
記住我
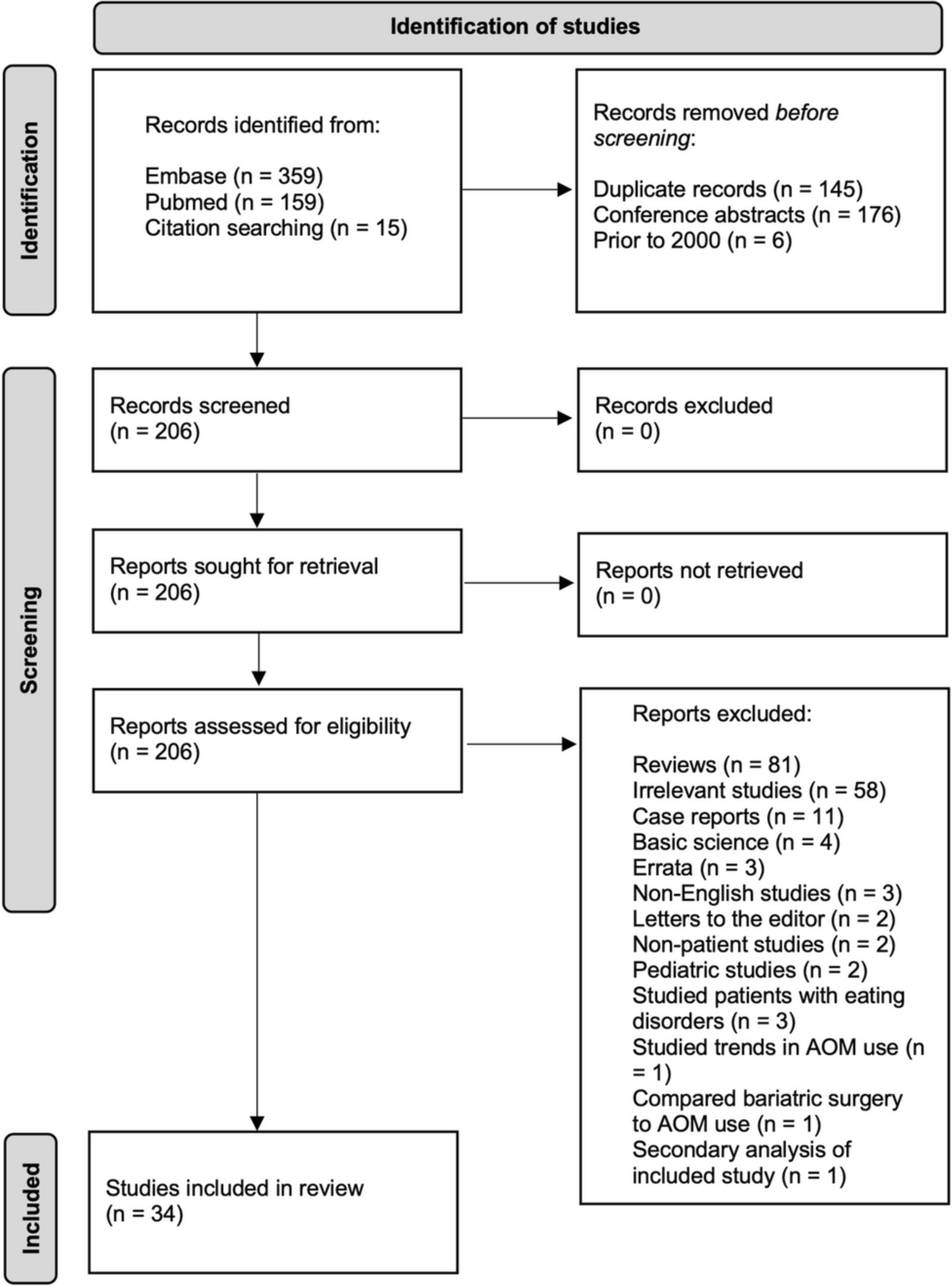
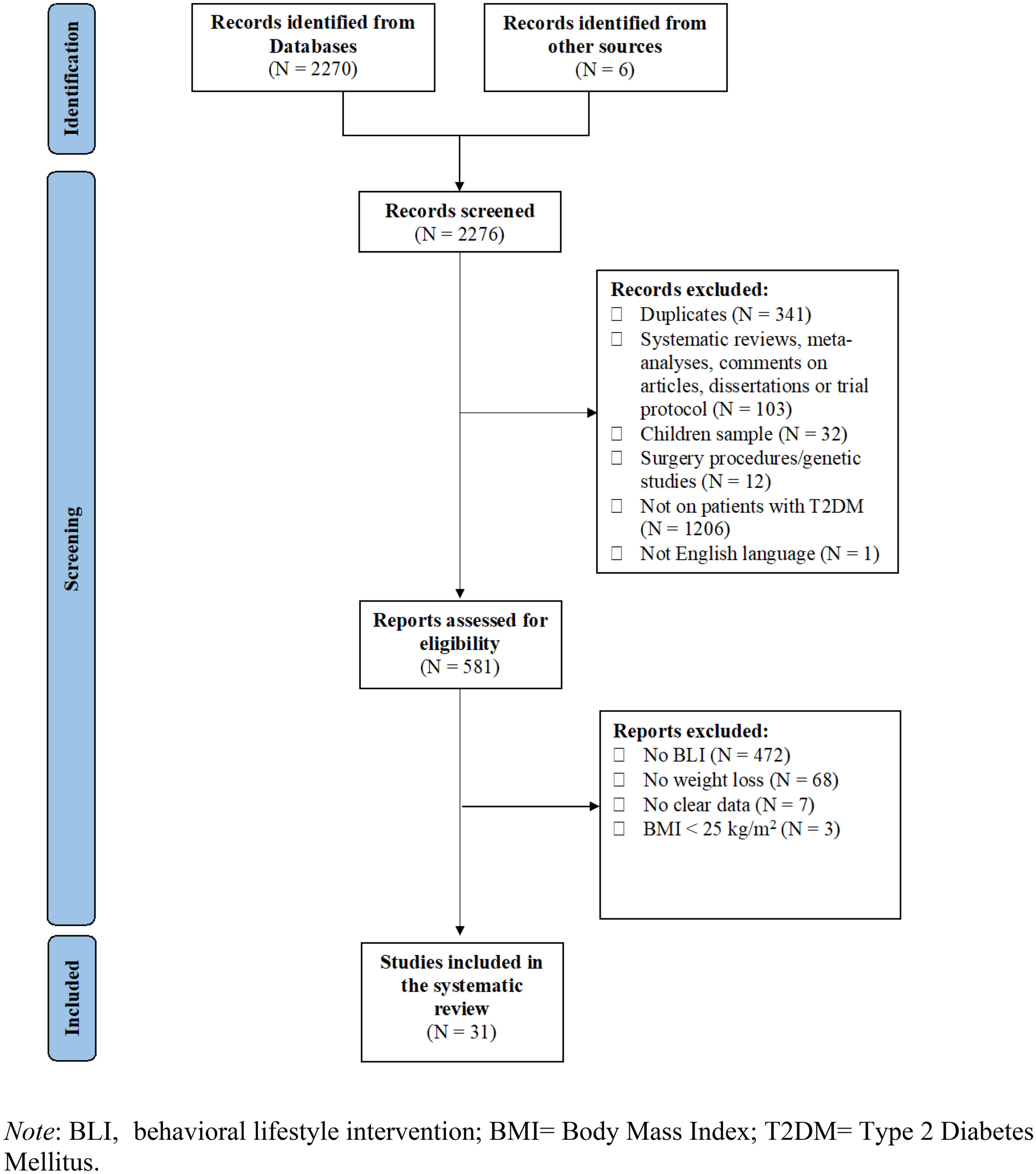
At the end of the screening process, 31 studies, which reported a total of 42 behavioral lifestyle interventions, were included in the review (see Fig. 1 for a detailed description of the study selection process). The main findings of the present systematic review are summarized in Fig. 2.
