
{kind=link}
{kind=link}
{kind=link}
{kind=link}
記住我
For decades, focal non-invasive neuromodulation of deep brain regions has not been possible because of the steep depth-focality trade-off of conventional non-invasive brain stimulation (NIBS) techniques, such as transcranial magnetic stimulation [1] or classical transcranial electric stimulation [2]. A method that has recently emerged to overcome this challenge is transcranial Temporal Interference Stimulation (tTIS) [3]. The concept of tTIS is to apply two high-frequency (HF) alternating currents (kHz range) through surface electrodes, with a small difference of frequency (Δ f ): the kHz frequencies of the two applied currents are supposed to be high enough to avoid direct neuromodulation [4], yet their interaction will create an envelope that oscillates at the low-frequency Δf and can be focally steered towards specific deep brain structures [3]. This method has been recently translated into human applications for subthreshold modulation of the striatum [5, 6] and the hippocampus [7]. More specifically, these studies showed that when using specific montages of electrodes (based on computational modeling on realistic head models) and when the target deep brain region was concomitantly engaged in a task, tTIS could selectively modulate deep brain activity and the associated behavior. While many questions remain regarding the mechanisms underlying tTIS-based neuromodulation [8], these results suggest that tTIS could be useful for non-invasive deep brain stimulation in fundamental neuroscience as well as in translational research. Importantly, there is evidence that transcranial electrical stimulation is safe and well-tolerated when applied at 2 mA in the form of transcranial alternating current stimulation (tACS [9, 10]) and transcranial direct current stimulation (tDCS, [11, 12]), yet, the tolerability, safety, and blinding profile of tTIS applied to target deep brain structures still has to be demonstrated for a wider use of the technique in systems human neuroscience and towards clinical applications [13].
Here, we share our first experience with deep tTIS by analyzing the safety, tolerability and efficiency of blinding on a large dataset consisting of 257 sessions (119 participants) targeting either the striatum or hippocampus in young and older adults and a small number of patients with traumatic brain injury (TBI).
