This study summarized the etiological distribution characteristics and corresponding clinical manifestations of 167 children with DRE, establishing a foundation for the precise diagnosis and treatment of pediatric DRE. 53.3% exhibited identifiable causes, predominantly structural, followed by genetic causes, with a minority having immunological or multifactorial etiologies. Onset ages varied among different causes, with genetic causes manifesting earlier than structural and immunological ones. Regarding clinical presentations, 60 cases displayed a specific epileptic syndrome, among which 36 cases (60%) had onset in the neonatal and infantile period. In the 107 cases of non-syndromic epileptic syndromes, 53 cases (49.5%) were characterized by focal epileptic seizures, and 40 cases (37.3%) presented with diverse seizure types.
The pathogenesis of DRE remains somewhat elusive to date. However, numerous studies have proposed several primary hypotheses through in vivo or in vitro experiments, including the drug transporter hypothesis, neural network hypothesis, drug target hypothesis, genetic mutation hypothesis, disease severity hypothesis, and pharmacokinetic hypothesis. Yet, these hypotheses have inherent limitations and areas where they overlap [14]. Presently, the role of neuroinflammation in the pathogenesis of DRE is gradually being elucidated. Neuroinflammation can result in compromised blood-brain barrier, neuronal loss, and excessive neuronal excitation, not only triggering epileptic seizures but also correlating with the occurrence of DRE [15]. Recent research has demonstrated that neuroinflammation could potentially serve as a common underlying mechanism among various hypotheses in DRE and might be a prospective target for its treatment [16]. Promising therapeutic effects and safety have been observed in DRE and status epilepticus with drugs targeting IL-1, IL-6, and CD20 [17]. However, clinical data on this front remains limited, warranting further research for validation.While the pathogenic mechanisms of DRE are still in the exploratory phase, the analysis of etiology can also offer instructive significance for therapeutic interventions.
Children with imaging abnormalities are more likely to develop DRE than children with normal imaging [18]. Malformations of Cortical Development (MCD) constitute the principal congenital structural anomalies. Acquiring structural cerebral abnormalities, primarily due to hypoxic-ischemic encephalopathy or hypoglycemia brain damage, is a major etiological factor in the onset of DRE during infancy [19]. Subsequently, residual foci of cerebral softening and glial proliferation following encephalitis represent another notable contributing factor. It has been documented that approximately 10% of pediatric encephalitis patients progress to DRE, with the herpes simplex virus (3/9, 33%) and unidentified (8/40, 20%) forms of encephalitis accounting for relatively common causative agents [20]. For children with structural lesions, it is imperative to embark on an early surgical evaluation, unhampered by considerations of age, coexisting medical conditions, or the type of seizures [18]. There exists compelling evidence supporting the supremacy of surgical intervention over pharmaceutical approaches in the treatment of DRE in children [8]. In cases where epilepsy is precipitated by a well-defined lesion within the nonverbal cortex, the contemplation of preoperative evaluation should be undertaken even before the onset of drug-resistant epilepsy [21].
