Recently, DSCT was applied for the staging of gastric cancer [26], and a complete blood count is a basic routine examination. Using data from DSCT and complete blood count is practical and noninvasive, although histological analysis by biopsy of the gastric lesion before any treatment is indispensable for clinical management [27]. It is reported that among gastric carcinoma types, SRC shows less aggressive biologic characteristics, and mixed-SRC shows more aggressive characteristics, which must be considered for planning therapies [3]. Thus, DSCT combined with NLR as a noninvasive method could be used to differentiate SRC in early gastric cancer, which may be helpful in deciding on a specific cancer treatment. The findings might provide evidence for the application of DSCT in the noninvasive differential diagnosis of gastric adenocarcinoma subtypes.
In this study, ICVP and NICVP, as indicators of angiogenesis and MVD [14], were significantly higher in the SRC group than in the mSRC and nSRC groups, but there were no significant differences in ICVP and NICVP between the mSRC and nSRC groups. The reason may be that SRC has abundant neovascularization and high permeability, while mSRC has low MVD [28]. The results also showed that the kVP of the SRC group was significantly higher than in the mSRC and nSRC groups, which may be related to the relatively rich blood supply of SRC tumors [29], leading to higher iodine contrast agent after enhancement and higher CT values when at lower keV.
The possibility of using the NLR to differentiate between benign and malignant conditions has been shown for gallbladder [18, 30] and adrenal lesions [19]. On the other hand, studies of the NLR in gastric cancer are rarer. A study showed that the inflammatory response and preoperative NLR were prognostic markers in patients with gastric adenocarcinoma [31]. Two other studies showed that the NLR was associated with prognosis [23] and lymph node positivity [24] in patients with gastric SRC. Regarding the diagnostic value of NLR for SRC, a recent study revealed that the NLR could differentiate between differentiated (not including SRC) vs. undifferentiated (including SRC) gastric cancers [22]. The present study appears to be the first to directly compare the NLR among SRC, mSRC, and nSRC, showing that the NLR was significantly different among the three subtypes. The normal NLR values in adult, non-geriatric individuals in good health are between 0.70 and 0.78 and 3.00-3.53 [16, 17], but variations in NLR can be observed among patients, even if they are within the normal range. Of note, the optimal cut-off value determined in the ROC analysis was 2.33 in the present study.