Fig. 1
PRISMA flow chart of study selection
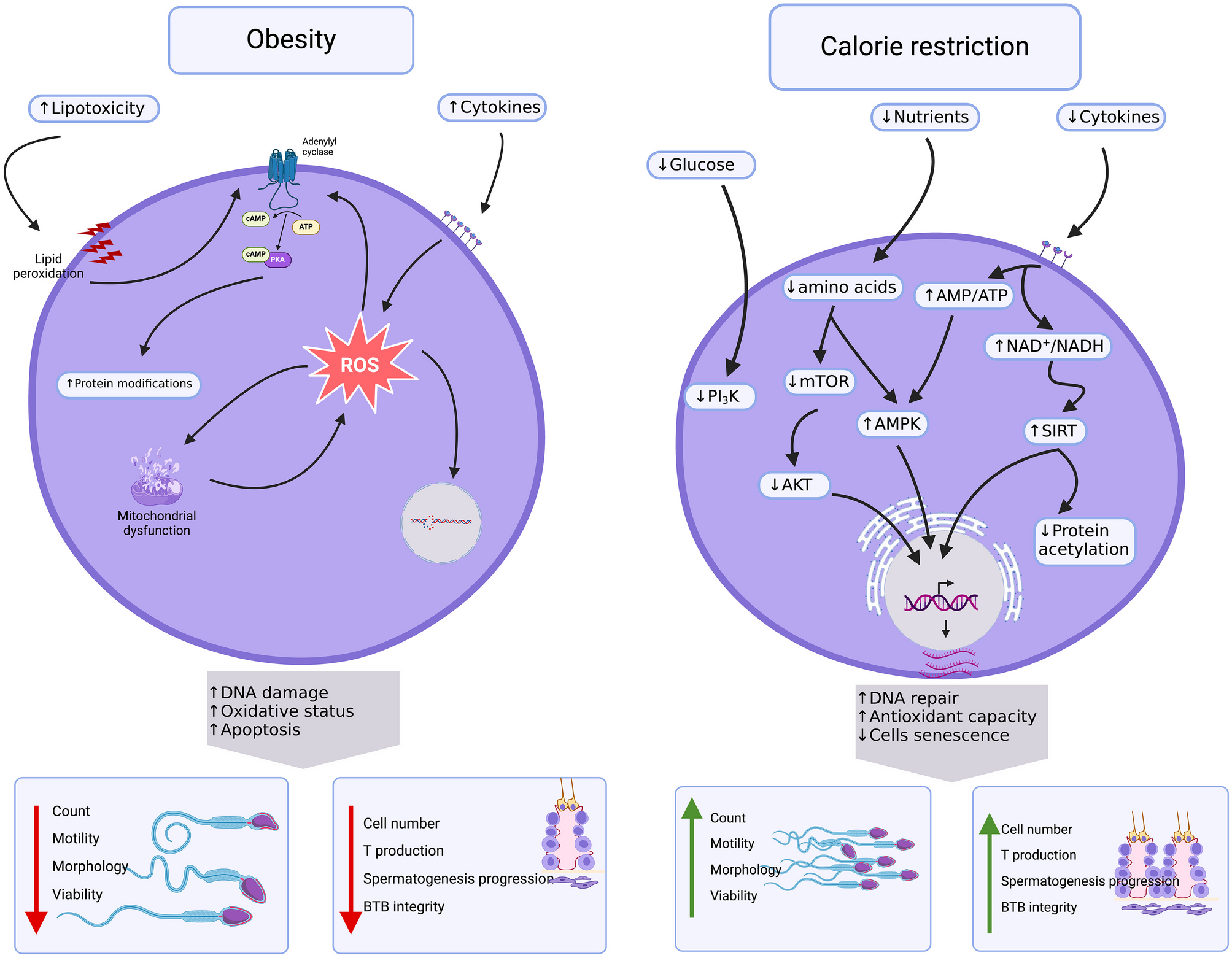
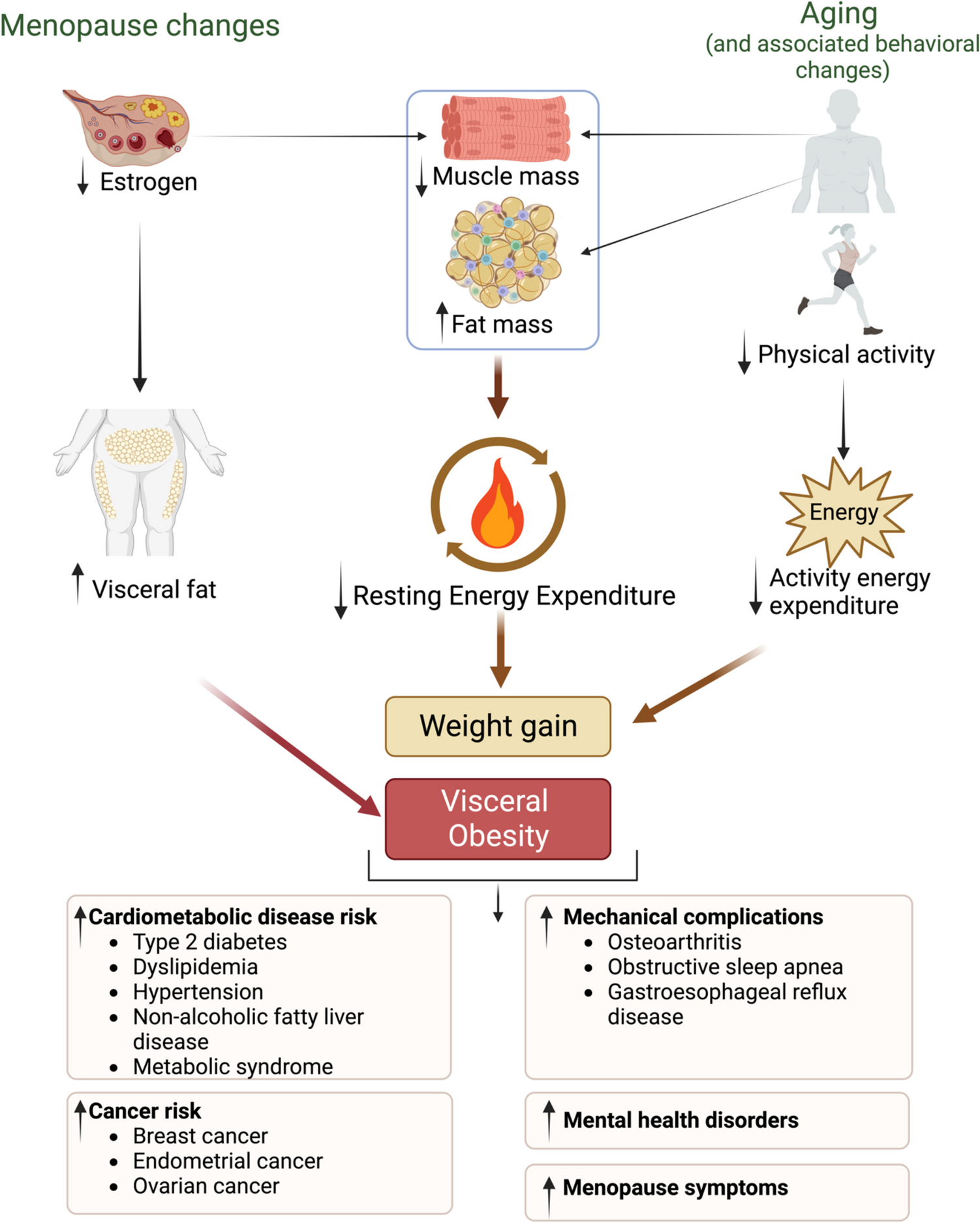
Fig. 2
Synopsis of main findings of the present systematic review
Characteristics of the StudiesThe included studies were published between 2013 and 2023 (Tables S2 and S3). All studies were randomized controlled trials (RCTs). Among the RCTs identified, three were feasibility trials [29, 30, 31•] and three pilot studies [32,33,34]. Most studies adopted a two-group design, except for 4 studies, which adopted a three-group design [29, 30, 33, 34].
