
記住我



Study design and setting: prospective cohort study of COVID-19 ARF patients admitted to the Fernandez Hospital RICU from June 2020 to February 2021. Institutional review board reviewed the protocol and authorized prospective data collection (Code register: ID #2263).
Primary study endpoint was to identify LUS cutoff point for 90-days mortality. Secondary endpoints were to identify LUS cut-off point for HFNC failure identification and ETI indication. HFNC failure was defined as the need to switch to CPAP devices to maintain oxygenation. NIRS was performed under a strict protocol [16] that is available online as supplementary content, as well as statistical data analysis.
PatientsConsecutive COVID-19 ARF patients admitted to RICU were included. Patients with advance directives (do not intubate or do not resuscitate) and pregnant women were excluded. A 12 h HFNC trial at 60 L/min and FiO2 to maintain SpO2 between 92 and 96% was initiated if one of the following criteria was met: PaO2/FiO2 (P/F) ≤ 200, supplemental oxygen requirement ≥ 10 L/min, respiratory rate (RR) ≥ 30/min with or without accessory muscles usage (eFigure 1). Awake prone position was used as an adjuvant therapy. Patients were considered responsive if RR was < 30/min and SpO2 increased > 94% with FiO2 < 0.6% after the 12 h trial. In non-responders patients, NIRS was switched to CPAP.
ETI indication was performed if two of the following signs of ARF worsening were present: lack of improvement or worsening oxygenation, respiratory rate above 40/min, lack of improvement of signs of respiratory muscle fatigue, development of copious tracheal secretions, acidosis with a pH < 7.35, or intolerance to CPAP. The need for ETI was also established by the presence of one of the following criteria: hemodynamic instability (systolic blood pressure < 90 mmHg, mean blood pressure < 65 mmHg or requirement for vasopressor support), deterioration of neurologic status with a Glasgow Coma Scale below 12 points.