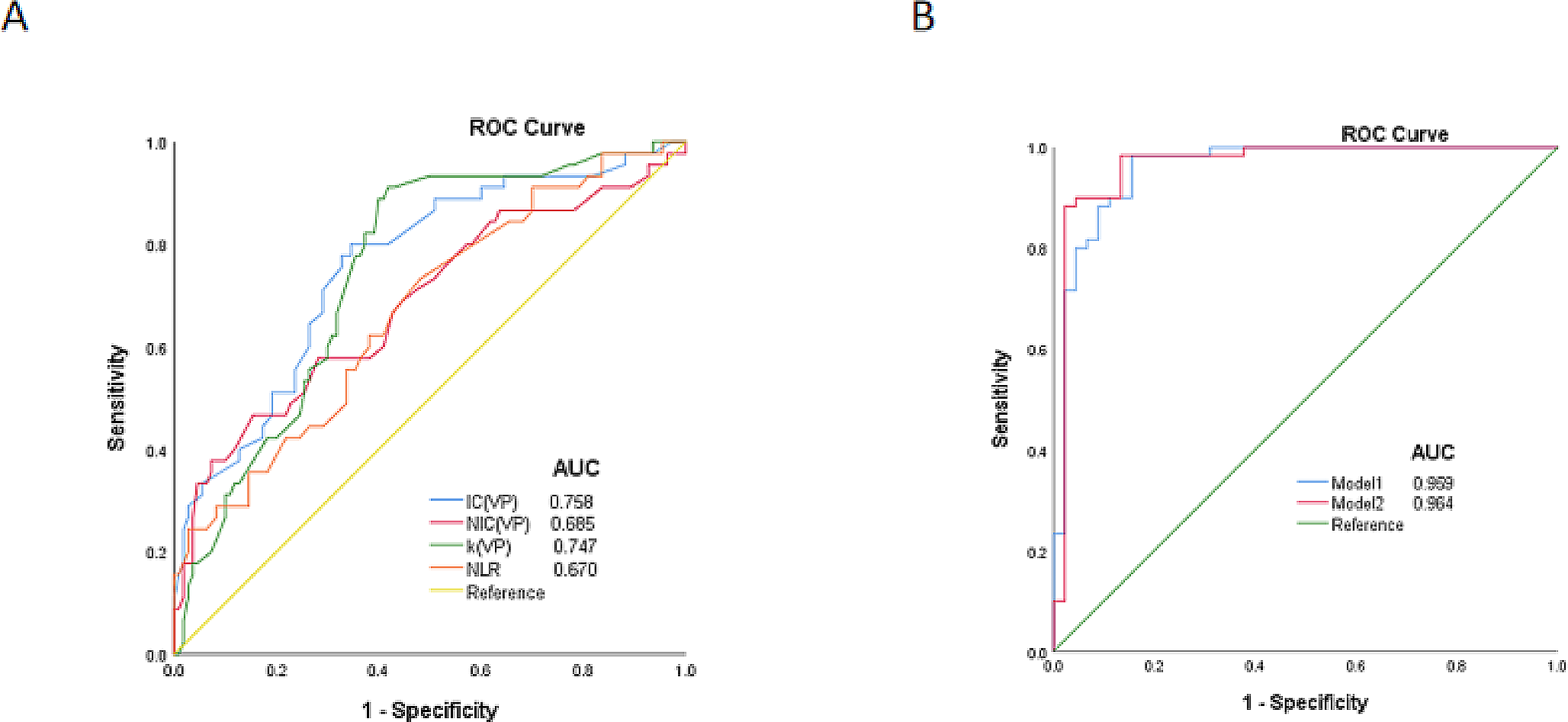
In the present study, the AUCs of the individual DSCT parameters and NLR were 0.670–0.758. The AUC values of the individual parameters were lower than that of CT-based radiomics nomograms for identifying SRC (Lauren nomogram, AUC = 0.841–0.895; SRCC nomogram, AUC = 0.845–0.918) [32], suggesting that the single indexes had a relatively poor diagnostic performance. On the other hand, the AUC of the combination of all four parameters was 0.964 for differentiating SRC from mSRC and nSRC. That combination had a higher AUC than in the radiomics study by Chen et al. [32]. Hence, the results support the use of that model for differentiating SRC from mSRC and nSRC, but external validity will have to be examined.
There were several limitations in this study. First, this study was conducted in a single center, limiting the sample size. The small size limits the reliability of the evaluation, and the single center limits the generalizability of the results. Second, this study was retrospective, which may cause data bias, limiting the analyzable data to those available in the patient charts and preventing the determination of any cause-to-effect relationships [33]. Third, multivariable analyses can be clinically invalid since they are based on the included variables, which depend upon the available variables. Hence, different studies that collected different variables can reach different conclusions. Fourth, the blood tests for NLR were generally performed 5 days before surgery, but it was a retrospective study, and it is possible that the timing might be different for some patients. The next step would be to increase the sample size and conduct prospective studies to continue exploring the diagnostic value of DSCT combined with the NLR for distinguishing SRC from mSRC and nSRC. In addition, T2WI imaging can help determine the mucus component in cancers [34, 35], but the present study only included DSCT data, not MRI. Nevertheless, future studies could investigate a combination of FSCT and MRI parameters for distinguishing SRC, mSRC, and nSRC.
In conclusion, DSCT combined with NLR showed high diagnostic efficacy to differentiate SRC from mSRC and nSRC. However, the result still requires prospective studies to be confirmed in the future. Nevertheless, the model could eventually be used to help guide patient management.



留言 (0)