
記住我






The RCT is being implemented in a community-based federally qualified health center (FQHC) located in the southern part of San Diego County, CA, along the US-Mexico border. This FQHC offers HIV primary and sub-specialty medical services and coordinated case management services at multiple locations to a majority racial minority population, which will help achieve the study goal of reaching Hispanic and Black PLWH.
Eligibility criteriaIndividuals are eligible to participate in PATH if they meet the following criteria: (a) are at least 18 years old; (b) can read and speak English or Spanish; (c) are living with HIV and at least 3 months have passed since HIV diagnosis; (d) currently prescribed antiretroviral therapy (ART) medication; (e) have regular access to an Internet browser on a computer, tablet, or smartphone; (f) do not plan to move out of the San Diego area in the next 12 months; (g) not currently enrolled in any other program, intervention, or research study designed to improve HIV adherence or engagement in HIV care; and (h) not currently a member of one of the community advisory boards providing advisement on the study. In addition to criteria a through g, eligible participants must meet one or more of the following criteria: (1) one or more detectable VL test result (> 200 copies m/L) in the past 12 months while on ART for at least 3 months; (2) missed 1 or more scheduled HIV care appointments in the last 12 months; (3) last HIV care visit with an HIV care provider was more than 6 months ago; (4) report anything less than excellent adherence on one of the Wilson-3 ART adherence scale [28] items; and/or (5) report non-prescription stimulant or opioid use in the past 6 months. The first three indicators are verified using medical chart information, and the last two are assessed via self-report on the screening questionnaire. Finally, since the intervention was designed in a manner whereby the PATH peer navigators are meant to provide support as part of the HIV care team at the community-based FQHC, and as a study that is interested in exploring implementation outcomes of the PATH intervention, eligible participants are required to be current HIV medical care patients of the community-based FQHC.
Who will take informed consent?Written informed consent is gathered from participants. During the enrollment visit, trained research staff explain the study procedures, risks, and strategies to minimize risk during the informed consent process.
Additional consent provisions for collection and use of participant data and biological specimensIn addition to providing informed consent, enrolled participants are required to provide permission for the researchers to use their personal health information for the study. Specifically, participants are asked to authorize the release of their HIV/AIDS treatment information (i.e., lab reports of HIV viral load, HIV care medical visit dates) from the community-based FQHC for the research.
InterventionsExplanation for the choice of comparatorsThe comparator in this trial is the community-based FQHC’s existing Ryan White medical and coordinated case management services as usual. Their UC includes outpatient/ambulatory medical care, AIDS Drug Assistance Program (e.g., through Medicare, Medi-Cal), oral healthcare, early intervention services, mental health services, health education, medical nutrition therapy, medical case management, substance use disorder outpatient services, and support services (e.g., emergency financial assistance, food pantry, housing services, medical transportation, and legal services).
Intervention descriptionThe PATH intervention integrates two theoretically grounded interventions developed by the team of investigators—a peer navigation intervention and an mHealth tool—with the goal of amplifying the impact of peer navigation on viral suppression among Hispanic and Black PLWH.
