Patients and Study Design
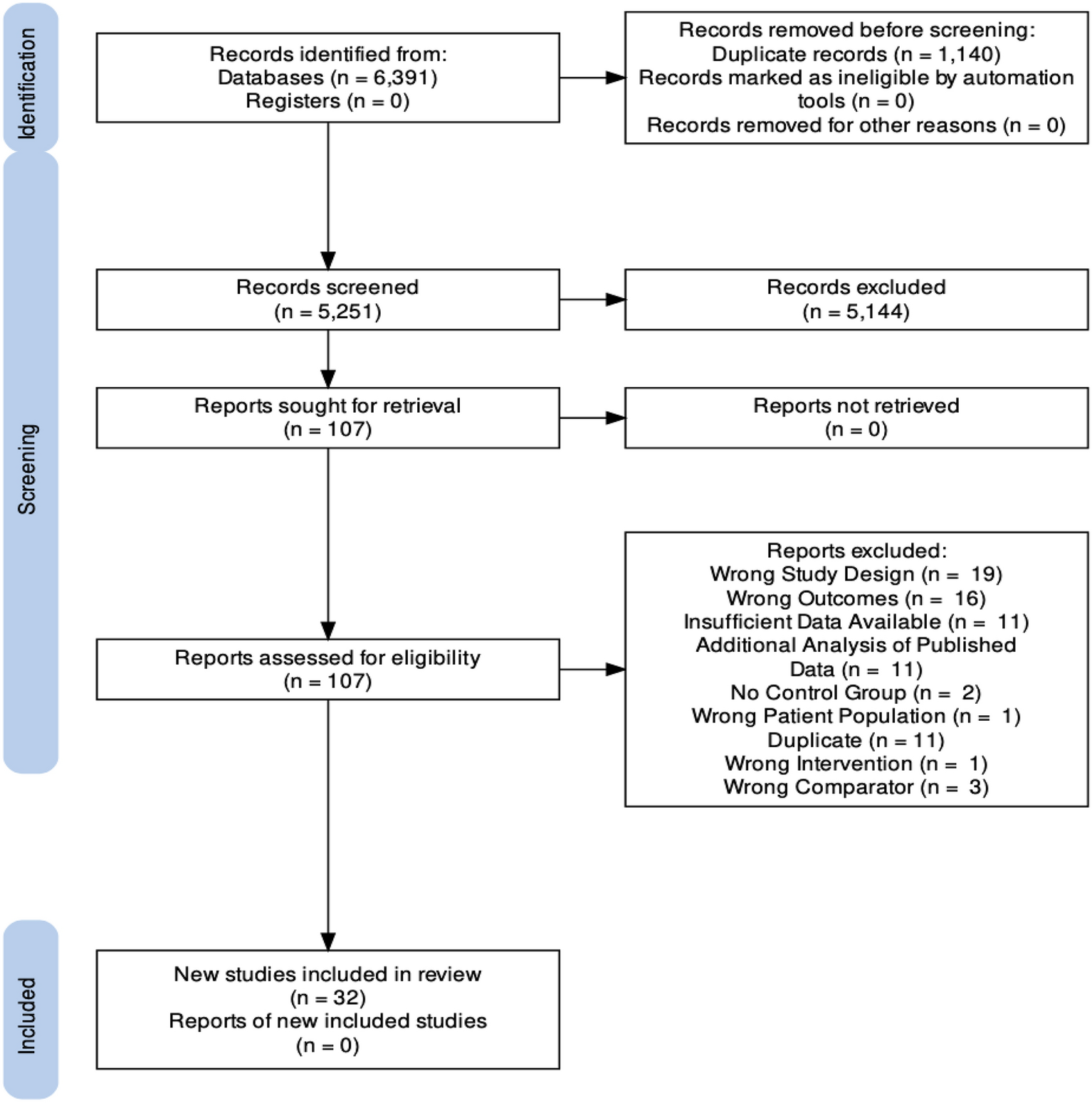
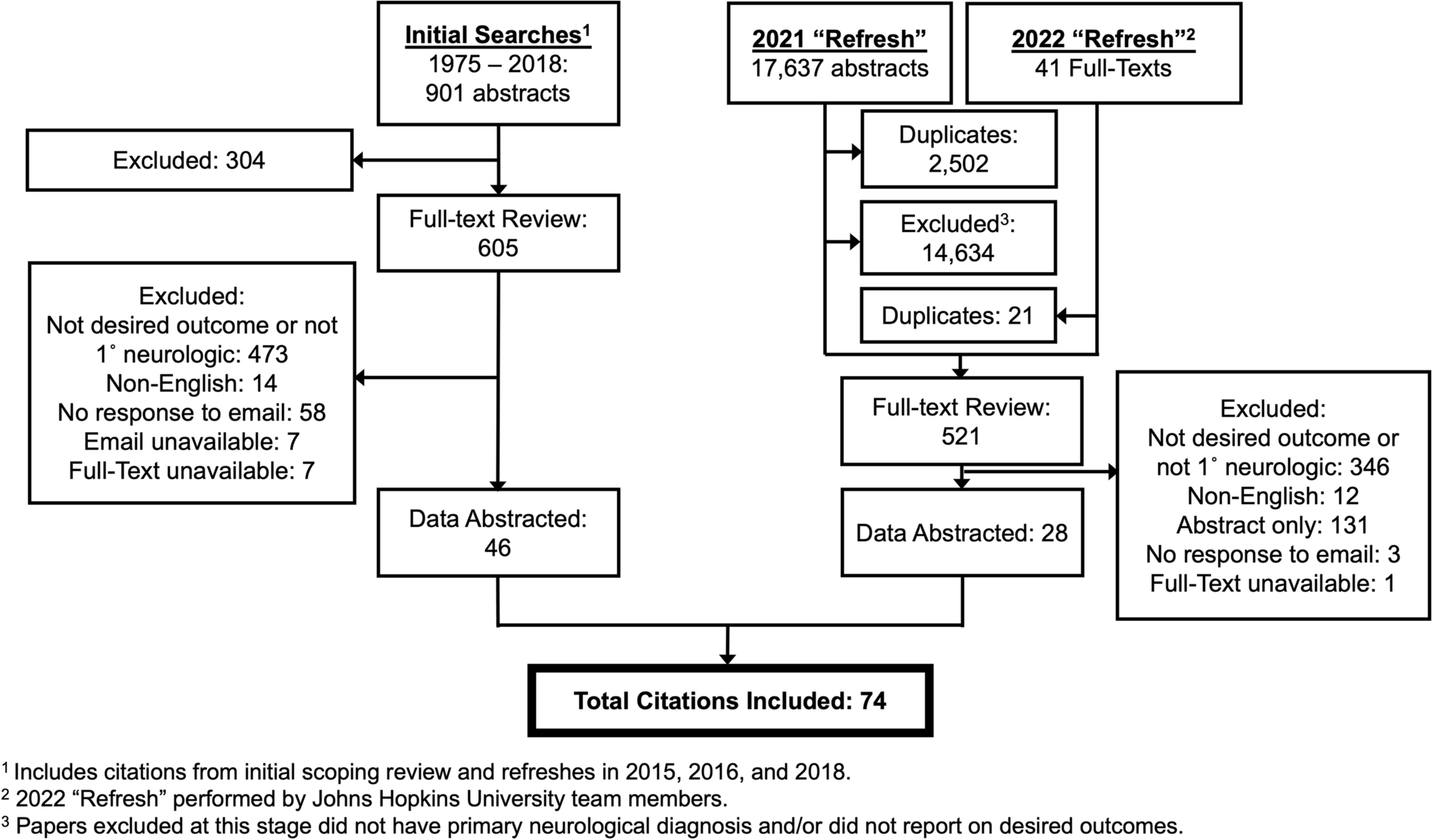
This was an observational study, conducted at the Department of Neurosurgery, Uppsala University Hospital, Uppsala, Sweden. Of 490 patients with TBI who were older than 15 years, received ICP monitoring, had at least two computed tomography (CT) scans the first 48 h, and were treated in our neurointensive care unit between 2008 and 2018, 105 were excluded (missing outcome data = 42, less than 12 h of ICP data the first 7 days = 63). Thus, the final study population included 385 patients.
Neurointensive Care Management Protocol
The patients were treated according to our standardized ICP-oriented and CPP-oriented TBI management protocol, which has been described in detail in previous studies [3, 28]. Treatment goals were as follows: ICP ≤ 20 mm Hg, CPP ≥ 60 mm Hg, systolic blood pressure ≥ 100 mm Hg, partial pressure of oxygen ≥ 12 kPa, arterial glucose level of 5–10 mM, hemoglobin level ≥ 10 g/dL, electrolytes within normal ranges, normovolemia, and body temperature < 38 °C.
