Osmotic Demyelination Syndrome Associated with Uremia and Elevated Serum Osmolality
Osmotic demyelination syndrome has been historically reported in cases with rapid correction of hyponatremia and rarely in cases of severe hypernatremia. In 2013, an expert panel recommended a maximum daily sodium correction rate of 8 mEq/L in high-risk hyponatremic patients and 10–12 mEq/L in those not at a high risk [9, 12]. There is controversy surrounding the pace of hyponatremia correction and risk of ODS with recent retrospective studies reporting weak correlation between the two [11, 15]. Macmillan et al. [11] noted that ODS is rare, occurring in 12 of 22,858 hospitalizations for hyponatremia. Of these 12 patients, 7 did not have a sodium correction rate > 8 mEq/L/day [11]. Another large retrospective study of 1024 patients admitted to the intensive care unit with severe hyponatremia noted that rapid correction (> 8 mEq/L/24 h) was associated with lower in-hospital mortality, longer intensive care unit and hospital-free days, and no significant difference in neurological complications [16]. Therefore, it is critical to understand the physiology underpinning transcellular fluid movement across the blood–brain-barrier (BBB) to understand the pathogenesis of ODS.
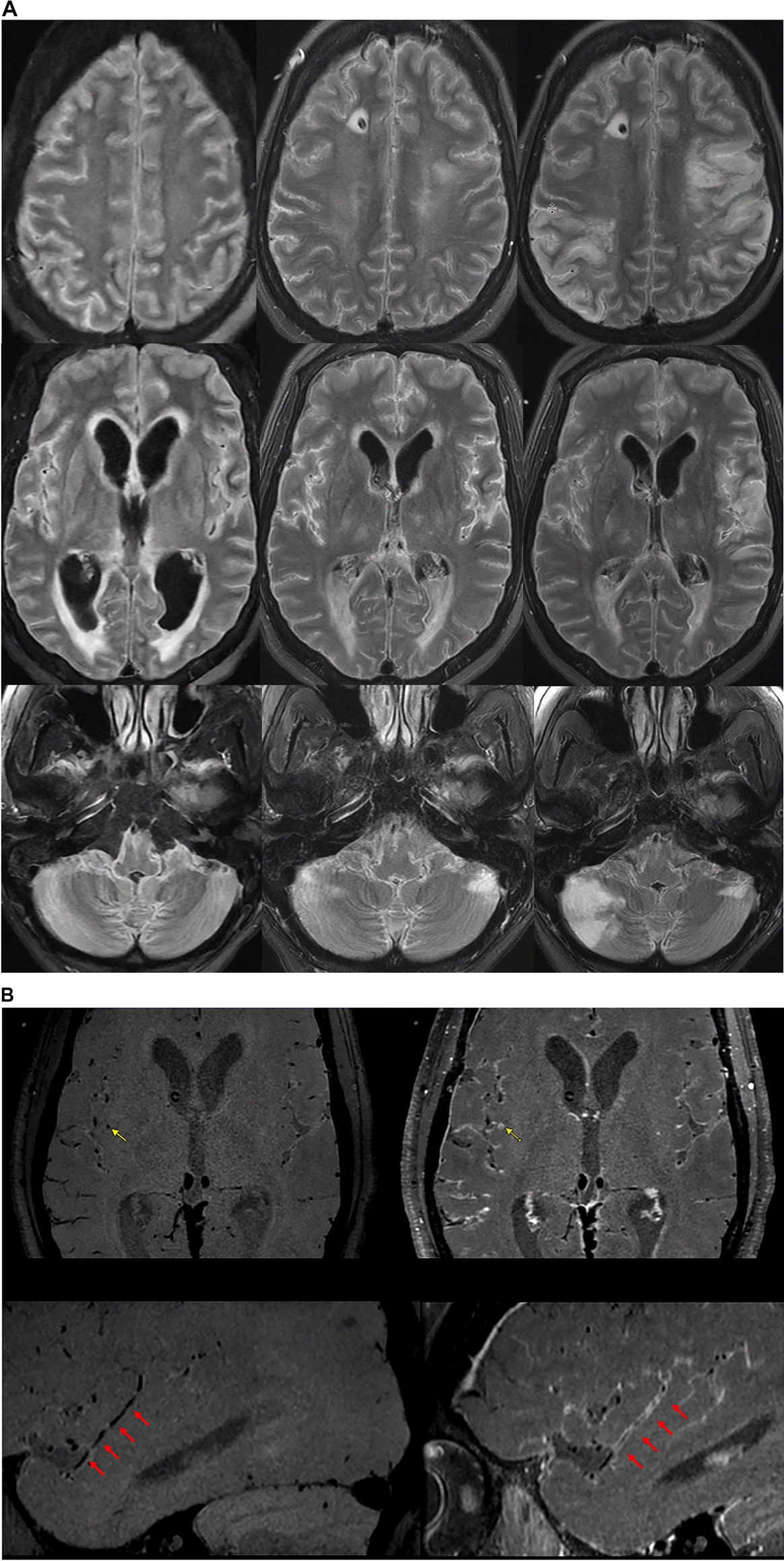
Acute increases in serum osmolality can trigger osmotic fluid shifts across the BBB, decreasing the volume of neuronal and glial cells [2]. The BBB prevents the passage of sodium. Abrupt increases in serum sodium levels can result in significant adjustments to the volumes of neuronal and glial cells, leading to demyelination and programmed cell death (ODS) [2]. Cells can adapt by uptake of intracellular osmoles to prevent shrinkage, although it is unclear how fast this adaptation can occur. The reflection coefficient, ranging from 0 to 1, is an index of the effectiveness of the solute in generating an osmotic driving force across the neuronal membrane. Sodium has a reflection coefficient of 1.0 across the BBB meaning that it is effectively excluded from diffusing into brain [2, 17].
Urea, possessing a reflection coefficient of about 0.5, only partially traverses the BBB as a solute [2, 17]. As a result, rapid and large increases in serum BUN levels can also contribute to the creation of an osmotic gradient across the BBB, promoting movement of water away from the brain and shrinking the sizes of neurons and glial cells [2, 18]. In our patient, although the elevation in serum sodium levels was gradual and did not exceed daily increments of 8 meq/L, the surge in effective serum osmolality over a few days due to a rapid rise in serum BUN levels resulted in osmotic fluid shifts [19]. This case highlights how both sodium and BUN levels need to be monitored when trying to prevent secondary neurological injury due to osmolality and fluid shifts.



留言 (0)