Data collectionAfter selection, informed consent was granted. The following variables were collected: age, sex, body mass index (BMI), comorbidities, SOFA(Sequential Organ Failure Assessment), APACHE II (Acute Physiology and Chronic Health Evaluation), NEWSII (National Early Warning), day of illness, P/F, ROX index (Respiratory rate-OXygenation) defined as the ratio of oxygen saturation (SpO2)/fraction of inspired oxygen (FiO2) to RR at different times (2, 6, 12, 24 and 48-h) and LUS at admission.
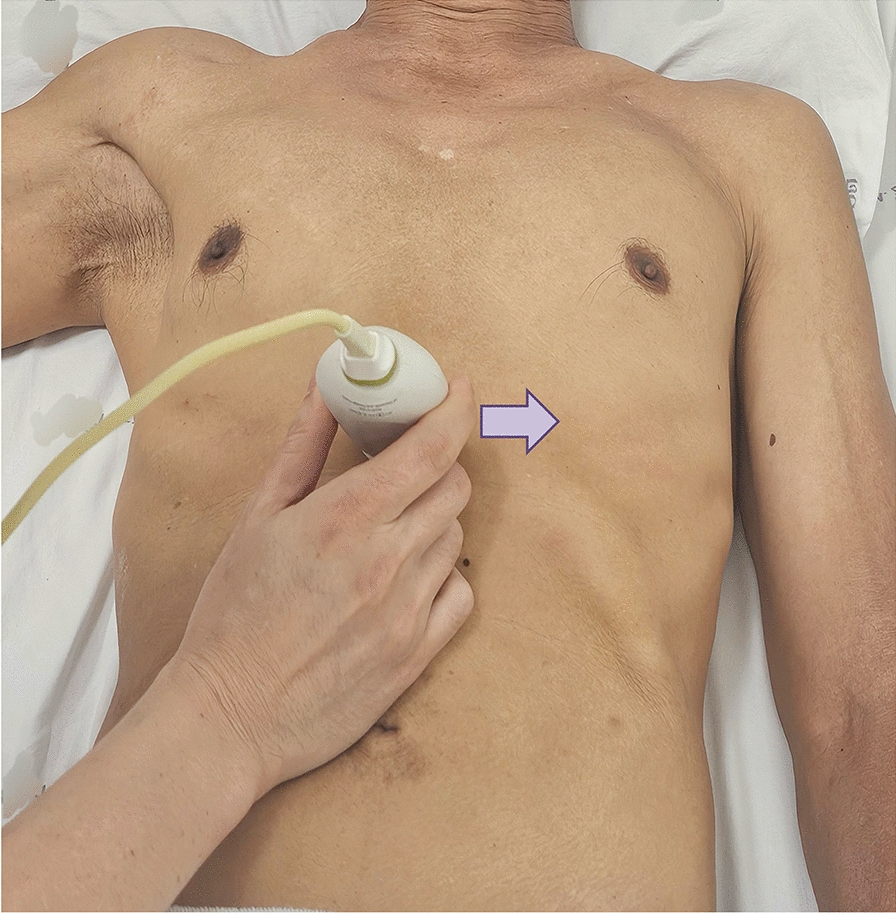
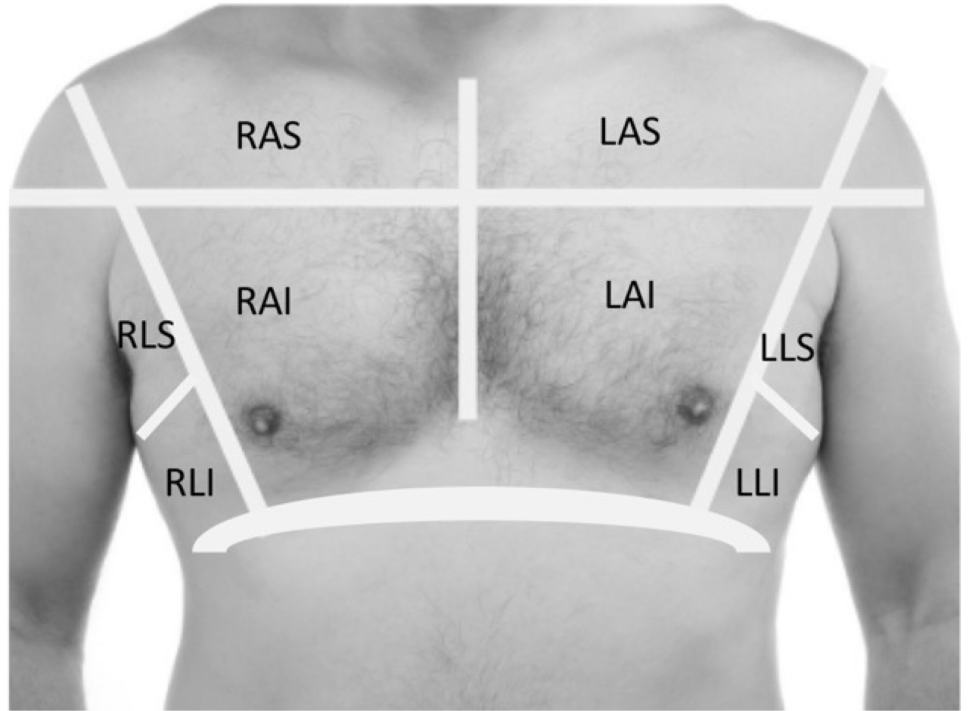
LUS protocolFour Respiratory Therapists certified in lung POCUS by the Argentinean Association of Kinesiology and trained in LUS for 2 months prior the study, performed all the ultrasound measurements within 24 h of RICU admission. The exploration was performed by dividing the thorax into 12 zones, delimited by the parasternal line, the anterior axillary line, the posterior axillary line and a paravertebral zone on each side. The upper and lower reference is given by the perpendicular line to the previous ones, at the level of the nipples. Exploration technique is developed in Fig. 1. A 3.5-5 Hz convex probe was used to explore the thorax, placing the focus at the level of the pleural line (2–4 cm) and setting a depth of 8 to 10 cm. A scan was performed in each of the 12 zones in the longitudinal plane and the pattern of least aeration present in each zone was assessed. In case of requiring a better ultrasonic window and/or a better evaluation of the area, the transducer was placed in the transverse plane.
