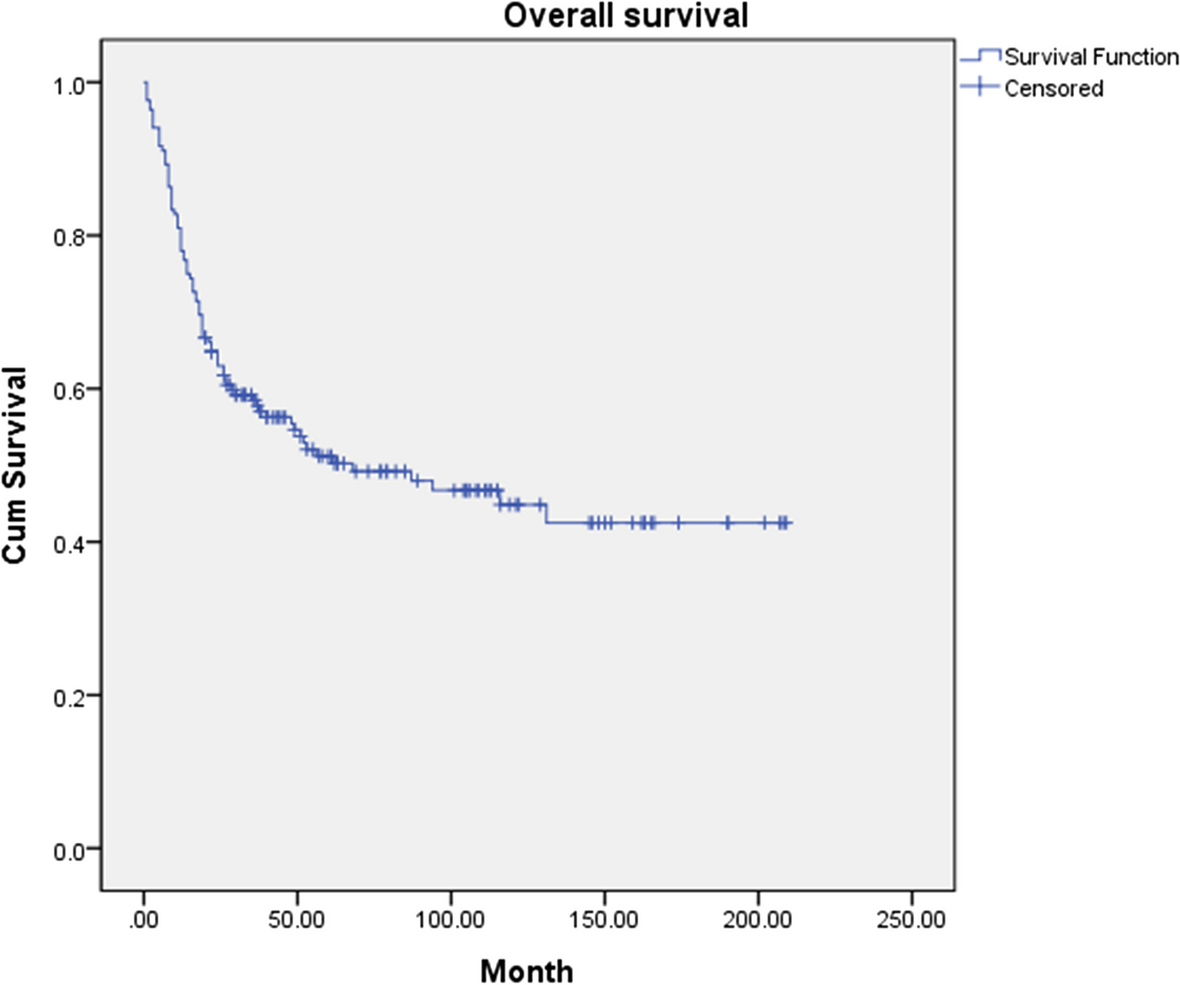
The study was planned in 2006, and there were no patients dropped out. In several recent studies, the 5-year survival rate was 47 to 71% [4,5,6,7,8]. However, most institutions showed survival rates lower than 60% [9]. In comparison, the 5-year cumulative OS and DSS in our study were 51.2% and 59.2%, retrospectively, which were quite favorable comparable results.
In multivariable analysis, the independent predictors statistically selected for DSS were recurrence and pTNM stage (p < 0.001 and hazard ratio = 8.09 and p = 0.002 and hazard ratio = 5.08) (Table 2). Specifically, considering that the most of patients who died of OSCC had recurrence (95.6%), recurrence is a significant prognostic factor. Even if the tumor recurs and the patient undergoes salvage surgery, a recurrent tumor grows deeper within the primary site or in the cervical region, and it often positions itself in a location that is hard to excise. These poor situations result in the difficulties of achieving complete resection due to the surrounding anatomical structures [6]. These difficulties result in an increased incidence of postoperative complications, such as aspiration pneumonia due to bleeding and airway obstruction. After salvage surgery, or if salvage surgery is not feasible, patients die due to general weakness and increased comorbidities resulting from malnutrition and cachexia. Additionally, patients died due to pneumonia induced by respiratory depression resulting from the use of opioids for pain management. However, recurrence is a result that occurs after surgery, it is difficult to predict recurrence in advance. In contrast, the pTNM stage can be predicted from the cTNM stage, and additionally, surgery, radiation therapy, and chemotherapy can be administered accordingly. Therefore, the pTNM stage is also an important prognostic factor in planning surgery and management. The pTNM stage has correlations with recurrence (r = 4.463, p < 0.001) (Table 3), and is a comprehensive factor that includes tumor size, invasion, and neck metastasis. these factors are more likely to contribute to the difficulties of achieving a clear resection margin and the formation of tumor budding and tumor cell nests. These increased postoperative complications, patient comorbidities, and tumor recurrence, ultimately result in a decreased patient’s survival rate.