Unconscious (Glasgow Coma Scale Motor score (GCS M 1–5)) patients were intubated, mechanically ventilated, and given propofol and morphine for sedation and analgesia, respectively. ICP was monitored with an external ventricular device (EVD; HanniSet, Xtrans; Smiths Medical GmbH, Glasbrunn, Germany) or an intraparenchymal sensor device (Codman ICP Micro-Sensor; Codman & Shurtleff, Raynham, MA) in unconscious patients. Surgical evacuation was performed in patients with significant intracranial mass lesions. The basic management included head elevation to 30° and mild hyperventilation (partial pressure of carbon dioxide 4.0–4.5 kPa) if ICP was increased. Neurological wake-up tests were done three times per day but not if ICP remained elevated. If ICP was still increased in the absence of mass lesions, an EVD was used to drain cerebrospinal fluid. If ICP was still refractory elevated, stress was treated with increased sedation, β1-antagonists, and α2-agonists. Last-tier treatments to control ICP included thiopental infusion and/or decompressive craniectomy (DC).
Functional Outcome
Functional outcome was evaluated according to the Glasgow Outcome Scale-Extended (GOS-E) 6 months post injury. The scale has eight categories and ranges from death (1) to upper good recovery (8) [29, 30]. The assessments were conducted by specially trained staff using structured telephone interviews with the patients if they had recovered sufficiently and otherwise with their closest relative. Favorable and unfavorable outcomes were classified as GOS-E scores 5–8 and 1–4, respectively.
Radiological Analysis
Volumetric (mL) assessments of contusions were performed based on the first two CT scans in the Brainlab software by one of the authors (TSW). To also assess the extra-axial hemorrhage burden, similar volumetric assessments were conducted for epidural hematomas (EDHs), acute subdural hematomas (aSDHs), and intraventricular hemorrhage (IVH). Only the sum of each hematoma type was reported (e.g., a reported contusion volume of 10 mL could reflect two contusions of 5 mL each). Presence/absence of traumatic subarachnoid hemorrhage (tSAH) on any of these two scans was also assessed; however, it could not be properly quantified volumetrically. Furthermore, the midline shift and the extent of compression of the basal cisterns (open, compressed, or obliterated) were evaluated. The highest value of the bleeding volume, midline shift, and basal cistern compression on any of the two CT scans was used in the statistical analyses. The Marshall classification was also assessed based on the first CT scan by the same author (TSW) [25]. We used 10-mL contusion volume as the cutoff to dichotomize patients into (1) significant contusion and (2) small/no contusion (but potentially extra-axial or diffuse injuries). We chose this cutoff a priori because it included contusions that were large enough to be significant, although they did not necessarily require surgical evacuation in all cases (e.g., surgery was usually only done for contusions sized 25 mL and above) [25]. The cutoff at 10 mL was similar to that in the Surgical Trial In Traumatic intraCerebral Haemorrhage (STITCH) trial [31].
Data Acquisition and Analysis
The physiological variables (ABP and ICP) were recorded at 100 Hz using the Odin software [13]. ABP was measured in the radial artery at heart level. ICP was monitored with either an EVD with the transducer at the level of foramen of Monro or an intraparenchymal probe. If a patient had both an intraparenchymal monitor and an EVD, only the ICP from the EVD was registered and analyzed. PRx was calculated as the 5-min correlation of 10-s averages of ICP and mean ABP [12, 14]. CPPopt was continuously calculated as the CPP with the lowest PRx the last 4 h [10,11,12]. The physiological variables were down-sampled and analyzed as minute-by-minute values. PRx and CPPopt were calculated in retrospect and were not available at the bedside. The physiological variables were analyzed during the first 7 days after injury.
