
記住我
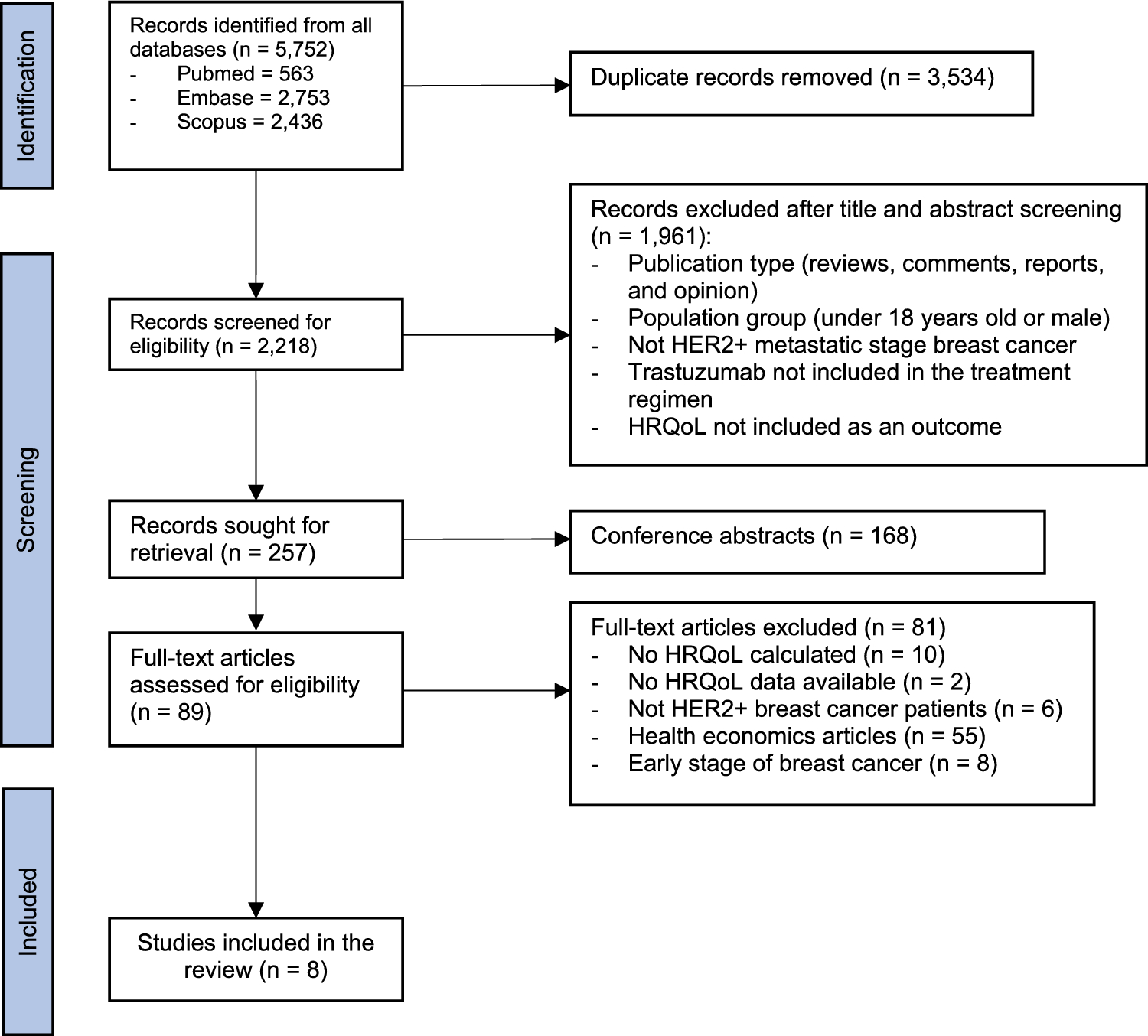

A flow diagram detailing the search is provided in Fig. 2. From 94 instruments identified in DIRUM and 1395 references identified in database searches, 49 instruments, and 77 references relating to 69 unique studies were included. From a grey literature search, 14 further documents/webpages were included for extraction of items related to social care, informal care and personal expenses. A broad range of conditions was covered (Table OR2, Online Resource). A total of 1619 items were extracted from the instruments, studies, documents and webpages. This number reduced to 723 following deduplication. Items were grouped on the basis of meaning, resulting in 203 items (e.g. care assistant, domiciliary care and care worker were grouped under home help/home care worker). The 203 items were grouped under the 13 categories listed in Table 1, which also shows the sectors each category is relevant to.