2.1. Participants119 participants were enrolled in at least one of 8 experiments (figure 1(A)). The cohort was composed of 79 young (46 women, 24.6 ± 0.45 years old [mean ± SE]), 25 older adults (16 women, 66 ± 1.1 years old) and 15 patients diagnosed with TBI (4 women, 50.3 ± 3.3 years old), leading to a total of 257 sessions. All participants gave their written informed consent in accordance with the Declaration of Helsinki and the Cantonal Ethics Committee Vaud, Switzerland (2020-00127).
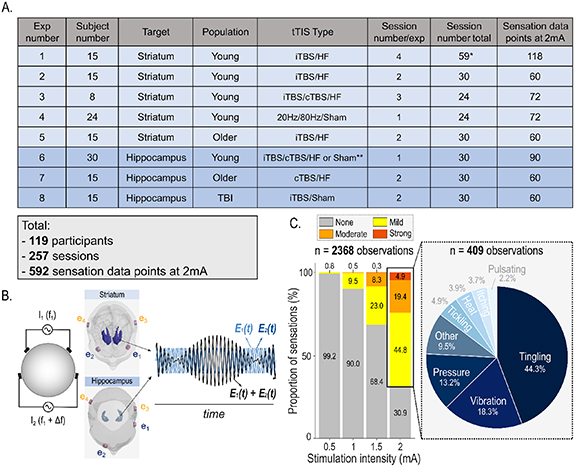
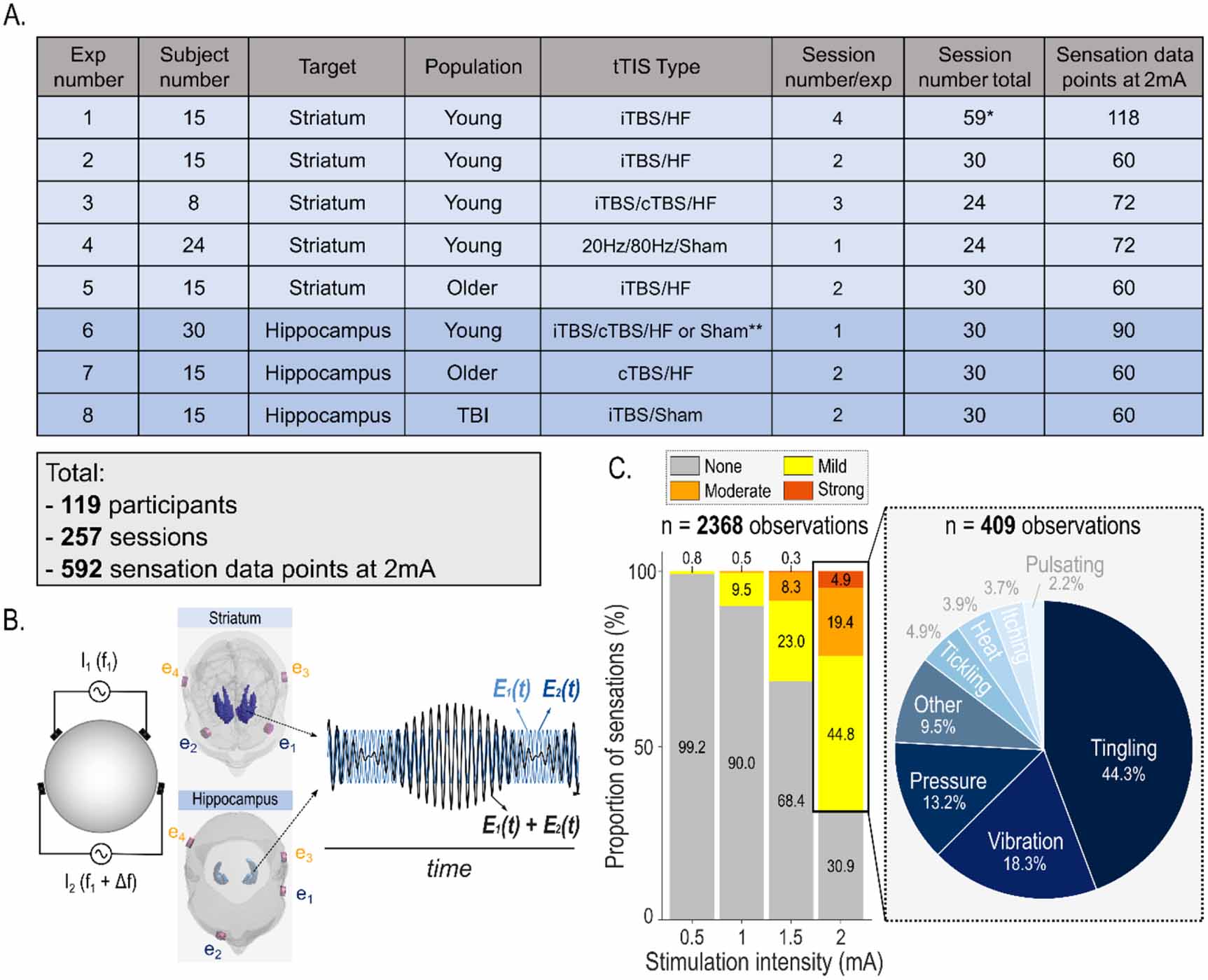
Figure 1. tTIS dataset and elicited sensations. (A) Summary of the dataset including 8 experiments. A total of 257 sessions were performed on 119 participants (15 subjects participated in multiple experiments) leading to 592 reports of elicited sensation at each intensity including 2 mA (i.e. the intensity used during experiments). *: One subject of experiment 1 missed one session, leading to a total of 59 sessions in this experiment. **: Two different placebo conditions were used in this experiment, with 16 participants receiving HF tTIS and 14 experiencing sham tTIS. (B) Concept of tTIS. On the left, two pairs of electrodes are shown on a head model with arrangement of electrodes targeting the striatum bilaterally [5, 6] or the left hippocampus [7]. In the striatal montage, electrode 1 (e1) and 2 (e2) are positioned on the F3 and F4 landmarks of the 10–20 EEG system, while e3 and e4 are positioned on TP7 and TP8, respectively. In the hippocampal montage, e1-e2 and e3-e4 are positioned around the FT7-Fp2 and TP7-P8 landmarks. The two currents are in the kHz range (oscillating at f1 and f1 + Δf) and applied with a small shift in frequency, resulting in a modulated electric field with the envelope oscillating at the low-frequency Δf (target frequency) where the two currents overlap. On the right, the interference of the two electric fields within the targets is represented with high envelope modulation. E1(t) and E2(t) represent the modulation of the fields' magnitude over time. Different types of tTIS were applied in the different experiments (see Methods). C) Magnitude and type of tTIS-related sensations. On the left, magnitude of sensations reported before each experiment for all tTISTYPES for current amplitudes ranging from 0.5 to 2 mA. On the right, type of sensations as described by the participants at 2 mA. Notably, only the descriptions which were used in at least 2% of observations are represented here. The rest of the observations are collapsed in the category 'Other' which accounts for less than 10% of the data. This category includes the following adjectives: 'pinching', 'massaging', 'touch', 'pain', 'stinging', 'shivering', 'bumping', 'screwing'.
