
記住我


Several ovarian pathologies can also manifest with hirsutism, including both benign and malignant entities. These entities may be discovered incidentally or during imaging work-up for hirsutism and virilization. Ovarian lesions are often seen on ultrasound; however, indeterminate lesions can be further evaluated on CT, MRI, and/or positron emission tomography (PET) [14].
Polycystic ovary syndrome (PCOS)Polycystic ovary syndrome (PCOS) is the most common cause for hyperandrogenism in premenopausal women [15, 16]. It is characterized by hyperandrogenism, ovarian abnormalities, and numerous ovarian cysts. The exact etiology of PCOS remains unknown, although posited hypotheses include increased frequency of gonadotropin-release hormone pulses stimulating androgen production by theca cells. PCOS is also associated with insulin resistance, leading to an increased risk of type 2 diabetes mellitus and cardiovascular disease [15,16,17].
One of the criteria used for diagnosing PCOS is the presence of multiple ovarian cysts, with either 12 or more cysts in one ovary or ovarian volume greater than 10 mL. Follicles are often peripherally oriented in the ovary, classically described as a “string of pearls” appearance (Figs. 5, 6) [16, 17]. However, imaging findings are not necessary for the diagnosis of PCOS if other clinical criteria are met, including biochemical evidence of hyperandrogenism and evidence of ovulation abnormality [16, 17].
Fig. 5
A 28-year-old woman with no significant past medical history presented with irregular menstrual periods. She underwent pelvic ultrasound which demonstrated mildly enlarged ovaries with numerous peripherally oriented small follicles (arrowheads). The right ovary measured 22 mL in volume, while the left ovary measured 16 mL (not shown)
Fig. 6
T2-weighted coronal MRI of the pelvis of a 29-year-old woman who presented with hirsutism and right ovarian cyst on ultrasound. Enlargement of both ovaries, which contain numerous peripheral small follicles in a “string of pearls” distribution, is seen (arrows). This appearance is compatible with PCOS
Ovarian hyperthecosisOvarian hyperthecosis is characterized by the presence of islands of luteinized theca cells in the ovarian stroma. These luteinized theca cell nests are scattered throughout the ovarian stroma in ovarian hyperthecosis. This is in contrast with PCOS, where they are located primarily in areas around the cystic follicles [18]. The clinical presentation of ovarian hyperthecosis is similar to PCOS, including menstrual dysfunction (which includes postmenopausal bleeding), obesity, insulin resistance, and hyperandrogenism. However, women with hyperthecosis tend to have higher testosterone levels, more hirsutism, and a higher incidence of virilization compared to those with PCOS. Ovarian hyperthecosis most commonly occurs in perimenopausal or postmenopausal women and is the second most common cause of hyperandrogenism in postmenopausal women [18, 19].
Ultrasound findings of ovarian hyperthecosis are nonspecific and may show an increase in ovarian size, often involving both ovaries. There are typically no focal areas of increased vascularity on color Doppler. The increased ovarian stroma in hyperthecosis tends to gently push normal-appearing follicles towards the periphery, in contrast with PCOS, which tends to present with numerous small follicles with thickened walls in a setting of relatively normal ovarian stroma [20]. However, failure to detect an ovarian lesion on pelvic ultrasound does not exclude hyperthecosis. MRI may be helpful for further evaluation in patients with possible ovarian hyperthecosis, although its role in diagnosing this entity is not fully established. The described MRI appearance of ovarian hyperthecosis have included symmetric bilateral ovarian enlargement with homogeneous T2 hypointensity of the ovaries, as well as mild enhancement (Fig. 7). Rarely, this entity can manifest as bilateral ovarian masses which are isointense to uterine myometrium on T1- and T2-weighted images [19, 21].
