
記住我
KEY POINTS With the advantage of continuous visualisation of airway anatomy, video double-lumen tubes (VDLTs) are increasingly used for lung isolation. The VDLT can make intubation more accurate and may reduce the risk of airway injury, but because of the installation of cameras, the outer diameter of the VDLT is thicker than that of the corresponding part of the double-lumen tube (DLT) of the same size, which increases the risk of airway injury. Few studies have investigated the intubation complications associated with VDLT from the perspective of airway injury. We found that there was no statistically significant difference in the incidence of moderate-to-severe tracheal injury and vocal cord injury between DLTs and VDLTs. While improving the first-attempt success rate, intubation with VDLT increased the incidence of postoperative 24 h sore throat and hoarseness.
IntroductionTracheal injuries, vocal cord injuries, sore throat and hoarseness are common complications of tracheal intubation that affect the postoperative recovery of patients and reduce their postoperative satisfaction.1–4 Double-lumen tubes (DLTs) have the advantages of a relatively stable tube position and a great effect on lung collapse, and are often used for lung isolation under thoracic anaesthesia.5 However, compared with single-lumen tubes, the DLT is made of more rigid material and has a large outer diameter and airway injuries were more obvious when DLT was used for lung isolation, and the incidence of sore throat and hoarseness after surgery was higher.6–8 Therefore, more attention should be given to intubation complications caused by DLTs.
With the development of visualisation technology, video double-lumen tubes (VDLTs) are gradually being used for lung isolation. The VDLT (Weili Medical Instrument Ltd, Guangdong, China) has an embedded camera and a light source between the tracheal and bronchial cuffs (Fig. 1a). The display screen is externally connected to achieve continuous airway visualisation (Fig. 1b). The VDLT can make intubation more precise and avoid unnecessary stimulation caused by blind insertion and repeated positioning, which may reduce the risk of airway injuries. However, because of the installation of a camera, the outer diameter of the main tracheal cuff (the thickest part of the tube) of the VDLT is thicker than that of the corresponding part of the same size as the DLT, which increases the potential risk of airway injuries. There are few studies on the effect of VDLT intubation on airway injury. Therefore, this study aimed to evaluate the effects of VDLT on intubation complications in patients undergoing thoracic surgery.
 Fig. 1:
Fig. 1: Profile features of video double-lumen tubes (a); the carina appears on an external display (b).
Methods StudyThe protocol of this prospective randomised controlled clinical trial was approved by the Ethics Committee of Xuzhou Cancer Hospital, Xuzhou, China, reference number 2022-02-045-k01 (Chairperson Professor Qiang Wang) on 14 July 2022 and registered at the Chinese Clinical Trial Registry website (trial registration code: ChiCTR2300067348, main researcher: Shanshan Zhu, registration date: 05 January 2023). There were no protocol changes after trial commencement. Written informed consent was obtained from all patients before surgery. This study was conducted from January 2023 to June 2023 at Xuzhou Cancer Hospital.
PatientsWe recruited patients aged 18 to 75 years with ASA physical status class I to III scheduled for elective thoracic surgery requiring DLT insertion. The exclusion criteria were preexisting airway injuries, sore throat or hoarseness, BMI at least 35 kg m−2, expectation of difficult airway, high risk of respiratory complications (e.g. asthma, pharyngitis, chronic obstructive pulmonary disease or recent pneumonia), DLT size ≤32Fr, Cormack–Lehane grade >II, history of one-lung ventilation, replacement of other lung isolation techniques due to failure of DLT intubation, inability to perform early extubation due to admission to the Intensive Care Unit or other reasons after surgery, and patients with a second operation within postoperative 3 days. Patients who refused to participate or to provide written informed consent were also excluded.
Enrolled patients were randomly allocated to either the DLT or VDLT group, using a computer-generated randomisation code. The allocation ratio was 1 : 1. Randomisation was performed by an anaesthesiologist who was only in charge of the group assignment. The randomisation sequence was kept in sealed opaque, identical envelopes and the envelopes were opened just before preparation of the tube. The patients and outcome assessors for trachea and vocal cord injuries, postoperative sore throat and hoarseness were blinded to group assignment.