Download figure:
Standard image High-resolution image 2.2. Experimental procedures and stimulation paradigmsAll 8 studies employed a randomized, double-blind, placebo-controlled design. Following screening and inclusion, participants were invited to one to four experimental sessions. tTIS was delivered by two independent DS5 isolated bipolar constant current stimulators (Digitimer Ltd, Welwyn Garden City, UK) and applied via surface electrodes (3 cm2) applying a low-intensity, sub-threshold protocol following the currently accepted cut-offs and safety guidelines for low-intensity transcranial electric stimulation in humans [10]. tTIS was applied as previously described [5, 6] (figure 1(B)). Different types of tTIS protocols were delivered by changing one of the two carrier frequencies, thereby modulating Δf and temporal interference exposure. Active tTIS consisted in either a continuous theta burst stimulation (cTBS, bursts of three pulses at 100 Hz delivered at 5 Hz, f1 = 2 kHz) or an intermittent theta burst stimulation (iTBS, bursts of 3 pulses at 100 Hz repeated at 5 Hz for 2 s, interspersed with 8 s without any temporal interference exposure [Δf = 0], f1 = 2 kHz). One experiment also included 20 or 80 Hz tTIS, with carrier frequencies centered on 2 kHz and equaling f1 = 1990 and 1960 Hz, respectively [5]. Finally, two different types of placebo stimulation were used, one HF control (f1 = 2 kHz, Δ f = 0) and one sham control (ramp-up [5 s] immediately followed by ramp-down [5 s] of the HF).
Two different tTIS montages were used, one targeting the striatum [5, 6] (F3-F4, TP7-TP8 in the 10–20 EEG system [14], 5 experiments, 167 sessions) and one targeting the left hippocampus (around the P8-CP7, Fp2-FT7 landmarks, see [7], 3 experiments, 90 sessions).
Safety was evaluated through self-reports of potential adverse events and number of drop-outs. Importantly, because many of the experiments involved multiple tTIS sessions and behavioral follow-ups, participants had multiple opportunities to report potentially lasting side effects. tTIS-related sensations were systematically evaluated in the beginning of each session after delivering 20 s of tTIS (including 5 s of ramp-up and 5 s of ramp-down). Different intensities were tested (0.5, 1, 1.5 and 2 mA per channel, baseline-to-peak) and participants were asked to rate the sensations between 0 (none), 1 (mild), 2 (moderate) or 3 (strong) and to give at least an adjective to describe it (free choice). For the analysis, we focused on the first adjective provided by the participant. At least one active and one placebo tTIS condition were tested in each session (figure 1(A)). Blinding efficiency was also evaluated after the experiment (i.e. after a longer exposure to tTIS at 2 mA), by asking the participants whether they believed they received 'Active' or 'Placebo' stimulation at each experimental block. Subjects were also allowed to not provide any guess by answering 'I do not know'.
