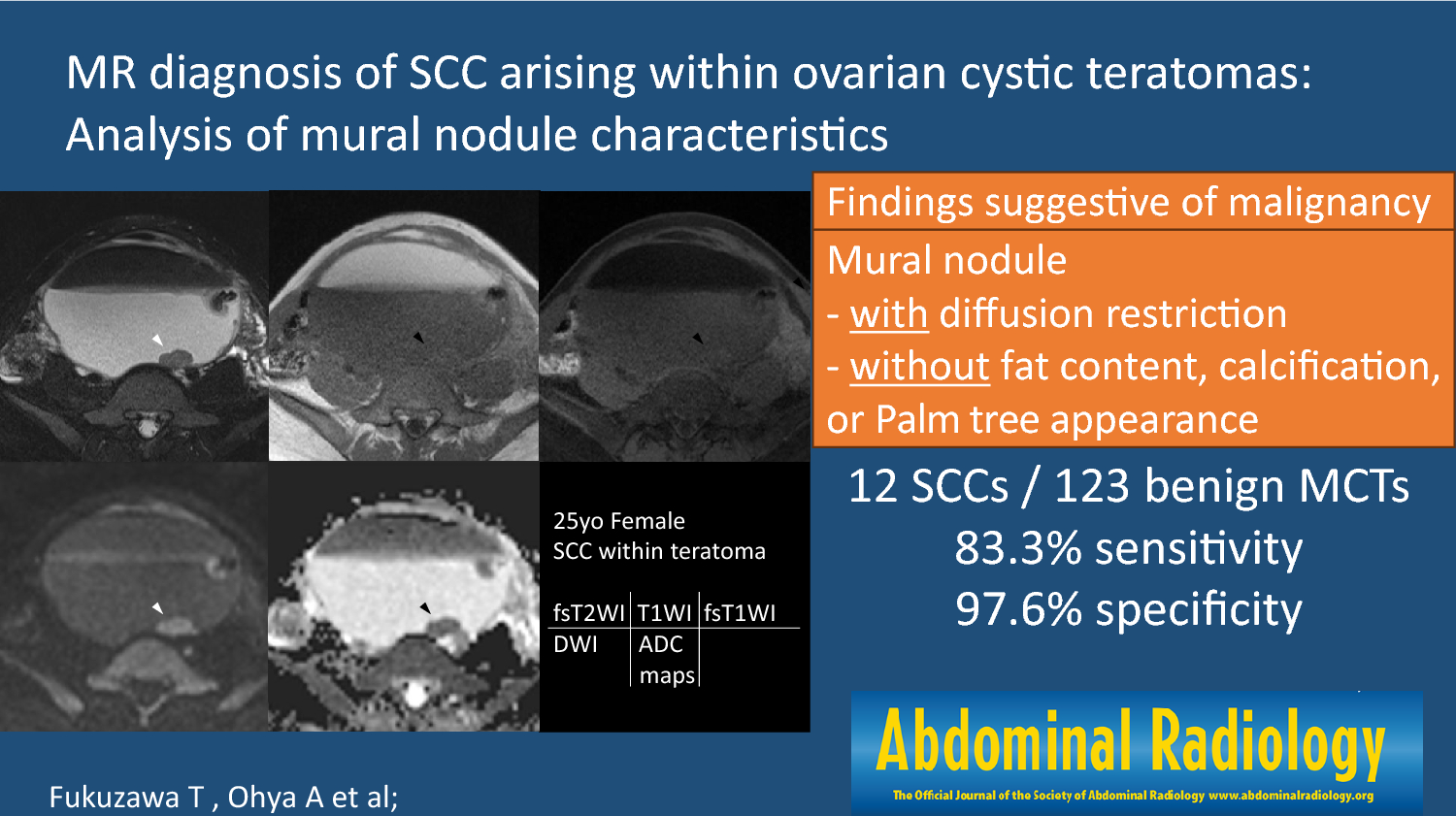
While SCC-MCT pathologically presents as a nodule inside the cystic tumor or a plaque on the cyst wall [2, 7], no study has focused on the MR characteristics of mural nodules within SCC-MCTs. Herein, we explored characteristic MR findings of mural nodules in SCC-MCTs, comparing their diagnostic performance with that of the PRFs. Particularly, we focused on the solid components observed within MCTs and found that findings such as presence of diffusion restriction, absence of fat content, absence of Palm tree appearance, and absence of calcification were significantly more frequent in the SCC-MCT group. Furthermore, the four findings suggestive of malignancy were characterized by an excellent inter-reader agreement among radiologists, and they demonstrated higher diagnostic ability compared to the PRFs.