Fig. 2
Flow diagram of record identification to inclusion
3.2 Survey of People Working in Social CareBetween July and September 2021, 24 people working in adult social care responded to the survey. Respondents had a range of roles and varied with respect to years’ experience working in adult social care (Table OR3, Online Resource). Of respondents, 58% reported that no adult social care items were missing from the list and 75% reported that the items included would not be described as something different by people who use social care. In Table OR4 (Online Resource), missed items and alternative terminology are presented, along with information on what changes were made in response to the suggestions. There were several reasons that items were not added, including the item already being included in a more general format (e.g. the suggestion of ‘Independent Mental Capacity Advocate’ was considered to be included under ‘Advocate’) and suggested items being outside the scope of the social care module (e.g. health-related items). In response to feedback, ‘social prescriber’ was changed to ‘community navigator/link worker’.
3.3 Focus Group with Health EconomistsFrom NIHR reports, 80 health economists were identified, seven were invited to participate and three participated in the focus group. Four health economists with specific expertise in social or informal care were also invited, and two participated. Participants were based at five academic institutions in England, Scotland and Wales (Table OR5, Online Resource).
3.3.1 Prioritisation of Social Care ItemsOn the basis of independent ranking, categories that were considered most important for inclusion are presented in Table 2. For the social care module, ‘social care professionals’ was considered the most important category to collect. Participants prioritised ‘professionals’ because “staff is likely to be the highest single cost item that would be differentiating two interventions being assessed within a trial” (health economist (HE) 2)). For the category ‘social care professionals’, ‘home help or home care worker’ and ‘social worker’ were considered the most important items to include by most participants because “thinking about core items, if we have an intervention that has some kind of social care element to it, those are the most likely” (HE3). Many other items (such as ‘welfare rights officer’) were considered to be context dependent and too specific for a generic instrument. Participants suggested that ‘social workers’ could be combined with other similar roles “that develop the care plans for individuals” (HE4).
“...unless you were very interested in social work and care manager in that particular study, you could really combine social work with care manager, and possibly care coordinator together. Because they are doing the same job and they have just got different titles in local authorities.” (HE1)
Table 2 Consensus results: relative importance of categories for inclusion in the new modulesOwing to geographical variations in terminology for the same roles, there was concern that trial participants would not understand job titles. To resolve this, it was suggested that all potential job titles, or definitions for each role, should be included. For ‘home help’, ‘care assistant’ was suggested as preferable terminology (HE4).
‘Social care services’ were considered the second most important category to include. For this category, ‘respite services’ and ‘day care services’ rated most highly. Participants highlighted potential overlap with ‘social care professionals’, as the unit of measurement in the instrument could be the service (e.g. ‘home care’) or the provider (e.g. ‘care assistant’). HE4 suggested grouping ‘social care services’ into four categories: (i) ‘day services’ (e.g. ‘respite care’), (ii) “services that sit on the interface between health and social care” (e.g. ‘reablement services’), (iii) “technology and aids and adaptation services” and (iv) ‘prevention services’ (e.g. ‘self-help group’).
Items covering ‘housing and residential care’ were rated less important for a generic social care module. HE1 indicated that, dependent on the context, items covering residential care may be highly important if the interventions alter residential care utilisation, or not important at all if residential status does not alter. HE4 indicated that ‘residential care homes’ and ‘nursing homes’ should be captured separately owing to differences in services provided and costs.
‘Aids, equipment and home adaptations’ were considered the least important category to collect in the social care module. Reasons for this included “aids and equipment... never come out to any amount of money” (HE1), poor completion in previous studies (HE3), and “some really big-ticket items like lifts, stairlifts... will be tens of thousands... but often they are being paid for by the individual” (HE4). HE4 thought ‘aids and equipment’ and ‘home adaptations’ could be grouped together. HE1 thought a free-text question would not be appropriate; they suggested, instead, a table with categories. HE4 agreed and suggested a standard cost could be applied to most items rather than asking people to report expenditure.
3.3.2 Prioritisation of Informal Care ItemsFor the informal care module, ‘time spent caring’ was considered most important to collect. ‘Who provided the care (e.g., spouse)’ and ‘what care was provided’ were rated joint second most important. For ‘what care is provided’, ‘personal care’ was considered the most important item, followed by ‘help around the house’, ‘time spent supervising’ and ‘help outside the home’. Participants agreed that these could be labelled ‘personal care’, ‘domestic care’ and ‘supervisory care’. ‘Who provides the most care’, ‘carer’s main activity if not caring’ and ‘carer employment details’ were considered next most important.