2.3. Statistical analysesData and statistical analyses were carried out with R (R Core Team 2022, Vienna, Austria). Generalised Additive Models (GAM; Wood, 2011) were fitted using the gam function of the mgcv package, with the ordered categorical (ocat) family and no smooth function. As random effects, we added an intercept for participants and slopes for sessions per participant. We assessed model fit with deviance explained and normality of residuals. To evaluate equivalence between the magnitude of sensations elicited by active and placebo tTIS, we defined equivalence bounds as [−0.5, 0.5], considering that a difference of sensation lower than 0.5 on the sensation scale (ranging from 0 [none] to 3 [strong]) would be practically unimportant. We then computed the 90% confidence interval on the coefficient estimate associated to the type of tTIS (tTISTYPE: active or placebo) in the GAM and established equivalence if this interval was completely contained within the equivalence bounds, as recommended by the US Food and Drugs Administration [15–18].
For analyses of the guesses in the end of the experiment, we grouped participants who provided an incorrect guess and who did not guess ('I do not know') considering that both of these sub-groups could be considered as efficiently blinded. We compared the proportion of remaining subjects (the ones who correctly guessed the type of stimulation) to a theoretical chance level of 50% with a binomial test.
3.1. Safety and tolerability profilesNo adverse event was detected over the 119 participants and 257 sessions. Only one participant (TBI patient) dropped out because sensations were received as too strong and reminded the patient about the trauma. The stimulation was well tolerated in all the remaining experiments. tTIS at 2 mA (intensity used during the experiments and shown to induce neural and behavioral effects [5, 6]) was generally reported as 'mild' (mean sensation on scale from 0 [none] to 3 [strong] = 0.98) and was most often characterized as 'Tingling', 'Vibrating' or as a 'Pressure' (figure 1(C)). These results suggest that tTIS applied to target deep brain structures present a favorable safety and tolerability profile.
3.2. Blinding efficiency in healthy adultsWe evaluated blinding efficiency in healthy using two approaches. First, we asked if sensations were significantly different between active and placebo tTIS following a brief exposure to the 2 mA stimulation, in the beginning of each session (n = 227). We ran a GAM with tTISTYPE (active or placebo), AgeGROUP (young or older adults) and TargetTYPE (striatum or hippocampus) as fixed effects. Crucially, the magnitude of sensations did not significantly vary between active and placebo tTIS (χ2 = 0.41, p = 0.52), suggesting an inability to discriminate between tTISTYPE based on the elicited cutaneous sensation (figure 2(A)). Notably, the 90% confidence interval ([−0.20, 0.44]) for the tTISTYPE coefficient was fully included in the pre-defined equivalence bounds ([0.5, 0.5], see Methods), suggesting equivalence between the magnitude of sensations elicited by active and placebo tTIS [15, 16]. Additionally, we found that participants provided the same answer for active and placebo tTIS in a large proportion of the ratings (73.8%). Among the remaining ratings (26.2%), there was no substantial bias towards active or placebo tTIS (active tTIS-related sensations were rated as weaker or stronger than placebo in 43.75% and 56.25% of the cases, respectively, exact binomial test against 50%: p = 0.31). Interestingly, the GAM also revealed a significant AgeGROUP effect (χ2 = 9.19, p = 0.0024): older adults felt in general less sensations than young, as expected and previously described [19]. Finally, magnitude of sensations did not significantly vary between the striatal and hippocampal montages (χ2 = 1.15, p= 0.28). These results show that active and placebo deep tTIS elicit very similar magnitudes of sensations that are reduced with age.