Projections called Rokitansky protuberances are often found in benign MCTs [8, 10]. Previously reported histological analysis of Rokitansky protuberances revealed the presence of sebaceous glands, adipose lobules, keratin, pilosebaceous adnexa, glial tissue, thyroid tissue, fibrous stroma, or vessels [15, 16]. Bone and teeth also tend to be observed in this protuberance and most of the hair arises from this nodule [3, 8, 13]. As a result, mural nodules within b-MCT often have calcifications and a Palm tree appearance. Rha et al. reported that a small fat component in the cystic wall of MCT can be detected using fat-saturated MR imaging or gradient-echo technique with both in-phase and opposed-phase imaging, which is useful to identify small amounts of fatty tissue on MR images [11]. Thus, the absence of these characteristic findings commonly observed in Rokitansky nodules is a distinctive feature of the mural nodules in SCC-MCT. However, as reported by Fujii et al., diffusion restriction in the mural nodules inside MCT, which often present as abnormal signal intensity on DWI in the diverse tissues of Rokitansky protuberances, does not alone indicate malignancy [17]. Moreover, squamous cell carcinomas typically exhibit diffusion restriction due to their high cellular density [18, 19]. Therefore, our study showed that diffusion restriction in the mural nodules alone does not rule out SCC-MCT; however, the absence of characteristic MR findings in the Rokitansky nodule (i.e., fat, calcification, and Palm tree appearance) combined with the occurrence of diffusion restriction in the mural nodule can lead to a diagnosis of SCC-MCT.
Several other useful findings to differentiate benign MCTs from malignant MCTs have been previously reported. The peak incidence of the MCT is reported to be between 20 and 40 years, while the mean age of malignant transformation is 45–60 years [3, 12]. The size of a malignant ovarian MCT is usually larger than that of a benign MCT [1,2,3, 5, 12, 20]. On MR images, SCC-MCT is characterized by transmural extension and infiltration into surrounding organs from solid components [7, 20, 21]. Furthermore, the analysis of CT and MR findings in 11 patients with this malignancy revealed that nine (82%) tumors had soft tissue components and eight (89%) had an obtuse angle between the soft tissue components and the inner wall of the cyst [2, 6]. Per findings of previous reports and the present study, the SCC-MCT group had significantly higher age, larger lesions, and greater mural nodule sizes compared to the b-MCT group. Additionally, mural nodules, obtuse angle between the nodule and the cyst wall, and transmural extension were observed significantly more frequently in the SCC-MCT group. These PRFs are considered important for differentiation between the two groups. However, if the mass is accompanied by transmural invasion, it is deemed to be already in the advanced stage of malignant transformation. Thus, imaging findings to detect SCC-MCT in its early stage are required. Additionally, there is a wide overlap in values of MR findings, such as tumor size, presence of mural nodules, and size of mural nodules, between benign MCT and SCC-MCT, making it difficult to establish clinically useful cut-off values [15, 16]. In the SCC-MCT group in our study, three cases did not exhibit transmural invasion, but conformed to the findings suggestive of malignancy (Figs. 5, 6, 7; Table 1). Additionally, two cases did not exhibit the PRFs for SCC-MCT, i.e., obtuse angle between the nodule and cyst wall. These three cases suggest the possibility that early-stage SCC-MCT can be diagnosed using findings suggestive of malignancy. In the Ovarian-Adnexal Reporting & Data System (O-RADS), a large volume of contrast-enhancing solid components in a lesion with lipid content presents an intermediate risk of malignancy [22]. However, it should be noted that even small mural nodules without transmural invasion may be indicative of malignancy. Therefore, diagnosis of SCC-MCT using findings suggestive of malignancy is crucial, regardless of patients’ age, tumor size, size of mural nodules, obtuse angle between the nodule and the cyst wall, or transmural invasion.
There were several limitations to our study. First, various MR imaging units and different protocols were included because this was a retrospective, long-term, and multicenter study. Second, while most institutions retain paraffin-embedded tissue blocks (PFFEs) for long durations, our retrospective study design presented specific challenges in correlating the mural nodules seen on MR images with their respective locations on pathology slides. This difficulty arises in retrospective analyses, where it is often not feasible to precisely match MR images with the exact sections in stored PFFEs. Consequently, we were unable to explore the correlations between the pathological findings and the radiographic findings suggestive of malignancy in the mural nodules. Third, there was a large difference in the number of cases between the benign and malignant groups, and it is necessary to take into account that there was a class imbalance bias in this study. However, it was unavoidable because SCC-MCTs are rare conditions. Finally, we did not investigate the malignant transformation of MCT that exhibit histological types other than SCC. This is because the number of cases with other histological types was extremely limited in the participating institutions. Therefore, it is unclear whether findings suggestive of malignancy can be applied to the malignant transformation to pathologies other than SCC.
In conclusion, characteristic MR findings of SCC-MCTs were as follows: mural nodules exhibited diffusion restriction, but, did not demonstrate fat content, Palm tree appearance, or calcification. These four findings suggestive of malignancy demonstrated higher diagnostic ability compared to the PRFs of age, tumor size, size of mural nodule, and the angle between mural nodule and cyst wall. Therefore, to provide accurate preoperative diagnosis of SCC-MCTs, cases with smaller mural nodules should be examined for the aforementioned four findings suggestive of malignancy.



留言 (0)