Intervention and anaesthesiaWhen patients were admitted to the operating room, standard monitoring of vital signs, including peripheral oxygen saturation, electrocardiogram, noninvasive blood pressure, invasive arterial blood pressure, cerebral state index (CSI) and train-of-four stimulation (TOF), was performed. The DLT or VDLT was selected according to the envelope instructions. The tube size was selected according to the measurement of the inner diameter of the trachea at the sternal head plane of the chest computed tomography (measurement method: the image was magnified to 300% to reduce the measurement error, and the average value was taken after repeated measurements three times). Either a 35 Fr, 37 Fr or 39 Fr tube was selected according to the inner diameter of the trachea (13–14.9, 15–16.9, ≥17 mm, respectively).9 Anaesthesia was induced with 0.3 mg kg−1 etomidate, 0.5 μg kg−1 sufentanil and 0.6 mg kg−1 rocuronium. Before intubation, the condition of the vocal cords and trachea was observed and recorded using fibreoptic bronchoscopy (FOB). A DLT or VDLT was inserted when the following optimum intubation conditions were achieved: absence of eyelash reflex, CSI less than 65, and TOF ratio = 0. After the bronchial tip of the tube had entered the glottis, it was rotated 90° or 180° to the left to help the cuff enter the glottis and direct the bronchial tip towards the left main bronchus. In the DLT group, the DLT was blindly advanced until reaching an adequate depth or facing considerable resistance preventing further advancement.10,11 Successful intubation was indicated when ensuring that the bronchial tip of the DLT was in the left lung and the carina and bronchial cuff of the DLT were observed to be in the same plane by FOB.11 In the VDLT group, the VDLT was visibly advanced until it was observed on the external display screen that the bronchial cuff had entered the left bronchus and was in the same plane as the carina. Successful intubation is indicated when the bronchial tip of the VDLT is located in the left lung by auscultation. These procedures were performed by an independent anaesthetist with more than 10 years of experience in anaesthesia.
During the operation, tracheal and bronchial intracuff pressures were measured at 30 min intervals and maintained within 25 and 44 cmH2O, respectively.4,12 Anaesthesia was maintained with propofol, remifentanil and rocuronium. The infusion rate was adjusted according to invasive blood pressure and CSI. Intraoperative blood pressure was maintained at 20% above and below the baseline value, and CSI was maintained at 40–60. Mechanical ventilation was performed with a tidal volume of 6–8 ml kg−1 during two-lung ventilation, a tidal volume of 4–6 ml kg−1 during one-lung ventilation, and a PEEP of 5 cmH2O. Other ventilator settings were adjusted to maintain the end-tidal carbon dioxide level at 35 to 45 mmHg. A unified lung collapse strategy was used.
At the end of surgery, the patients were placed in the supine position instead of the lateral position. To make the video recording of the tracheal and vocal cord injuries more stable and clearer, the FOB was inserted into the bronchial lumen of the DLT, and the tracheal condition was videotaped while extubation was performed under anaesthesia. Then, a laryngeal mask was placed for ventilation, and vocal cord injuries were recorded with FOB through the laryngeal mask. With the recording function of the FOB, images of the trachea and vocal cord were saved as video files. Finally, the patient was sent to the postanaesthesia care unit for stabilisation and transferred to the ward after the laryngeal mask was removed. Intravenous patient-controlled analgesia (PCA) was administered for postoperative pain management. The PCA regimen was as follows: 3 μg kg−1 sufentanil were diluted up to 200 ml with 0.9% saline, followed by a continuous infusion rate of 4 ml h−1, a bolus of 2 ml and a lockout interval of 20 min.