Fig. 1
Region of interest for lung ultrasound score
A semi quantitative score ranging, running from 0 to 3, was performed according to lung ultrasound findings: 0 = normal A lines, 1 = multiple separated B lines, 2 = coalescing B lines or light beam, 3 = consolidation. The aeration score is built by the sum of all the areas, with a minimum of 0 and a maximum of 36 according to the aeration loss. The following ultrasound devices were used; Philips Lumify® ultrasound machine (Philips Medical Systems, Bothell, WA, USA) with a convex transducer, a Sonoscape S6® ultrasound machine (Yizhe building, Yuquan Road, Shenzhen, 518,051, China) and a Chison ECO 1® (No.9, Xinhuihuan Road, Xinwu District, Wuxi, Jiangsu, China 214,028) were used for the measurements.
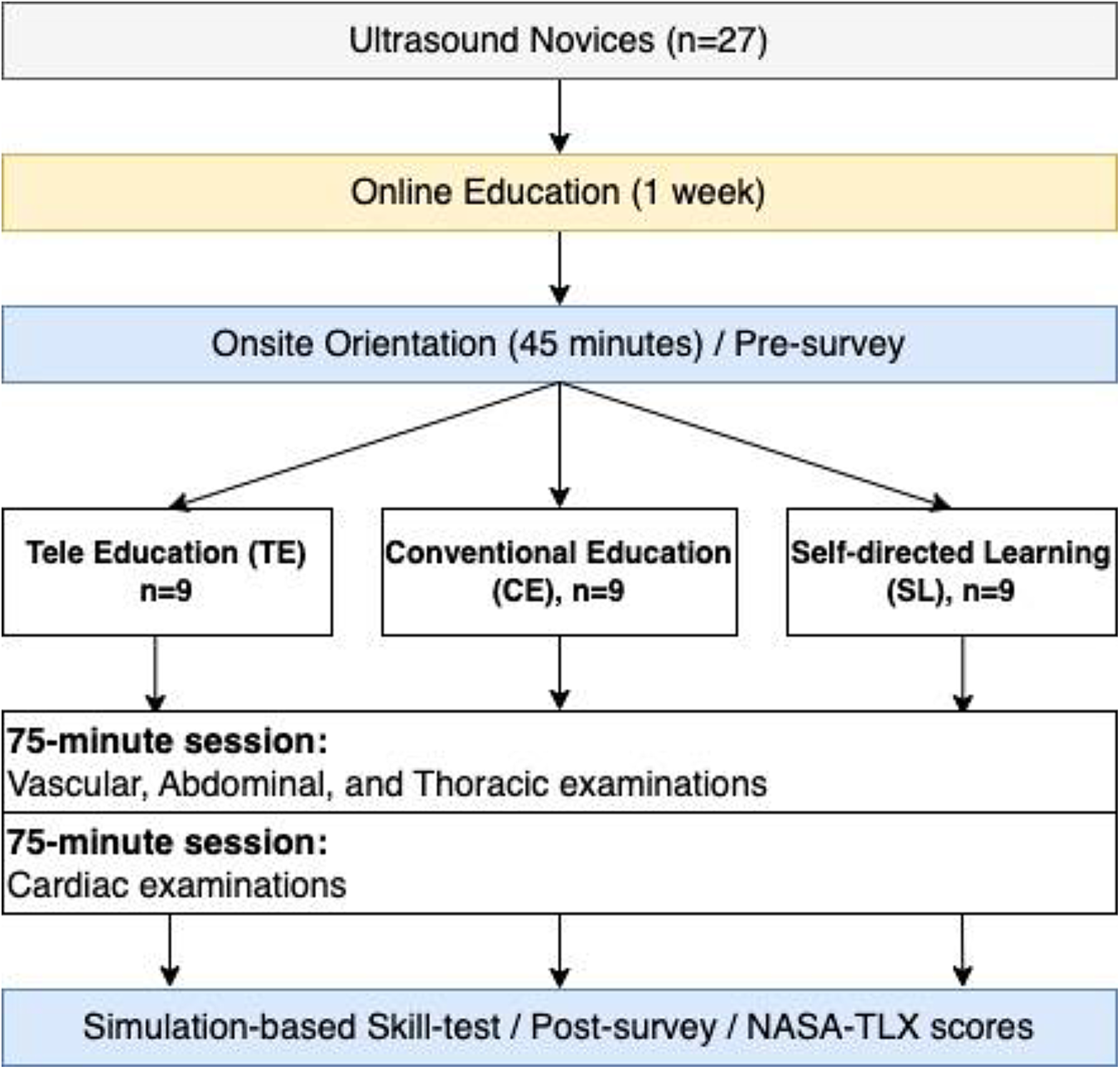
Statistical analysisSample size was not predetermined. Normality criteria was established by Schapiro Wilk test and according to it were presented as means ± standard deviations (± SD), medians and interquartile range (IQR). Categorical variables were presented as absolute values and percentages. Continuous variables were compared using the student’s t-test or the U-Mann Whitney test, as appropriate. For categorical variables, chi-square tests were used (Figure 2).