For informal care, discussions centred on the importance of items with respect to the costing approach. For the proxy good costing method, ‘what caring is provided’ was considered important, alongside ‘time spent on the caring activity’, for sourcing appropriate unit costs, whereas for the opportunity cost method, ‘what activity is foregone’ is required.
“…it matters what activity they are doing if you are using a proxy good method... if they are doing nursing activity or housework, then you might end up costing in quite a different way… But if you are using the opportunity cost method you are more interested in what activity they have given up…” (HE5)
HE4 highlighted that the type of care often differs depending on the relationship of the informal carer and this is important for costing.
“…co-habiting, caring, spousal care tends to be quite different and often of a close, personal care nature, whereas people that live outside, children for example, tend to provide more instrumental activities like shopping and support…” (HE4)
The difficulty of answering questions on the amount of time spent on caring was highlighted. This included discussion around reporting of ‘supervising’ time, where the carer is present, but not directly providing care. HE3 reported that “some [trial participants] consistently report 24 hours, 24/7 because they are there all the time and obviously if there is an issue at night they would be there to sort things out, even though technically they are asleep”. HE4 mentioned that studies use “broad categories… rather than ask for specific hours”.
When considering what informal carer employment information to collect, ‘main occupation’ was rated second most important, to ‘time off work’, but HE1 said ‘main occupation’ would only be considered relevant if individualised wage rates were used, and not relevant if an average wage would be applied for costing. Other information that was rated less important included ‘given up work’, ‘changed working hours’ and ‘difficulty finding work’. The rationale for this included “you might get only one person in your trial sample that is out of a job” (HE1), “they tend to be one-offs” (HE4) and when deciding what to collect, you need to consider “to what extent might it drive cost differences, or resource use differences between two interventions” (HE5).
3.3.3 Prioritisation of Personal Expenses ItemsHE3 explained that, when selecting items to collect in economic evaluations and when ranking items, they considered “why would that [item] be different between the different arms?”. They ranked items lower if they did not think they would differ. ‘Housing and residential care’ was ranked the most important category, with ‘nursing and residential homes’ rated the most important item. This category was rated highly, as dependent on personal circumstances (i.e. whether or not the individual qualifies for government-funded care), it can make a “big difference” (HE4). ‘Care or care professionals’ were ranked the second most important category.
It became apparent during the focus group that some of the participants had ranked personal expenses items with a social care perspective in mind, which explains why care-related categories ranked so highly. Participants said they may have ranked items differently if they were not thinking of the social care perspective. ‘Aids and adaptations’ were ranked more highly for the personal expenses module than for the social care module. HE1 indicated that “they are more important [in the personal expenses module] because they are a cost to you”. They also mentioned that local authorities are likely to get a bulk order discount from suppliers, whereas individuals are likely to pay more.
It was clear from discussions that which personal expenses items to collect would be driven by context. HE2 stated that the list of personal expense items was comprehensive, but “to have a generic personal expenses category… that would simply be too long a list to include” in a concise instrument. Participants also indicated that double counting should be considered, as items can appear in multiple modules.
3.4 Focus Group with People Who Have Accessed Social Care ServicesFour people participated. Participant characteristics are presented in Table OR6 (Online Resource). Two participants provided informal care to a spouse, one participant received care for themselves, and one participant assisted a parent with accessing social care and also had experience working in social care.
Participants were initially asked about their understanding of social care and informal care. This highlighted mixed understanding.
“My view of informal care is basically you source your own people you need to assist you and you pay them. Social care, local authority, provide the people and pick up the tab. (Participant (P) 2, provides care for spouse)
“…informal care is unpaid care. So, that might be a family carer or it might be a neighbour or somebody who just helps you out. Whereas formal care is something that is paid for. And that might be by the local authority, or it might be by yourself, you may be funding it yourself.” (P4, provided care for mother, experience of social care in professional capacity)
The term ‘informal care’ was deemed problematic by some participants; P1 cared for their spouse, but did not consider themselves an informal carer “because it’s not ad hoc, it’s every day”. They described themselves as “an unpaid carer”. There were issues evident with the terms ‘care’ and ‘carer’, as individuals may be “resistant to care” (P4) or identify it as help, and care providers, such as P1, said they “struggle to identify as a carer, as it’s what you do in a relationship… you don’t actually think that what you're doing is care”.