Good monitoring time (GMT) was defined as the total monitoring time (in minutes) subtracted by the time when the data acquisition was interrupted (e.g., when the patients left neurointensive care for surgery) and after removal of artifactual values. The %GMTs with ICP > 20 mm Hg, PRx > 0.30, CPP < 60 mm Hg, CPP within 60–70 mm Hg, CPP > 70 mm Hg, ΔCPPopt less than − 5 mm Hg, ΔCPPopt ± 5 mm Hg, and ΔCPPopt > 5 mm Hg were analyzed during the first 7 days post injury. The ICP threshold was chosen according to our management protocol [3]. The CPP thresholds were defined according to the Brain Trauma Foundation guidelines [5]. We chose PRx > 0.30 as a threshold because PRx between 0.20 and 0.40 has been associated with unfavorable outcome [32] and has also been estimated as the lower limit of autoregulation [8]. The ΔCPPopt threshold at 5 mm Hg was chosen in accordance with the CPPopt Guided Therapy: Assessment of Target Effectiveness (COGiTATE) trial [9].
Visualization of Combined Insults
To study the combined role of the absolute PRx/CPP thresholds a two-dimensional plot was conducted, which illustrated the correlation between %GMT of various PRx/CPP combinations and GOS-E. This method has been developed by our group and has been described in detail in a previous study [17]. These plots were created for the significant contusion and the small/no contusion groups. The %GMT during the first 7 days after injury for combinations of PRx (range − 1 to + 1 with a 0.05 resolution) and CPP values (range 40–100 mm Hg, with a 2-mm Hg resolution), yielding a grid of 1,200 cells (40 × 30), was calculated for all patients in each cohort and analyzed in relation to GOS-E with the Spearman test. To reduce high-frequency noise, each pixel was divided into 3 by 3 smaller pixels, followed by a Gaussian smoothing (standard deviation = 2). The final values for each pixel were translated into the jet color range (red to blue) with red/blue color indicating a negative/positive association with GOS-E. The jet color scale was limited to a ± 0.30 correlation coefficient range because of the moderate correlation strength. Pixels with fewer than five patients with at least 5 min of monitoring time were colored as white. Furthermore, a density plot was conducted to visualize the frequency of the %GMT for certain combinations of PRx and CPP. The resulting numbers were divided by the highest count within the grid to yield density values ranging from 0 to 1 for each cell in the grid. Gaussian smoothing was also applied here, and the final values were then transformed to colors using the jet color scale and plotted. Furthermore, similar plots were done with ∆CPPopt, instead of CPP, in combination with PRx in relation to GOS-E.
Statistical Analysis
Nominal variables were presented as numbers (proportions), and ordinal/continuous variables were presented as medians (interquartile range [IQR]). Differences in demographics, admission variables, treatments, outcome, imaging, and cerebral physiology between those with significant contusions and those with small/no contusions were evaluated with the Mann–Whitney U-test or the χ2 test, depending on the type of data. The association of the %GMTs within/outside the thresholds of ICP, PRx, CPP, and ΔCPPopt with GOS-E was assessed with the Spearman test for the significant contusions and the small/no contusions groups, separately. Multiple logistic regressions with unfavorable outcome (GOS-E scores 1–4) as the dependent variable and age, GCS M, pupillary status, and the %GMTs of ICP > 20 mm Hg, PRx > 0.30, and CPP within 60 to 70 mm Hg as independent variables were conducted for the significant contusions and the small/no contusion groups, separately. The independent variables were similar to those in the International Mission for Prognosis and Clinical Trials in Traumatic Brain Injury (IMPACT) core model (age, GCS M, and pupillary status) [33], in addition to being within/outside the explored ICP, PRx, and CPP thresholds. We chose CPP within 60–70 mm Hg because this interval was more strongly associated with GOS-E in univariate analysis than values below or above this interval. In similar regressions, the %GMT of CPP within 60–70 mm Hg was replaced by the autoregulatory target ΔCPPopt ± 5 mm Hg. We chose ΔCPPopt ± 5 mm Hg because this interval was more strongly associated with GOS-E in univariate analysis than values below or above this interval. Missing data were rare (CPPopt could not be calculated in six patients with otherwise complete data), and these patients were excluded from the relevant analyses, i.e., no imputation was done. A p value < 0.05 was considered statistically significant. We abstained from adjustment for multiple comparisons because this was an exploratory study. The statistical analyses were conducted in RStudio software (version 2022.12.0) [34].
Ethics
All procedures performed in the studies involving humans were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki Declaration and its later amendments. The study was approved by Uppsala University Regional Ethical Board (Dnr: 2022–06526-02). Written informed consent was obtained during neurointensive care or follow-up by most patients or their relatives but was waived if the patient/relatives could no longer be reached.




留言 (0)