Fig. 2
Patients allocation to non-invasive respiratory support. ARF: Acute Respiratory Failure; COVID-19: Coronavirus disease 19; HFNC: High-Flow Nasal Cannula; CPAP: Continuous Positive Airway Pressure; LUS: Lung Ultrasound
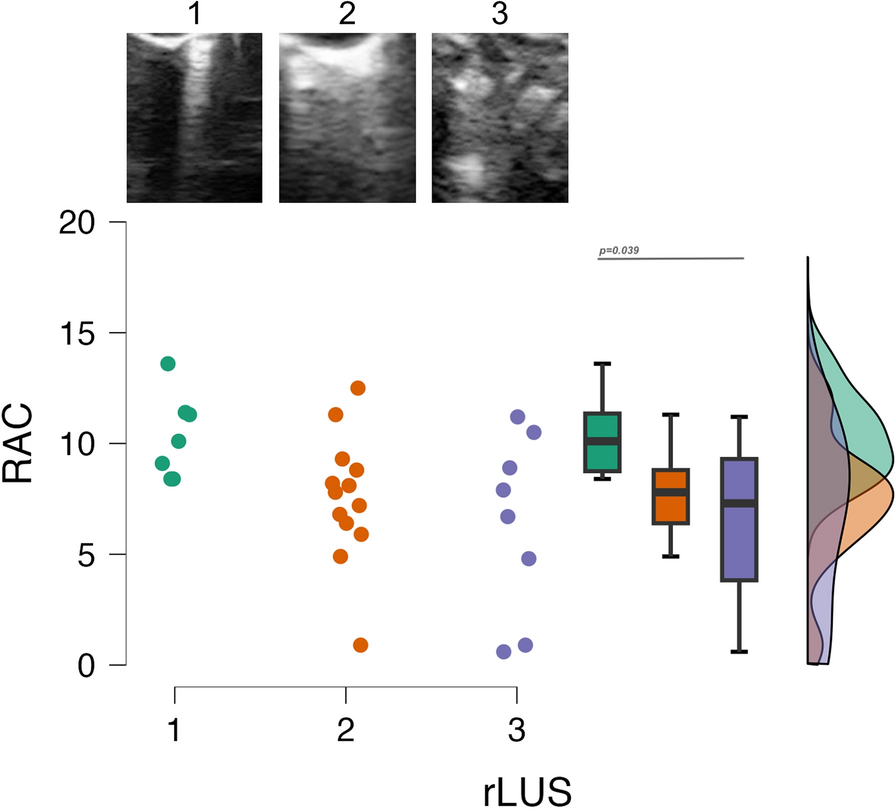
A Receiver Operating Characteristic (ROC) curve analysis was performed accorded to LUS findings on respect of primary and secondary outcomes. The area under the curve (AUC) was calculated to quantify the differences. LUS sensitivity and specificity were determined and the cut-off point corresponded to the maximum of the Youden’s index.
Kaplan-Meier curves were used for survival analysis and ETI incidence. In order to identify factors associated with the likelihood of in-hospital mortality, we fit a multivariable logistic regression model with mortality as the dependent variable. A priori selected variables were those considered of clinical relevance as well as variables that were significantly associated with the outcome in the bivariate analysis (at a p-value threshold of 0.2 or less). We report odds ratios (OR) with their associated 95% confidence intervals (CI). A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 26.0 (IBM Corporation, Armonk, NY, USA).
留言 (0)