Study outcomesThe primary outcomes were the incidence of moderate-to-severe tracheal injury and vocal cord injury. The secondary outcomes included the incidence and severity of postoperative 24 and 48 h sore throat and hoarseness, first-attempt success rate, intubation time, incidence of misplacement of DLT to the right bronchus, incidence of hypoxaemia, quality of lung collapse and change in mean arterial pressure before vs. after insertion (ΔMAP).
Tracheal and vocal cord injuries were assessed by a blinded senior anaesthesiologist who observed the video files. The severity of the tracheal injuries was defined as follows: none, mild (redness, oedema, 1 to 3 patchy haemorrhagic lesions), moderate (≥3 mild lesions or 1 diffuse haemorrhagic lesion) and severe (≥2 diffuse haemorrhagic lesions or oedema causing the disappearance of the tracheal ring).8,13 The depths were divided into the following four levels: subglottic (just below the vocal cords), main trachea, carina and bronchus. With respect to the vocal cord, the types of lesions were classified as follows: oedema, swollen mucosa; petechiae, small red spots on the mucosa; and haematoma, bleeding into the mucosa. The Prince Henry Hospital Pain Score14 was used to categorise sore throat as level 0, 1, 2 or 3, indicating no pain when coughing; pain only when coughing; pain when breathing deeply, but not at rest; pain at rest, but mild and tolerable and excruciating pain at rest, respectively. Hoarseness was graded from 0 to 3: 0, no hoarseness; 1, noticed by the patient; 2, obviously noticed and 3, unable to speak.5
During intubation, the Cormack–Lehane grade and resistance to placing the DLT into the vocal cords and advancing it through the trachea into the left main bronchus were recorded. Resistance was ranked as none, mild or moderate according to the evaluation of the anaesthesiologist who performed the DLT intubation.8 Intubation time was defined as the duration between the laryngoscope lifting of the epiglottis and the first time at which no further manipulation of the (V)DLT was needed. After DLT insertion, the FOB was used to confirm the position of the bronchial cuff, and the timing was stopped if the cuff position was appropriate and no further manipulation was needed. The time to successful intubation was the time after the VDLT was inserted, when both cuffs were inflated, and if no further manipulation was needed. In both cases, if further manipulation of the tube was required after the first inflation of both cuffs, then the time at which the cuffs were re-inflated and no further manipulation taking place became the time to successful intubation. First-attempt success was defined as tube placement directly to the correct position without secondary adjustment. Hypoxaemia, defined as SpO2 less than 90, was recorded during intubation. The quality of lung collapse was evaluated by the surgeon 10 min after the start of the operation, which was graded from 0 to 3: 0, complete collapse; 1, partial residual gas; 2, residual gas interfering with surgical exposure; and 3, no collapse. ΔMAP was defined as the difference in mean arterial pressure as measured just before tube insertion and at the point of successful tube insertion. In addition, the type of surgery, tube rotation angle for entering the glottis, duration of DLT, duration of laryngeal mask, and FOB view grade were also recorded. The FOB view grade,15 indicating whether the laryngeal mask had been accurately positioned, was graded from 1 to 4: 1, indicating that the glottis was seen completely without any obstruction; 2, the glottis was seen only partially, with the visual obstruction less than 50%; 3, the glottis was barely seen, with the visual obstruction more than 50% and 4, the glottis was not seen.
Statistical analysisSample size calculation was performed using PASS 15.0 (NCSS, LLC, Kaysville, Utah, USA). The expected incidence of moderate-to-severe tracheal injury was based on the results of a preliminary trial (n = 40). With a set at 0.05 and 1-bset at 80%, the sample size required to detect a difference of 20% in the incidence of sore throat between the VDLT group (53.3%) and the DLT group (33.3%) was 91 patients in each group. Assuming a 5% loss to follow-up, 96 patients were required for each group; therefore, 192 patients were included in the study.