The peer navigation component is informed by our prior research developing “Conexiones Saludables” (“Healthy Connections” in Spanish; “Conexiones” for short), which is a theory-based intervention including modularized training for peer navigators to build core competencies in supporting marginalized PLWH [29, 30]. Peer navigators undergo 3 weeks of daily modularized training (15 modules total). Conexiones also included peer-delivered “peer empowerment sessions” designed to promote information, motivation, and behavioral skills (self-efficacy) in HIV care engagement and ART adherence, especially in the context of co-occurring conditions like substance use and mental health conditions. Sessions are conducted on a one-on-one basis between the participant and their assigned peer navigator and are delivered monthly over approximately 6 months using motivational interviewing techniques to facilitate intrinsic motivation for behavior change [31]. The design of Conexiones was based on the Situated Information, Motivation, and Behavioral skills (IMB) Model [32], which outlines how behavioral skills to engage in HIV care and adhere to ART should be situated to one’s specific socio-structural context, such as substance use or cultural norms in order to enact behavior change (e.g., ART adherence) [32, 33]. For example, providing information about ART adherence strategies aligned with drug use patterns, understanding sociostructural factors, such as intersectional stigma and discrimination, affecting motivation to engage in healthcare and treatment, and developing behavioral skills, such as self-efficacy, to maintain ART adherence even in a context of substance use stigma in the healthcare setting. In addition to the Situated-IMB Model, Conexiones was also founded in the Theory of Triadic Influence [34], a multilevel Social Cognitive theory [35] that hypothesizes three “streams of influence” (individual, social, and structural) which may act simultaneously to affect self-efficacy to engage in healthy behavior. Operationalized to the health behavior context of Hispanic and Black PLWH, the streams of influence most relevant to PATH include individual-level barriers (being a racial/ethnic minority, substance use) and socio-structural level barriers, such as or substance use stigma or medical mistrust, that decrease both Hispanic and Black people’s engagement in health and HIV care [18,19,20, 36,37,38,39]. Conexiones pilot data demonstrated improvement in HIV care continuum outcomes among marginalized Hispanic PLWH, such as people who use and/or inject drugs, in the US-Mexico border region [29, 30, 40].