In univariable analysis, neck metastasis, depth of invasion, cell differentiation, lymphovascular invasion, and postoperative radiotherapy were also statistically significant prognostic factors (Table 1). Particularly, neck metastasis and depth of invasion were well-known prognostic factors in the previous study [13, 14, 17, 25,26,27], and were included in the criteria for determining pTNM stage. This demonstrates the statistically significant correlation with the pTNM stage. (neck metastasis r = 0.518, p < 0.001, depth of invasion: r = 0.562, p < 0.001) (Table 3). The neck node metastasis and depth of invasion are indicators of an OSCC’s ability to metastasize, invasion section margin, and the formation of tumor budding and tumor cell nests [28]. These increased tumor recurrence, ultimately result in a decreased patient survival rate. This demonstrates the statistically significant correlation with recurrence (neck metastasis r = 0.373, p < 0.001, depth of invasion: r = 0.307, p < 0.001). Cell differentiation was also a well-known prognostic factor. However, it was not included in the criteria for determining TNM stage [29, 30]. This demonstrates no statistically significant correlation with the pTNM stage (p = 0.114). But, poorly differentiated tumors were associated with a recurrence (r = 0.162, p = 0.036), resulting in a decreased survival rate. Postoperative radiotherapy was also found to have statistical significance in relation to DSS. The indications for postoperative radiotherapy: positive neck metastasis, poor histologic factors, and large primary cancers are already crucial prognostic factors for survival rate [24]. This demonstrates the statistically significant correlation with recurrence, pTNM stage, neck metastasis, depth of invasion, and differentiation. These correlations result in a decreased survival rate. Lymphovascular invasion was also found to have statistical significance in relation to DSS. It would seem reasonable that the presence of the lymphovascular invasion at the primary site would predict neck metastasis since the invasion of lymphatic is the initial step in forming a metastasis [31, 32]. Considering neck metastasis as a critical prognostic factor, these correlations result in a decreased survival rate. This demonstrates the statistically significant correlation with neck metastasis in Table 3 (neck metastasis r = 0.211, p = 0.006).
In this study, patient factors such as age, sex, smoking status, and alcohol habits were found not to have a statistically significant impact on survival. Young age (< 50) represented higher DSS than older age (≥ 50), but there were no statistically significant. Similar studies focusing on age groups emphasized results where older patients had a lower survival rate compared to younger patients [33, 34]. And according to previous research, smoking and alcohol habits are recognized as primary risk factors for OSCC [35]. But it’s notably observed that the most of smokers and drinkers are men, while about one-third of the women (male:female = 112:56) in this study do almost not smoke or drink alcohol. Women, in previous studies, have been reported to have lower survival rates compared to men, also in the present study [27, 36] The patient factors, that exhibited conflicting and complex interrelationships, proved challenging to establish statistical significance. But above all, there are stronger factors (recurrence, pTNM stages etc.) that affect survival, and make the other factors less apparent in the statistical significance. There were controversies regarding whether surgical sites are a prognostic factor for survival or not, as cervical metastasis and bone and muscle invasion may manifest differently depending on the sites [21, 22, 37, 38]. This can be overcome by surgically removing the tumor and lymph nodes with a sufficient margin. therefore, it did not have a significant impact on the survival rate in this study. In this study, neck dissection included elective neck dissection (n = 20) and therapeutic neck dissection (n = 90). Among the total cN0 cases (n = 78), lymph node recurrence (n = 11) was 14.1%, and total lymph node recurrence (n = 26) was 15.5%. These were comparable to findings in previous studies [39, 40]. Therefore, it can be seen that all types of neck dissection were conducted well with almost no neck failure. However, neck dissection did not yield statistically significant results in this study. Since this study was not designed to randomize patients and evaluate differences in survival based on neck dissection or its absence, and elective neck dissection or therapeutic neck dissection, it would be hard to evaluate whether neck dissection and elective neck dissection or therapeutic neck dissection has a relation to survival or not.
The novelty of this study lies in the fact that it was conducted by a single surgeon within a single institution. In this study, we adjusted factors related to the surgeon, oncologist, and radiation oncologist that may affect the survival of patients with oral squamous cell carcinoma (OSCC). Additionally, our results were consistent with those of previous studies [6, 9, 13, 19, 20]. However, the limitations of the study include a relatively modest sample size and a retrospective study design. It will be necessary to address this limitation by supplementing it with more accumulated clinical case reports in the future.




留言 (0)