Numerical variables were analysed for normality by the Kolmogorov–Smirnov test. Normally distributed continuous variables were expressed as the mean ± standard deviation (SD) and compared using the independent samples t test. Nonnormally distributed continuous variables are expressed as the median [interquartile range] and were compared using the Mann–Whitney U test. Categorical variables are presented as numbers (%) and were compared using the χ2 test, Fisher's exact test, or the Wilcoxon rank-sum test in the case of ordinal variables (sore throat severity, hoarseness severity, resistance to advance through trachea, quality of lung collapse grade and FOB view grade). Intubation time was assessed using Kaplan–Meier curves, which were compared using the log-rank test. SPSS version 25.0 software (IBM Corp., Chicago, Illinois, USA) was utilised for all statistical analyses. All P values were two-sided, and a P value of less than 0.05 was considered to indicate statistical significance.
ResultsOf the 204 patients evaluated for eligibility, 12 were excluded (8 declined to participate and 4 met the exclusion criteria) and the remaining 192 patients were randomly assigned to one of the two groups. Of the 192 patients enrolled, 10 dropped out and 182 completed the study (Fig. 2). Patient characteristics, age-adjusted Charlson comorbidity index (ACCI), DLT size, side of surgery, type of surgery, duration of DLT, duration of laryngeal mask, Cormack–Lehane grade and FOB view grade were comparable between the two groups (Table 1).
 Fig. 2:
Fig. 2: CONSORT flow diagram.
Table 1 - Characteristics of patients, anaesthesia and surgery DLT group (n = 90) VDLT group (n = 92) P value Age (years) 59.5 ± 11.0 58 ± 12.5 0.367 Male sex 43 (47.8) 43 (46.7) 0.888 Height (cm) 163.6 ± 7.5 163.7 ± 7.7 0.783 Weight (kg) 65.9 ± 10.5 65.9 ± 11.4 0.794 BMI (kg m−2) 24.4 ± 3.4 24.4 ± 3.1 0.928 ASA 0.861 I 23 (25.6) 23 (25) II 60 (66.7) 64 (69.6) III 7 (7.8) 5 (5.4) ACCI 3.4 ± 1.5 3.2 ± 1.5 0.247 Smoking history 23 (25.6) 19 (20.7) 0.432 Tube size 0.393 35 Fr 35 (38.8) 28 (30.4) 37 Fr 32 (35.6) 41 (44.6) 39 Fr 23 (25.6) 23 (25) Side of surgery 0.426 Left 41 (45.6) 35 (38.0) Right 46 (51.1) 51 (55.5) Mediastinum 3 (3.3) 6 (6.5) Type of surgery 0.735 Wedge lung resection 12 (13.3) 10 (10.9) Pulmonary segment resection 33 (36.7) 31 (33.7) Lobectomy 42 (46.7) 45 (48.9) Mediastinal mass resection 3 (3.3) 6 (6.5) Duration of DLT (min) 153.8 ± 51.5 145.4 ± 42.6 0.173 Rotation angle for entering glottis 0.097 90° 78 (86.7) 71 (77.2) 180° 12 (13.3) 21 (22.8) Duration of laryngeal mask (min) 13.2 ± 2.7 12.9 ± 2.0 0.526 Cormack–Lehane grade 0.833 Grade 1 70 (77.8) 72 (78.2) Grade 2 18 (20) 19 (20.7) Grade 3 2 (2.2) 1 (1.1) FOB view grade 1.000 Grade 1 84 (93.3) 85 (92.4) Grade 2 5 (5.6) 6 (6.5) Grade 3 1 (1.1) 1 (1.1)Data are presented as mean ± SD or number (%). ACCI, age-adjusted Charlson Comorbidity index; DLT, double-lumen tube; FOB, fibreoptic bronchoscopy.
The incidence of moderate-to-severe tracheal injury was 32/90 (35.6%) in the DLT group, and 45/92 (48.9%) in the VDLT group (P = 0.077; relative risk 1.38, 95% CI, 0.97 to 1.95). The incidence of vocal cord injury was 31/90 (34.4%) in the DLT group, and 34/92 (37%) in the VDLT group (P = 0.449) (Table 2).