Four additional studies compared “device-based” behavioral lifestyle interventions to educational interventions [29, 30, 35•, 36]. Ten studies [37,38,39,40,41,42,43, 44••, 45, 46] belonged to the Look AHEAD trial. Besides the Look AHEAD trial, seven additional studies compared a behavioral lifestyle intervention vs. usual care control group [31•, 33, 34, 47,48,49, 50••, 51, ] and a no-treatment control group [52]. Five studies compared interventions consisting of different behavioral techniques associated with specific diets [32, 53,54,55,56,57, 58••], and 2 studies compared behavioral lifestyle intervention vs usual care in subgroups of ethnic minorities [36, 38].
Studies included a follow-up evaluation ranging from 1 month to almost 10 years after the end of the intervention. Excluding the Look AHEAD studies [38,39,40,41,42,43, 44••, 45, 46], which included the longest follow-ups, other research involved follow-up of 1 month [36], 6 months [29, 31•, 35•, 49], 12 months [31•, 47, 48], and 48 months [48].
Characteristics of the SampleThe 31 studies included a total of 7272 participants, of whom 5145 were part of the Look AHEAD study. The sample size ranged from 26 to 5145. The mean age of the sample ranged from 36.5 to 69 years at baseline (Tables S2 and S3). Excluding a single study in which the sample was exclusively represented by women [36], the percentage of women in the remaining studies ranged from 34 to 75%. The mean BMI ranged from 31.6 to 38.1.
In 8 studies [35•, 39, 40, 42, 43, 45, 48, 50••], the sample reported having comorbidities with other medical conditions, such as chronic kidney disease [35•], obstructive sleep apnea [48], and cardiovascular disease [39, 40, 42, 43, 45, 50••]. More specifically, the sample in the study of Delahanty et al. [50••] reported the presence of other medical conditions, such as hypertension, hyperlipidemia, retinopathy, neuropathy, proteinuria, coronary artery disease, and congestive heart failure.
In 6 studies [40, 42, 47, 54, 56, 57], participants reported using pharmacological management, specifically they reported taking metformin [54], sulphonylureas [54], GLP-1 agonists [54], DPP-4 inhibitors [54], lipid lowering medication [54], antihypertensive medication [54], ACE inhibitor [56], angiotensin receptor blocker [56], diuretic [56], calcium-channel blocker [56], statin [56], antiplatelet drug [56], oral antidiabetic [57], antihyperglycemic medicines [47], oral hypoglycemic medication [40], and cholesterol medication [42].
Behavioral Lifestyle Intervention DesignOverall, 42 behavioral lifestyle interventions were identified among the 31 studies (Tables S1 and S3).
Even if all studies included behavioral components in association with diet and/or physical activity, the interventions were heterogeneous in the duration, frequency of contacts, staff, techniques, and type of intervention. Interventions’ duration ranged from 9 weeks to 5 years, with daily, weekly, bi-weekly, and/or monthly contacts. In most interventions, the frequency of contacts tended to be more intense at the beginning of the program and then diminished over time.
Additionally, eleven studies [30, 38,39,40,41,42,43, 44••, 45, 53, 54] included the evaluation of a maintenance phase, in which the longest phase lasted 12 weeks after the end of an intensive phase. The maintenance phase was meant to assess the preservation and consolidation of the achieved results.
Most interventions were performed by dieticians and exercise trainers. Other interventionists included physicians, nurses, physical therapists, physiologists, clinical psychologists, social workers, diabetes educators, and trained research staff. Sessions were generally delivered in-person and could be individual sessions, group sessions, or a combination of both.
There were 10 studies belonging to a major clinical trial, the Look AHEAD trial [37,38,39,40,41,42,43, 44••, 45, 46] which is a multicentric RCT on adults with T2DM and overweight/obesity (BMI ≥ 25, or BMI ≥ 27 if taking insulin therapy), which compared an intensive lifestyle intervention (ILI) to achieve weight loss through caloric restriction and physical activity, with a Diabetes Support and Education (DSE) group. The study began in 2001 and included over 5000 participants (2570 in the ILI group and 2575 in the DSE group). The interventions phase lasted 4 years. Outcomes were assessed once/twice a year, from baseline up to 9.6 years (median) of follow-up.