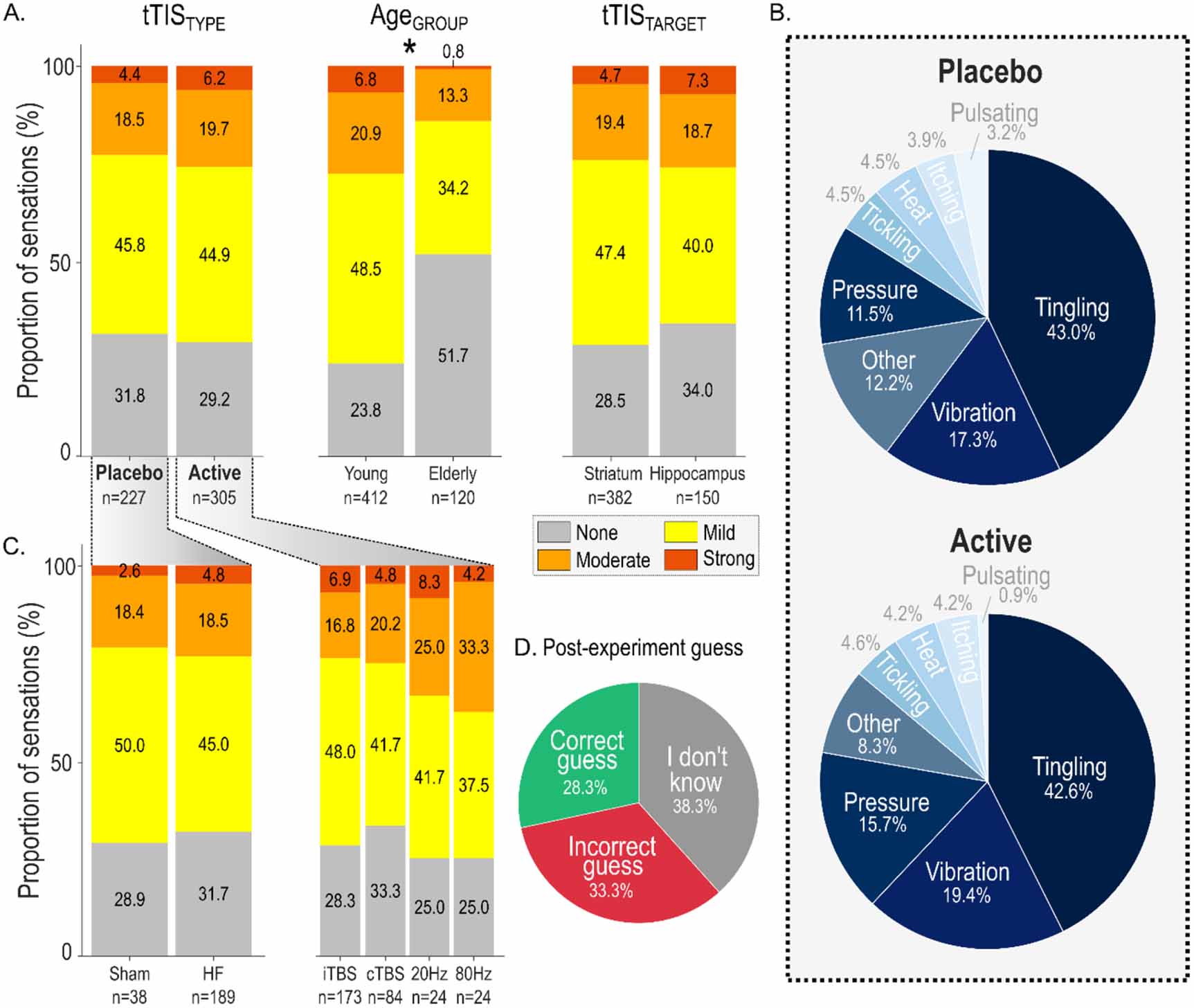
Figure 2. Blinding efficiency of deep tTIS in healthy adults. (A) Magnitude of sensations. Magnitude of sensations at 2 mA depending on the tTISTYPE (placebo or active, left), AgeGROUP (young or older, center) and tTISTARGET (striatum or hippocampus, right). The number of observations for each category is reported below the respective plots. Note that only AgeGROUP had a significant effect on the rating of sensations, as denoted by the star (p = 0.0024). (B) Type of sensations. Type of sensations as described by the participants for placebo (upper pie chart) and active (lower pie chart) tTIS. (C) Magnitude of sensations for subtypes of placebo and active tTIS. Secondary analysis comparing the sensations of different sub-types of placebo (sham and HF) and active tTIS (iTBS, cTBS, 20 Hz, 80 Hz). (D) Results of the post-experiment guess. Pie chart representing the proportion of participants who provided a correct, incorrect or no guess regarding the order of stimulation conditions (active/placebo) when asked after the end of the experiment.