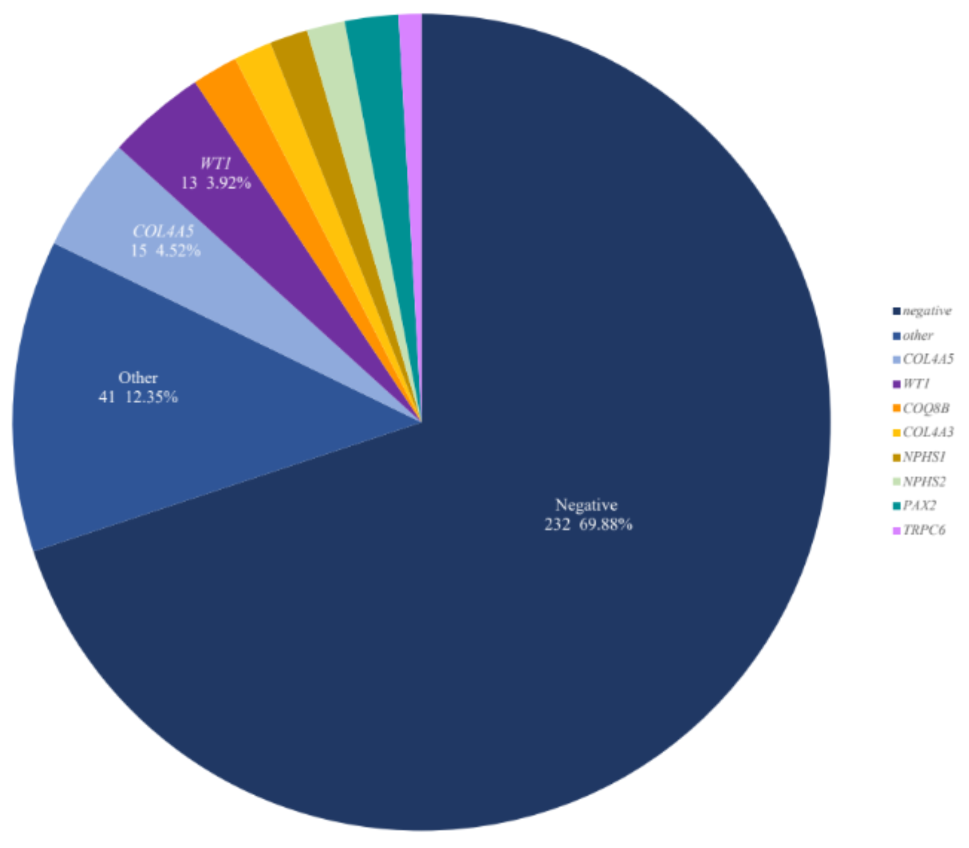
The genetic etiology is closely linked to drug-resistant epilepsy, particularly in severe cases of DEES such as the majority of Dravet syndromes where resistance to medication is commonly observed [22]. Approximately 80% of Dravet syndrome cases are associated with SCN1A variation [23], which aligns with the findings of this study. Additionally, IESS patients are also commonly associated with genetic factors, and cognitive dysfunction and stagnation are among its clinical phenotypes [24]. Predominantly, genetic variations are attributed to ion channel genes, including but not limited to SCN1A and KCNQ2, echoing the observations of Liu et al [25, 26]. DRE related genes also include enzyme regulators,exemplified by CDKL5, elements of cellular metabolism and signal transduction, typified by FGF12, and cell adhesion molecules such as PCDH19. It is worth noting that in this study, a child with chromosome copy number variation was found to have 13.6 Mb deletion in the 18q22.1q23 region, and its clinical manifestations included microcephaly and comprehensive developmental disorder in addition to DRE [27]. Reportedly, copy number variation (CNV) constitutes approximately 10% of hereditary epilepsy cases [28]. An international study has illuminated the transformative potential of a definitive genetic diagnosis in the realm of clinical management [29]. It has been unveiled that when clinical management was tailored in response to genetic testing outcomes, approximately 64.7% of patients witnessed a reduction or even elimination of seizures.This underscores the profound influence of genetic testing on enhancing patient outcomes among individuals grappling with epilepsy [29].
The significance of immunological factors in DRE should not be disregarded. In 2020, the ILAE introduced the term “autoimmune epilepsy” denoting the persistence of seizures despite appropriate immunotherapy without substantial evidence of inflammatory activity [30]. This condition can manifest in patients displaying high titers of GAD65 antibodies, tumor-related antibodies, and Rasmussen’s encephalitis. It also encompasses a small subset of patients who continue to experience seizures even after the acute phase of autoimmune encephalitis has passed. Unlike acute symptomatic seizures secondary to autoimmune encephalitis, autoimmune-related epilepsy manifests as drug-resistant. Even after adequate immunotherapy for the primary condition and standardized anti-seizure treatment, seizures persist chronically and long-term, proving challenging to control solely through medications. Research suggests that neuronal apoptosis induced by T cell cytotoxicity stands as the central pathological mechanism, potentially resulting in structural damage to the cerebral hemisphere. The presence of antibodies might represent a consequential byproduct in this pathological process, hinting that comprehensive immunotherapy might not effectively diminish seizure frequency [31]. Therefore, clinicians are encouraged to consider timely immune-targeted therapy, symptomatic supportive treatment, and actively explore opportunities for surgical intervention to potentially enhance disease prognosis.