“I think the word [care] itself sometimes is not very acceptable to people who are getting older. And if someone says to me, “P3, you need a carer,” I would say, “No, I don’t need a carer”. But if someone said to me, “I think maybe you need a bit of help with your shopping,” that would be a completely different answer that I would give.” (P3)
P3 thought “one way of determining whether a person is actually having care is how often they come”, with something on a frequent basis indicating care. Participants thought the activities that informal carers provide could be separated into ‘maintenance’ (e.g. property upkeep) and ‘personal care’ (e.g. washing hair). In the first focus group, HE4 indicated that informal carer tasks are dependent on their relationship to and whether they are living with the individual they care for. This was confirmed by P4, who was a carer for their mother; they took on administrative tasks, while P1, who cared for their spouse, provided more personal care.
“I just saw myself as somebody who sorted things out really, which was very different to being a carer. I wouldn’t say I had that direct caring role.” (P4)
“You're making meals, cutting meals up, doing drinks, catheters.” (P1)
For time spent caring, P4 thought that informal care time is “not easy to quantify at all”. P2 described doing “17, 18 hour days”, while time spent away from caring “varies from day to day, and you snatch these moments [to do non-caring activities]”. P1 said they like to paint, but they had a monitor, so they could attend to their spouse when needed, indicating that, while they were not directly caring at that time, they were still on-call.
Participants were also asked about their understanding of different job roles in social care. Social workers were understood to “assess what is required… assess affordability” (P2), “conduct a carer’s assessment” (P1) and arrange care. Most participants named social workers as the professional that organises care, with one participant also indicating they had an occupational therapist assessor (P1). P4 said that their relative saw a range of people but would identify them all as a social worker.
“He had a social worker… he also had a care coordinator from the GP practice, he had another care coordinator, or a link worker or something like that, from a voluntary sector organisation, he had a coordinator from the council, and he had somebody who called herself a coordinator from a care company, that was providing his direct care. And he would have called all of those people his social worker.” (P4)
‘Care assistant’ was considered ambiguous by P3.
“Somebody comes and helps me wash my hair. Now, I don’t actually call her a care assistant.” (P3)
Participants indicated that it can be difficult to distinguish what is paid for by government and what they pay for themselves, as social care can be arranged via the council but paid for personally.
“I get an attendance allowance. And that pays for all sorts of things which I need. And I wouldn’t know whether that was the council paying for my care or me looking after it really.” (P3)
Participants also mentioned that some care is provided by the “voluntary sector” (P4), and care by charities can be paid for personally.
“We’ve got Age UK coming in… that is also paid for… they’ll do some mobility exercises with him, they’ll bring iPads and take him on city tours, and things like that. They don’t do personal care… But that, I organised myself.” (P1)
When asked about the main things they had paid for, P2 indicated they had paid for an expensive chair, but social services had provided a walking frame. P1 said they had bought lots of things but “none of them are expensive, but they add up”. P1 thought they could “roughly” and P2 thought they could “pretty accurately” recall how much they had spent.
3.5 Formulation of Draft ModulesFour health economists responded to the survey outlining the initial design of the modules. Most agreed with the items selected for the modules. There was one comment where, dependent on context, the participant advocated for ‘day care’ to be prioritised for inclusion in the social care module over ‘food at home’, as it is more of a core service.
On the basis of feedback from both focus groups, for the social care module, questions were included on ‘care assistant for personal care’, ‘someone who organises care’, ‘support activities (e.g. self-help group)’ and ‘group activities (e.g. day care)’. The informal care module included questions on ‘relationship to care recipient’, ‘time spent caring’ and ‘cohabiting’. Optional questions were drafted on ‘occupation of carer’ and ‘time spent caring by caring activity’. It was clear that a core list of items to collect in a personal expenses module was not appropriate, as what is important is context dependent. Aids and adaptations were indicated as costly expenses for individuals, therefore the focus of the third module was narrowed to aids and adaptations. Collecting data on aids and adaptations can be problematic as it can be funded by the government or the individual themselves, therefore the draft module allows respondents to categorise both the type of aid/adaptation (from cheap to expensive) and the source of funding for each aid/adaptation. The draft modules are provided in the Online Resource (Fig. OR3).
留言 (0)