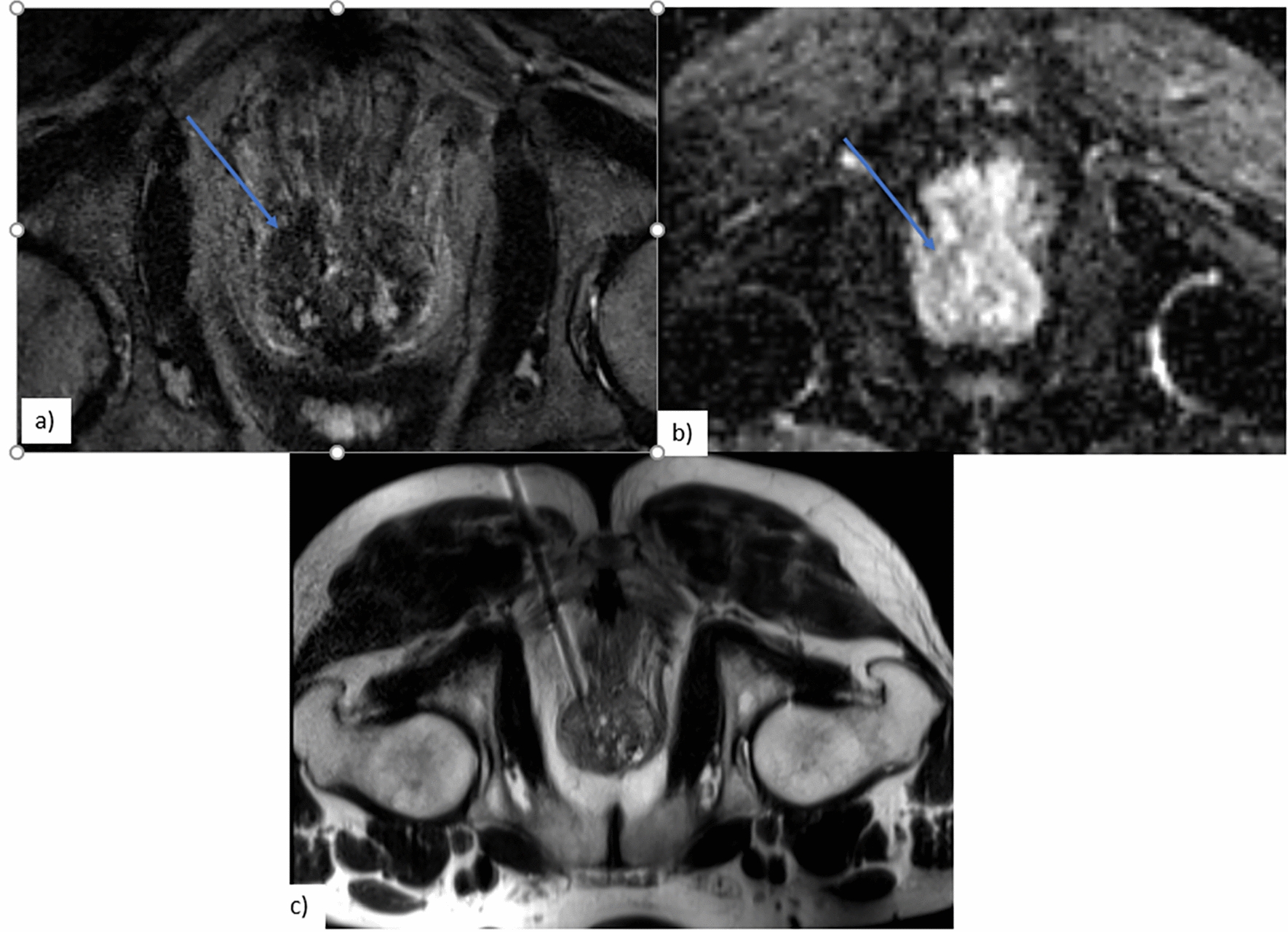
Fig. 7
A 69-year-old woman with a history of hypertension, diabetes mellitus, and hepatitis C, who presented with 2 years of hirsutism, with laboratory results demonstrating elevated total testosterone levels and low DHEAS level. MRI abdomen demonstrated stable mild thickening of the left adrenal gland and normal right adrenal gland. Subsequent pelvic MRI was significant for enlargement of both ovaries (arrows) with low to intermediate signal on T1-weighted sequences (image a). On T2-weighted images, the ovaries demonstrated relatively decreased signal intensity (image b). Contrast-enhanced images (image c) demonstrated mild enhancement of the ovaries. The decision was made for the patient to undergo bilateral salpingo-oophorectomy. Final pathology was consistent with ovarian stromal hyperplasia and stromal hyperthecosis
Treatment of ovarian hyperthecosis includes medical management such as gonadal suppression and surgical management (oophorectomy or ovarian wedge resection) [18].