Table 2 - Trachea and vocal cord injuries DLT group (n = 90) VDLT group (n = 92) P value RR (95% CI) Trachea injury Severity 0.077 None 27 (30.0) 18 (19.6) Mild 31 (34.4) 29 (31) Moderate 27 (30) 38 (41.3) Severe 5 (5.6) 7 (7.6) Total incidence 0.074 1.38 (0.97 to 1.95) None-mild 58 (64.4) 47 (51.1) Moderate– severe 32 (35.6) 45 (48.9) Level of injury Subglottic 18 (20) 29 (31.5) 0.091 1.58 (0.95 to 2.62) Main trachea 23 (25.6) 39 (42.4) 0.019 1.66 (1.08 to 2.54) Carina 17 (18.9) 10 (10.9) 0.148 0.57 (0.28 to 1.19) Bronchus 16 (17.8) 6 (6.5) 0.023 0.37 (0.15 to 0.90) Vocal cord injury 0.449 None 59 (65.6) 58 (63.0) Petechiae 21 (23.3) 18 (19.6) Oedema 10 (11.1) 16 (17.4) Haematoma 0 (0) 0 (0)Data are presented as number (%). 95% CI, 95% confidence interval; RR, relative risk.
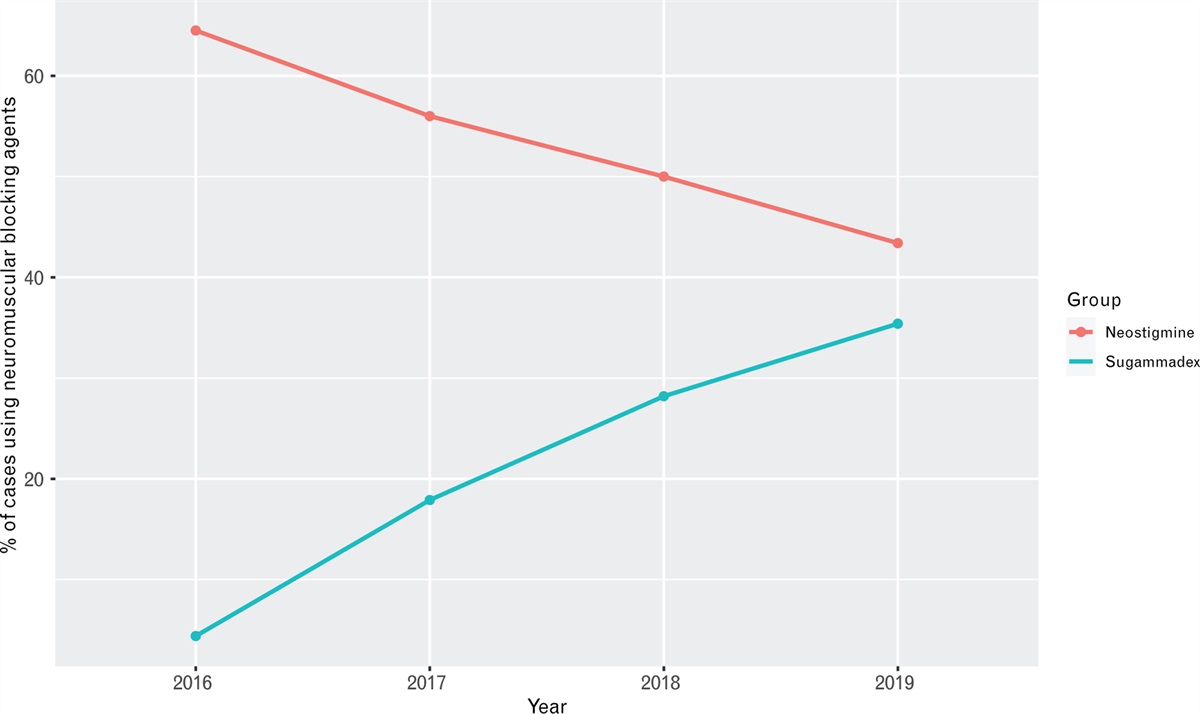
The incidence of postoperative 24 h sore throat and hoarseness was significantly higher in the VDLT group than in the DLT group (for sore throat: P = 0.032, relative risk 1.63 95% CI, 1.03 to 2.57; for hoarseness: P = 0.018, relative risk 1.48, 95% CI, 1.06 to 2.06, Table 3). The severity of sore throat and hoarseness was significantly increased in the VDLT group compared with the DLT group at postoperative 24 h (for sore throat: P = 0.038; for hoarseness: P = 0.014) (Table 3). However, the incidence and severity of sore throat and hoarseness were comparable in both groups at postoperative 48 h (Table 3).