The mHealth component of PATH is informed by “LinkPositively,” a mobile-optimized web application (or “webapp”) aimed at improving engagement in the HIV care continuum [41]. The LinkPositively intervention includes interactive features that were based on the IMB model [32, 42]. For example, the webapp incorporated information relevant to HIV self-management (educational and self-care tips feature), motivational enhancements (social support via a feed that participants can post to and reply to comments from other participants and gamification features), and behavioral skills (ART self-monitoring feature) to improve ART adherence. Based on focus group and community feedback, adaptations were made to the original Conexiones and LinkPositively interventions to make them more culturally tailored for both Hispanic and Black PLWH (e.g., creating English and Spanish language versions, using images that both Hispanic and Black participants may identify with).
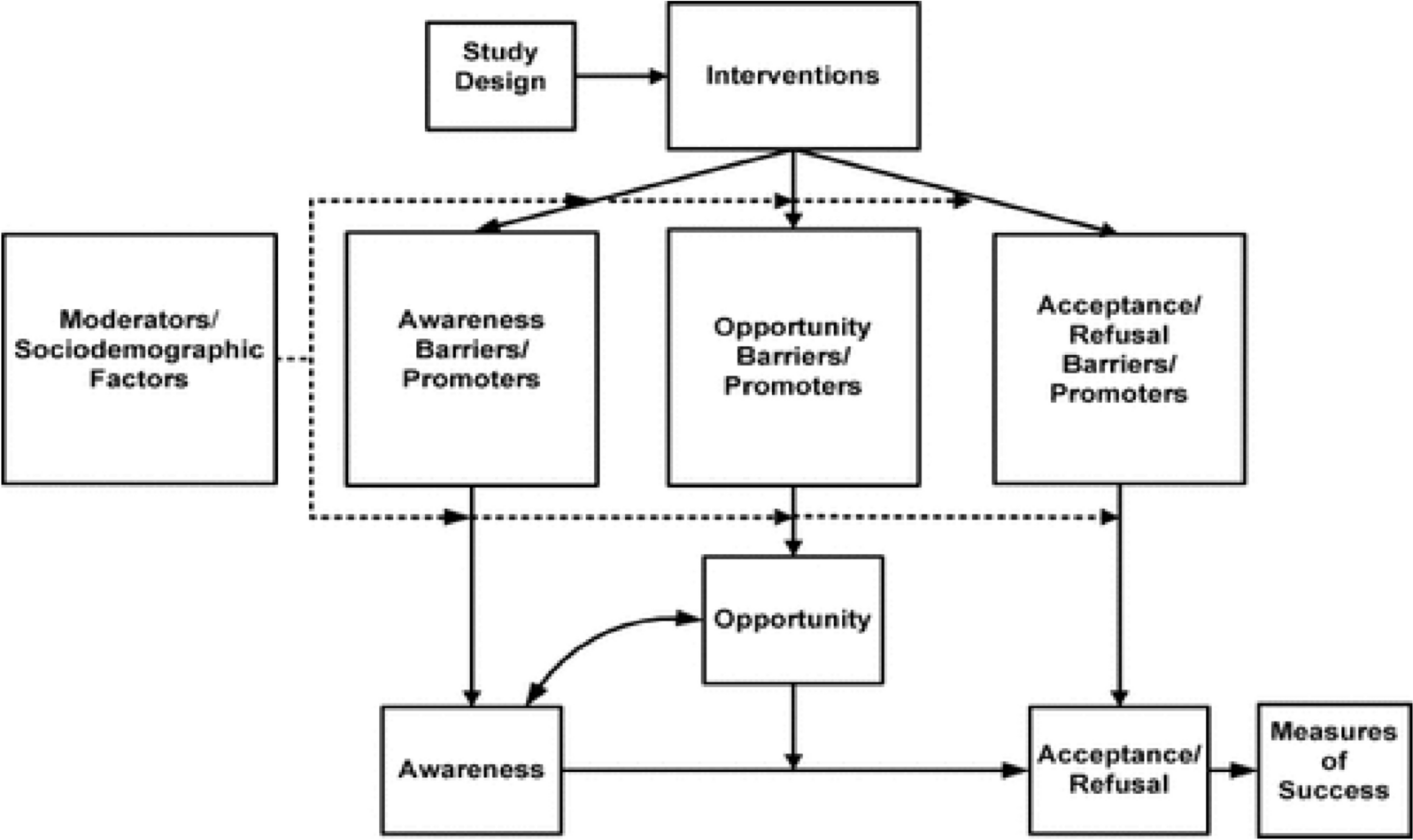
Applying the theoretical foundations that informed the PATH peer navigation and mHealth components, Fig. 1 summarizes how PATH is hypothesized to target multiple psychological and social mechanisms of action, which should ultimately lead to a potent impact on HIV care outcomes among Hispanic and Black PLWH. Overall, participants assigned to the PATH intervention arm are assigned to receive support from one peer navigator and have access to the PATH webapp. Peer navigators meet with their clients at least monthly to deliver peer empowerment sessions. Empowerment sessions occur during the first 6 months, after which participants continue to have access to their peer and the PATH webapp for 12 months total, for example by messaging the peer through the PATH webapp. As much as possible, the study aims for peers to reflect the patient population by recruiting peers who speak English and Spanish, and who are Hispanic or Black. The PATH webapp is available in both languages. Translations of the webapp content were first translated then back-translated and reviewed for cultural and linguistic accuracy.
Fig. 1
Summary of PATH intervention features and the theory-informed mechanisms of action that are hypothesized to produce effects on the primary and secondary outcomes
Criteria for discontinuing or modifying allocated interventionsThe outcome analysis will follow the intent-to-treat approach. Under no circumstances is it possible for the allocated intervention (i.e., usual care or PATH intervention) to be modified once the participant has been enrolled in the trial. However, participants may be unenrolled from the study at any point due to voluntary withdrawal for any reason.
Strategies to improve adherence to interventionsFor participants randomized to the PATH intervention arm, a number of strategies are used to promote adherence to the intervention. These include intensive one-on-one training on how to use the PATH webapp and its features, including re-training upon request. Upon randomization to the intervention arm, participants are also asked to sign a client confidentiality agreement which outlines how PATH intervention participants can expect to receive professional, timely, respectful, and trustworthy peer support. Finally, whenever possible, all clients receive a “warm handoff” to immediately meet their assigned peer navigator over Zoom or in person following randomization into the PATH arm.