FibrothecomaFibrothecomas, fibromas, and thecomas are benign solid ovarian sex-cord stromal tumors. They are relatively uncommon, making up around 4% of all ovarian tumors [22]. While fibromas consist of benign fibroblast and collagen bundles arranged in whorls, thecomas are made of theca cells containing cytoplasmic lipid with varying degrees of fibrosis. The term ‘fibrothecoma’ reflects the frequently noted histologic overlap of these lesions. Fibrothecomas can occasionally be hormonally active. Meigs syndrome is a clinical triad consisting of fibroma, ascites, and pleural effusion, which resolves after resection of the fibroma. Fibromas and fibrothecomas can also present in association with basal cell nevus (Gorlin-Goltz) syndrome, which consists of large multinodular ovarian fibromas, multiple basal cell carcinomas of the skin, odontogenic keratocysts, and other findings [15, 23, 24].
Ultrasound findings of ovarian fibrothecoma are often nonspecific, typically a hypoechoic solid ovarian mass (Fig. 8), although hyperechoic masses have also been reported [25]. On CT imaging, most fibrothecomas present as solid adnexal masses with variable enhancement, although many demonstrate delayed homogeneous enhancement [24, 25]. On MRI, the solid portions of the tumor typically demonstrate homogeneous low signal compared to myometrium on T1- and T2-weighted images, with mild enhancement on contrast-enhanced images (Fig. 9). Associated edema and cystic degeneration are commonly seen, especially in large fibrothecomas [23, 25]. Calcifications and hemorrhage are rare. The majority of these lesions are unilateral and can rarely be malignant [23,24,25].
Fig. 8
A 21-year-old woman with no significant past medical history, who presented with menstrual irregularity and pelvic pain. Pelvic ultrasound demonstrated a solid left ovarian mass (image a) with internal vascular flow (image b), most consistent with a solid ovarian lesion such as fibrothecoma
Fig. 9
Pelvic MRI in the same patient shows a solid left ovarian lesion with low to intermediate T2 signal intensity (arrow), as well as mild uniform enhancement, consistent with fibrous tumor such as fibrothecoma. The patient underwent left salpingo-oophorectomy, with final pathology consistent with ovarian fibrothecoma
Although functional ovarian fibrothecoma are rare, there have been several reported cases of ovarian thecomas causing hirsutism, menstrual irregularity and/or amenorrhea. The mainstay treatment of hyperandrogenic ovarian thecomas is complete surgical excision [26].
Leydig cell tumorLeydig cell tumors are rare ovarian sex-cord stromal tumors, accounting for less than 0.1% of all ovarian tumors [25]. They primarily occur in postmenopausal women and are typically benign and unilateral. These tumors are functional and typically produce testosterone, leading to hyperandrogenism and virilization. Histological characteristics include nodules of Leydig cells with neoplastic stromal proliferation. Approximately half of patients develop signs of virilization, while another third present with estrogenic manifestations, which can be secondary to direct estrogen secretion from the tumor, peripheral conversion of androgen to estrogen, associated ovarian stromal hyperthecosis, or a combination of factors [27]. The mainstay treatment is surgical resection, especially given the difficulty in distinguishing benign versus malignant variants of this tumor based on clinical presentation and imaging alone. In some patients who may not be good surgical candidates, medical hormone treatment (e.g., gonadotropin releasing hormone agonists) may be a viable management option [25, 27].