Behavioral ComponentA variety of different behavioral techniques, proposed by Michie’s taxonomy [27], were used in the behavioral lifestyle interventions included in the current work, and the most used taxonomy groups of interventions were goals and planning, feedback and monitoring, social support, shaping knowledge, natural consequences, and repetition and substitution. Specifically, the goals and planning taxonomy group was the most frequent behavioral protocols in the studies and mainly provided a description of objectives in terms of the behaviors to be implemented, the results to be achieved, the review of these objectives, problem solving, and a detailed description of the performance of the behavior. In the taxonomy group feedback and monitoring, the characterizing techniques were monitoring and/or self-monitoring of behaviors and reached goals, and biofeedback. Social support mainly comprised general support and, to a lesser extent, emotional support. With respect to shaping knowledge group, all the participants in the studies were given instructions on how to perform the behavior relating to diet, physical activity, and lifestyle. Considering natural consequences category, ingredients focused on education about health consequences of desired behaviors, also using specific methods to highlight the consequences of the performance of behavior in order to make it more memorable and, to a lesser extent, is given space to the identification and monitoring of emotional consequences. Finally, considering the group repetition and substitution, in all the considered studies the repetitive practice of one behavior was solicited in order to form new habits and replace old less or non-functional ones (Table S1).
Counseling meetings were intended to increase motivation and offer general support in making lifestyle changes, both during the intervention and follow-ups, when this was the case [30, 34, 48]. Educational meetings included diet, weight, and diabetes self-management education. Most interventions incorporated cognitive-behavioral therapy strategies for diabetes management and weight loss, including self-monitoring and/or monitoring by others (e.g., dietician) of weight, dietary and calorie intake, blood glucose, and adherence; goal setting; problem solving; and homework assignments.
Diet ComponentGeneral diet recommendations were provided in 23 studies [29, 30, 33, 34, 35•, 36,37,38,39,40,41,42,43, 44••, 45, 47,48,49, 50••, 51, 52, 59], while more specific diet instructions were provided in 7 studies [32, 46, 53,54,55,56,57]. These latter included calorie restriction and/or management of macronutrients intake, such as carbohydrates, proteins, fibers, and fats (saturated and unsaturated). Furthermore, 7 studies used meal replacement [30, 34, 41, 43, 45, 48, 50••].
Specifically, Carter et al. [53] compared a 500–600 kcal/day diet for 2 days/week and the usual diet for 5 days/week to a continuous 1200–1500 kcal/day diet. Watson et al. [54] compared a higher protein diet with a higher carbohydrate diet. Both diets were followed by a 12-week eucaloric maintenance phase. Otten et al. [55, 56] and Stomby et al. [58••] tested the efficacy of a Paleolithic diet alone (PD) or associated with a supervised exercise intervention (PDEX). The Paleolithic diet is a type of diet that excludes the intake of diary food, salt, refined sugar, and grains and simultaneously increases the intake of vegetables, lean meat fish, and nuts [60]. Ziegler et al. [32] compared the efficacy of a diet high in cereal fiber, free of red meat, and high in coffee versus a diet low in fiber, high in red meat, and coffee. Goday et al. [57] compared a ketogenic diet and a very low-calorie diet (VLCK) with a standard low-calorie diet.
Physical Activity ComponentA physical activity component was present in all 31 behavioral lifestyle interventions (Tables S2 and S3): 11 studies encouraged physical activity without any specific instruction [29, 30, 32,33,34, 36, 50••, 51, 53, 57, 59], while 20 studies provided clear indications on the type, intensity, duration, and/or frequency of physical activity [35•, 37, 39,40,41,42,43, 44••, 45,46,47,48,49, 52, 54,55,56, 58••, 59]. The intensity of physical activity varied from low intensity walk [38, 43, 45, 48, 49, 51, 58••] to moderately intense activity [35•, 39,40,41,42, 44••, 46, 47,
留言 (0)