Download figure:
Standard image High-resolution imageImportantly, beyond their magnitude, the type of sensations could also compromise blinding. Categories of sensations that were at least used in 2% of the observations were considered and the rest was collapsed under the category 'Other', leading to a total of 8 categories of sensations (figure 2(B)). Notably, their relative proportions were not different in the active and placebo tTIS conditions (Pearson's Chi-squared test: χ2 = 5.27, p= 0.63). Hence, the type of elicited sensations was not different between active and placebo tTIS.
As a secondary analysis, we asked if within each category of tTIS (active or placebo), different stimulation parameters led to different sensations. We re-ran the same statistical model separately for active (iTBS, cTBS, 20 Hz, 80 Hz) and placebo (HF and sham) tTIS. Again, there was no effect of tTISTYPE in any of the two models (active tTIS data: χ2 = 0.074, p = 0.99, placebo: χ2 = 2.16, p = 0.14, figure 2(C)). Hence, sensations elicited by tTIS did not depend on stimulation frequency or protocol, suggesting that these different active and placebo tTIS conditions can be compared without the risk of unblinding.
As a second evaluation of blinding, we asked if participants could guess in which session they received active or placebo tTIS after the main experiment. Here, for homogeneity, we included data from all experiments where participants had to guess the correct order between 2 types of tTIS experienced in separate days (n = 120 sessions, between 7 and 40 min of exposure to tTIS). Participants were not able to guess the correct order of the conditions above chance level (correct guess: 17/60 participants, incorrect guess or no guess: 43/60, figure 2(D)). These data confirm that participants could not distinguish between active and placebo tTIS, even after a longer exposure to the stimulation.
3.3. Blinding efficiency in TBI patientsAs a proof-of-concept for the use of tTIS in clinical populations, we asked if the same results could be obtained in TBI patients (n = 15, 2 sessions, iTBS vs HF, intensity =2 mA per channel, hippocampal montage). First, none of the TBI patients rated the sensation as 'strong', and the mean magnitude of sensations was 0.83 (scale from 0 [none] to 3 [strong]), suggesting very good tolerability. Then, consistent with the healthy data, the model did not reveal any difference between the active and placebo conditions (χ2 = 1.08, p = 0.30). Finally, TBI patients were not able to guess the correct order of stimulation above chance level (9/15 correct guesses, exact binomial test against 50%: p = 0.85). This constitutes preliminary evidence that tTIS is tolerable and compatible with blinding in patients.
In the present paper, we present first findings after more than 250 sessions of non-invasive deep brain stimulation by means of tTIS showing feasibility, favorable safety and tolerability profiles, and excellent blinding efficiency.
Sensations elicited by 2 mA tTIS were generally considered mild and were most often described as 'Tingling', 'Vibrating' or 'Pressure', in line with sensations elicited by cortical NIBS techniques such as tDCS or tACS [9–12, 20, 21]. These results also align well with previous applications of tACS over motor cortex in the kHz range [22, 23] (see also [24] for a safety assessment at 1 mA) and a recent study showing that 30 min of tTIS targeting motor cortex was safe and well tolerated based on multiple measurements including serum neuron specific enolase, temperature of skin-electrode interface, electro-encephalography and clinical scales (n = 38 healthy participants; [25]). Here, we extend these results to tTIS montages targeting deep brain regions [5–7] in a large dataset including older adults and TBI patients and further show that tTIS is compatible with efficient blinding. It is worth noting that our first experience based on self-reports and number of drop-outs suggest a favorable safety profile of tTIS applied to deep brain regions but that a more extensive evaluation of safety including blood samples, electrophysiology and structural imaging will be required to further establish the safety of tTIS.