On ultrasound, Leydig cell tumors are typically unilateral and tend to be isoechoic to myometrium (Fig. 10) [25]. On CT, these tumors tend to present as a hypodense solid ovarian mass (Fig. 11) [25]. MRI characteristics of Leydig cell tumors include variable T2-weighted signal depending on the amount of fibrous content (Fig. 12) [25]. Given their small size, they can be difficult to differentiate from normal ovarian tissue. Diffusion weighted sequences can be helpful in these cases, as the tumor tends to demonstrate slightly higher signal intensity on these sequences compared to normal ovary [25]. These tumors demonstrate gradually increasing and delayed enhancement [25].
Fig. 10
A 57-year-old woman underwent pelvic ultrasound exam showing a solid left ovarian mass with internal vascularity on Doppler ultrasound exam
Fig. 11
The patient subsequently underwent contrast-enhanced CT examination, which demonstrated a corresponding heterogeneously enhancing left ovarian lesion (arrow). Final pathology confirmed Leydig cell tumor
Fig. 12
A 68-year-old woman with a past medical history of hypertension and uterine fibroids presented with a 3-year history of hirsutism, with increased hair on shoulders. Laboratory results showed elevated testosterone, suppressed luteinizing hormone (LH) and follicle-stimulating hormone (FSH), and low DHEAS levels. Pelvic MRI showed a right ovarian lesion (arrow) with low to intermediate T1 signal intensity (image a), low T2 signal intensity (image b), and heterogeneous enhancement (image c). On surgical resection, a 2.5 cm right ovarian mass was noted, with final pathology consistent with benign Sertoli–Leydig cell tumor. On follow up visits, the patient reported improving hirsutism and had decreasing testosterone levels
Other sex-cord stromal tumors, such as granulosa cell tumors and steroid cell tumors, have also been reported in association with virilization and hirsutism, although these cases are extremely rare [28, 29].
Androgen-secreting mature cystic teratomaMature cystic teratomas, also commonly referred to as dermoids, represent approximately 10–20% of ovarian neoplasms and are commonly seen in reproductive age women [30]. They consist of well-differentiated ectodermal, endodermal, and mesodermal germ cell layers. While most ovarian teratomas are nonfunctional and usually discovered incidentally, rarely teratomas can secrete androgens, leading to virilization and hirsutism. Cases of single or multiple ovarian teratomas in association with polycystic ovaries have been reported [31]. Polycystic ovaries can be seen secondary to high circulating androgens. However, there have also been cases of hirsutism associated with ovarian teratomas without the presence of polycystic ovaries. In some of these lesions, histologic evaluation demonstrated luteinized cells within the stroma of the tumor, which may have been the cause for hyperandrogenism [15, 30, 31].
Several ultrasound features of ovarian mature cystic teratomas have been described. A classic appearance is that of a cystic adnexal lesion (Fig. 13) with a densely hyperechoic nodule, known as a Rokitansky nodule, projecting into the lumen of the cyst. Other described ultrasound appearances include a homogeneously hyperechoic lesion, fat-fluid levels, dermoid mesh (linear echogenic bands floating within the cyst, representing hair fibers), and the ‘tip of the iceberg sign’ which describes an echogenic mass containing hair causing posterior acoustic shadowing [32,33,34]. CT findings of ovarian teratomas also typically include a unilocular cyst with a solid Rokitansky nodule which contains fat and hair (Fig. 14). Calcification of the cyst wall may be present or absent [33, 34]. On MRI, the macroscopic fat-containing portion of the dermoid follows the expected signal intensity of fat on all sequences [33, 34].
Fig. 13
A 15-year-old female with a past medical history of epilepsy presented with hirsutism and elevated testosterone levels. Pelvic ultrasound demonstrated a large cystic structure in the right adnexum containing internal low-level echoes
Fig. 14
Contrast-enhanced CT of the pelvis in the same patient as Fig. 13, which demonstrates a large fluid-filled cystic structure (arrow) with adjacent solid nodule (arrowhead) containing punctate calcification. Macroscopic fat (*) is present anteriorly in the mass. Final pathology was consistent with mature teratoma. The patient’s testosterone levels normalized after surgery
留言 (0)