Within the scope of this study, twelve children exhibited a dual etiology involving genetic factors along with structural or metabolic elements. These etiological factors may be either causally related or act independently. Among them, four cases presented with tuberous sclerosis (TSC) evident on MRI scans. Three cases were found to harbor variants in the TSC1 gene, while one case exhibited variants in the TSC2 gene. These gene variants are situated within the mTOR pathway and are known to trigger excessive activation of the mTOR pathway. This, in turn, disrupts normal cell proliferation and ultimately contributes to the development of malformed cerebral cortex, a condition closely associated with the onset of DRE [32]. Furthermore, three cases exhibited epileptic seizures attributable to mitochondrial gene variants (POLG, MT-TL1, DNM1L), as documented in previous studies [33,34,35]. Mitochondria-associated epilepsy entails a multifaceted pathogenesis, giving rise to various seizure types, predominantly drug-resistant, coupled with multisystem involvement and an unfavorable prognosis [36]. When faced with DRE of indeterminate etiology in a clinical setting, it is imperative to consider the potential involvement of mitochondrial diseases.
In this study, 46.7% of cases had an undetermined etiology, with 48.7% (38 out of 78) attributed to incomplete genetic testing, without excluding the presence of a certain proportion of genetic factors. For children with DRE where the cause is unclear or there is no surgical indication, alternative non-pharmacological therapies can be employed in anti-seizure treatment. Ketogenic Diet (KD), as a traditional non-pharmacological intervention, constitutes a dietary formula characterized by a high proportion of fats, low carbohydrates, and appropriate levels of proteins and other nutrients. By restricting the intake of dietary fiber carbohydrates, thereby emulating the metabolic state of the body under conditions of hunger, it can effectively diminish the frequency and severity of epileptic seizures. KD is applicable to children across various age groups experiencing frequent seizures associated with DRE and metabolic disorders such as Glucose Transporter 1 Deficiency Syndrome (GLUT-1). The therapeutic outcomes demonstrate a reduction of seizure frequency by over 50% in 50–80% of refractory epilepsy cases, achieving complete seizure freedom in 10–20% of cases, and enhancing overall quality of life by improving cognition, behavior, and sleep quality [6]. Another rapidly advancing non-pharmacological therapy is neuromodulation, primarily encompassing Vagus Nerve Stimulation (VNS), Responsive Neurostimulation (RNS), and Deep Brain Stimulation (DBS) [7]. Neuromodulation is applicable to patients with poorly controlled epilepsy who are not suitable candidates for resective surgery. According to research findings [7], the average improvement rate of DRE with VNS therapy is approximately 34.7%. For DBS, there is an average reduction of 41% in seizure frequency after one year. After five years post-surgery, 68% of patients experience at least a 50% reduction in seizure frequency, with 16% of patients achieving seizure-free periods exceeding six months [37]. Regarding RNS, it can completely control about 10–15% of refractory epilepsy seizures [38]. Therefore, it is considered that neuromodulation stands as one of the effective therapeutic choices for DRE. However, each treatment modality possesses its unique advantages and limitations, requiring personalized assessments before formulating a plan.
There are certain limitations in our study to acknowledge: (1)This study is a single-center endeavor, characterized by a relatively modest sample size, potentially introducing a degree of bias in the distribution of etiological factors. (2)The retrospective nature of this study restricts its exploration of etiological factors to a cross-sectional approach. It is thus advisable to embark on a prospective cohort study as the subsequent course of action, allowing for the monitoring of seizures in children with DRE following adjustments in their treatment regimens in accordance with the identified etiology.





留言 (0)