Notably, in the present work, temporal interference was generated by applying two high frequency currents around 2 kHz, as initially done in rodents [3] and then further developed in humans to target superficial [25, 26] and more recently deep brain regions [5–7] Hence, though very likely [13], we cannot be completely sure to have identical safety, tolerability and blinding efficiency when using other kHz carrier frequencies. Yet, previous research applying for example tACS at 1, 2 or 5 kHz (at 1 mA) over the motor cortex in young healthy subjects report comparable safety, tolerability and blinding profiles [23, 24], suggesting that similar results could be obtained with other low-kHz carrier frequencies. Computational modelling also supports the idea that tTIS can be safely applied at 2 mA (and putatively up to 7 mA) for low-kHz carrier frequencies, while safety thresholds are yet to be established above 10 kHz [13]. Future research could aim at evaluating safety and sensations elicited by tTIS for a larger parameter space including more possible carrier frequencies and intensities.
As mentioned above, a critical aspect for NIBS is to make sure that sensations elicited by stimulation do not allow participants to discriminate active and placebo conditions [20]. Here, participants could not discriminate tTIS conditions neither when they were asked to describe the sensation immediately following short exposure to stimulation, nor when they had to guess the order of the conditions (active vs. placebo) after minutes of tTIS. Participants also reported similar sensations for the two different electrode montages (targeting striatum or hippocampus) and the different active (20 Hz, 80 Hz, iTBS, cTBS) or placebo (HF or sham) stimulations. We report an age-related decrease in the magnitude of tTIS-related sensations, which parallels the well-described decline in somatosensory function observed with ageing [27, 28]. Finally, beyond the case of one TBI participant who dropped-out because of sensations perceived as too strong, tTIS was generally well tolerated in TBI patients and compatible with successful blinding. Although the TBI cohort is small (15 patients), this constitutes promising evidence that tTIS is also feasible in clinical applications with good blinding and tolerability. Re-evaluation of safety, tolerability and blinding efficiency will be required on larger patient cohorts.
Another important line of research following this work could be to systematically compare the side-effects of tTIS with the ones of low-intensity transcranial ultrasound stimulation (tUS), another emerging deep NIBS approach [29, 30]. As such, when compared to classical tES, tUS induces less skin sensations but a higher rate of other symptoms such as sleepiness [31]. Another important difference between tUS and tTIS may concern the peripheral auditory stimulation arising from tUS which requires appropriate masking to ensure blinding efficiency and can complicate the interpretation of online effects [32]. Hence, future work comparing non-invasive deep brain stimulation techniques will have to not only confront their neuromodulatory effects, but also take into account their safety, tolerability and blinding efficiency profiles, in the view of future clinical translation [33, 34].
We acknowledge access to the MRI and Neuromodulation facilities of the Human Neuroscience Platform of the Fondation Campus Biotech Geneva and access to the Neuroimaging Facilities of the HVS, Sion. This work has received financial support by the Horizon Europe Research & Innovation Programme under Grant Agreement No. 101092612 (Social and hUman ceNtered XR—SUN project) to F H; by the Swiss National Science Foundation (SNSF, 320030L_197899, NiBS-iCog) to F H; the Defitech Foundation (NiN-Park, Morges, CH) to F H; the Bertarelli Foundation—Catalyst program (Gstaad, CH) to F H, M W; the Novartis Research Foundation—FreeNovation (Basel, CH) to M W; the Wyss Center for Bio and Neuroengineering to F H; the Interdisciplinary Center for Clinical Research (IZKF) at the University of Würzburg (Project number Z-3R/4) to M W; the Fund for Research training in Industry and Agriculture (FRIA/FNRS; FC29690) and Wallonie-Bruxelles International to P V; Personalized Health and Related Technologies (PHRT #2017-205)' of the ETH Domain to F H and the ERA-NET NEURON (The DiSCoVer project) to F H. The NEURON "Network of European Funding for Neuroscience Research" is established under the organisation of the ERA-NET 'European Research Area Networks' of the European Commission. National funding is the Swiss National Science Foundation (SNSF) for EPFL.
The data cannot be made publicly available upon publication because they contain sensitive personal information. The data that support the findings of this study are available upon reasonable request from the authors.
The authors declare no competing interests.
留言 (0)