Relevant concomitant care permitted or prohibited during the trialOne of the study eligibility criteria is that participants must not currently be enrolled in any other program, intervention, or research study designed to improve HIV adherence or engagement in HIV care (regardless of intervention approach). While this is assessed during screening procedures, if a participant were to receive HIV care and/or ART adherence support from another program or research study during their participation in the trial, this information is recorded during follow-up assessments but does not require disenrollment from the trial.
Provisions for post-trial careParticipants will not be provided any additional care outside of UC from the community-based FQHC.
OutcomesThe primary outcome in this trial is sustained viral suppression, defined as an HIV viral load at 6 and 12 months post-enrollment of less than 200 copies/mL. Secondary outcomes include the following variables: Retention in HIV care (at 6- and 12-month follow-up) is assessed through chart review using the HRSA definition of having greater than or equal to 2 HIV medical visits at least 90 days apart within the 12-month follow-up. Gap in HIV medical visits is measured through chart review at 6 and 12 months using the HRSA definition (no HIV medical visits in the last 6 months) [43]. ART adherence is measured using the self-report Wilson-3 scale [28] at 3-, 6-, 9-, and 12-month follow-up. The secondary outcomes were chosen to fill gaps in outcome measurements in the HIV peer navigation intervention literature [17] and to have a broader representation of the stages of engagement in the HIV care continuum [4].
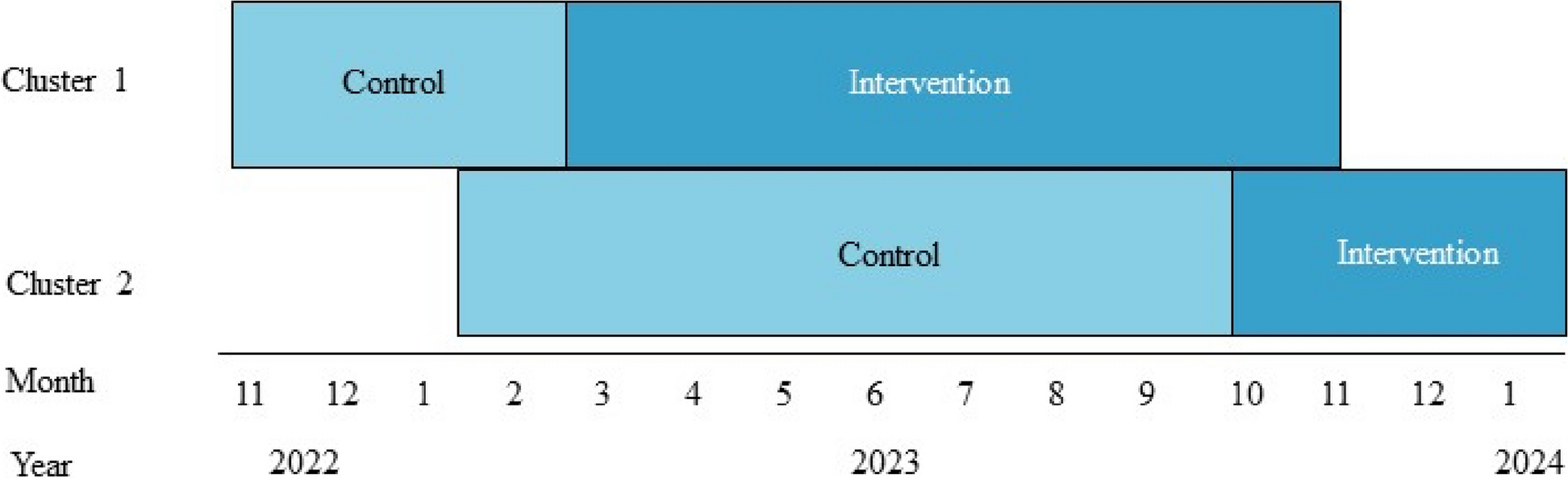
Participant timelineInterested participants meet with study staff (in person or over the phone) to complete a screening questionnaire. Once eligibility criteria are verified by study staff, the participant is asked to complete enrolment procedures within 30 days of completing screening. If 30 days have passed since the screening, the participants must be re-screened again to verify that they continue to be eligible for the study. Study enrolment procedures consist of the informed consent process, authorization to release personal health information for the research, completing a “locator” form to share details for future contact with the participants, and completing the baseline assessment through self-administration via an online survey tool (Qualtrics, Provo, UT). Only after these procedures have been completed, including the baseline assessment, are participants officially enrolled in the study and randomly assigned to either the control or the PATH intervention arm. Assignment to study arm is concealed to both study staff and participants until this final stage. A schematic of the participant timeline in the RCT is shown in Fig. 2.
