume of studies reduced with each additional exercise type added. Forty-one studies (30%) included 3-component exercise interventions. The most common combination of exercise types was aerobic, resistance and balance (n=15, 36.6%.) A greater proportion (n=20, 49%) of 3-component studies were accompanied by non-exercise elements, principally education (61.9%), followed by behaviour change (14.3%) and psychological interventions (14.3%). Centre-based interventions were marginally more frequent (n=21, 51%) over a combined centre and home setting (48%). Physiotherapists were the intervention deliverer of choice (n=30, 73.1%), for a mean duration of 168 days (range 21–730). Average frequency was three times/week, giving a mean exercise time of 180 minutes/week.
Four-component studiesThirty-one studies (22%) included a 4-component exercise intervention, these were dominated by aerobic, resistance, balance and flexibility combinations (n=19, 59.3%). Forty-five percent of 4-component interventions were accompanied by non-exercise elements (n=14), these were most often medical optimisation (23.8%) followed by education and nutrition (both n=4, 19%). The mean duration of intervention was 265 days (range: 28–1277 days) and physiotherapists were again the main deliverer (n=15, 46.8%), followed by education therapists (n=8, 25%) or the multi-disciplinary team (n=6, 18.7%). Exercises were prescribed on average three days per week for an average exercise time of 156 minutes/week.
Five-component studiesAll 5-component studies (n=4, 3%) included the same combination of exercises: aerobic, resistance, balance, flexibility and functional. Only one of these was accompanied by a non-exercise component (medical optimisation). Mean duration was 130 days (range: 121–182 days) and three out of four interventions (75%) were delivered by the MDT. Mean frequency was seven times/week for an average of 275 minutes/week.
留言 (0)