Fig. 2
Schematic of participant timeline in the PATH RCT. *Participants are allowed to finish enrollment activities up to 30 days after they initially screen for eligibility, after which point they are required to re-screen. **Participants who are randomly allocated to the PATH intervention arm immediately complete intervention onboarding activities, which include assignment to their PATH peer navigator, creation of their account for the PATH web application, and in-depth tutorial on how to log into the PATH app and its features
Sample sizeIt was estimated that a sample size of up to 375 total participants would be required to achieve study objectives. This estimate was informed by a sample size calculation. Figure 3 displays power and sample size estimates based on intervention effect sizes and covariates. Meta-analytic data from Finitsis et al. [44] of mHealth text messaging interventions to promote ART adherence among PLWH has shown that such interventions can improve VL suppression (k = 3; OR = 1.57, 95% CI = 1.11, 2.20). This OR of 1.56 is a small effect size, and Chen et al. [45] established conventions of small, medium, and large ORs (similar to Cohen’s magnitudes of effect size, d). Based on the Finitsis meta-analysis (OR = 1.57), and accounting for other possible effect sizes of small (OR = 1.68) or medium (OR = 3.47) magnitude (based on Chen et al.) [45], the required sample sizes to achieve adequate power of at least 0.85 ranges from n = 179 to 204; with covariates in the model (accounting for 25% of the variance in the outcome, then a sample size ranging from n = 263 to 339 would be required). To provide further support for this power analysis, we conducted another analysis in G*Power using an effect size estimate from a recent peer navigation intervention (that does not include a mHealth component, “LINK LA” [46]) for HIV-positive men and transgender women released from jail. In this study, the investigators tested the efficacy of their peer navigation intervention compared to usual care (case management) and found a 22% difference-in-difference between the intervention and control arm on viral suppression over a 12-month follow-up. Using this effect size information, and assuming 0.80 power, alpha = 0.05, and 1:1 allocation ratio between intervention and control arms, the required sample size is 97 per group, or a total n of 194. Altogether, our calculations to estimate the desired sample size with adequate power and, based on up to 20% anticipated attrition, a sample size between 225 and 375 would provide us with adequate power to achieve our aims. Thus, our goal is to randomize up to 375 participants for an analytic sample size of ~ 300 (150 per arm).
Fig. 3
Power and sample size estimates based on small, medium, and large intervention effect sizes and covariates
RecruitmentParticipants are recruited internally within the community-based FQHC. The clinic data team regularly creates, updates, and shares a list of potentially eligible patients based on their recent HIV care history with the research team. Clinic staff also help to recruit from their patient population by reviewing clinic schedules weekly to identify participants with a pending appointment who might qualify based on the eligibility criteria for on-site recruitment. Other clinic staff, such as case managers and general medical staff, are informed of study details and eligibility to provide preliminary study information and refer potential participants. Research staff also work with other teams within the HIV Department to promote the study. The clinic’s community advisory board also serves as a resource for informing potential participants that the study is occurring, and study participants can also refer friends. When a patient is identified to be potentially eligible for the study (e.g., through clinic staff referral, or by reviewing clinic data), study staff attempt to recruit the individual, usually by phone. Study staff introduce the study and provide the next steps for interested patients. Those not interested are given an opt-out option to limit further contact from the team.
留言 (0)