Table 3 - Postoperative sore throat and hoarseness in the two groups DLT group (n = 90) VDLT group (n = 92) P value RR (95% CI) Sore throat 24 h 21 (23.3) 35 (38) 0.032 1.63 (1.03 to 2.57) Prince–Henry Pain score 0.038 0 69 (76.7) 57 (62.0) 1 10 (11.1) 18 (19.6) 2 9 (10.0) 13 (14.1) 3 2 (2.2) 4 (4.3) 4 0 (0) 0 (0) Sore throat 48 h 8 (8.9) 11 (12) 0.629 1.35 (0.56 to 3.19) Prince–Henry Pain score 0.492 0 82 (91.1) 81 (88.0 1 7 (7.8 9 (9.8) 2 1 (1.1) 2 (2.2) 3 0 (0) 0 (0) Hoarseness 24 h 33 (36.6) 50 (54.3) 0.018 1.48 (1.06 to 2.06) Severity 0.014 0 57 (63.3) 42 (45.7) 1 22 (24.4) 30 (32.6) 2 11 (12.2) 20 (21.7) 3 0 (0) 0 (0) Hoarseness 48 h 10 (11.1) 17 (18.5) 0.211 1.66 (0.81 to 3.43) Severity 0.421 0 80 (88.9) 75 (81.5) 1 9 (10.0) 15 (16.3) 2 1 (1.1) 2 (2.2)Data are presented as number (%). Sore throat was ranked by Prince–Henry Pain Score. 95% CI, 95% confidence interval; RR, relative risk.
The quality of lung collapse, ΔMAP, and resistance to advance through the trachea were comparable in both groups (Table 4). The intubation time was significantly shorter in the VDLT group than in the DLT group (P < 0.001). The Kaplan–Meier curves also illustrated that the intubation time in the VDLT group was shorter (log-rank P < 0.01, Fig. 3). The VDLT group had a higher first-attempt success rate and a lower incidence of hypoxemia during intubation (P < 0.001). The incidence of misplacement of the DLT to the right bronchus was also lower in the VDLT group than in the DLT group (P = 0.023, Table 4).
Table 4 - Intubation profiles and haemodynamic responses DLT group (n = 90) VDLT group (n = 92) P value ΔMAP (mmHg) 19.7 ± 8.0 22.6 ± 10.2 0.065 Intubation time (s) 138 [122,148] 96 [91,102] <0.001 First-attempt success 13 (14.4) 84 (91.3) <0.001 Misplacement of DLT to right bronchus 11 (12.2) 3 (3.3) 0.023 Hypoxaemia 19 (21.1) 3 (3.3) <0.001 Quality of lung collapse 0.850 0 76 (84.4) 78 (84.8) 1 8 (8.9) 12 (13.0) 2 6 (6.7) 2 (2.2) 3 0 (0) 0 (0) Resistance to advancement in trachea 0.790 None 16 (17.8) 12 (13.0) Mild 57 (63.3) 69 (75.0) Moderate 17 (18.9) 11 (12.0)Data are presented as mean ± SD or numbers (%). Intubation times are indicated as median (interquartile range). 95% CI, 95% confidence interval; ΔMAP, mean arterial pressure immediately after insertion–mean arterial pressure before insertion; RR, relative risk.
 Fig. 3:
Fig. 3: Intubation time of successful attempts to successful insertions.
DiscussionCommon intubation complications include sore throat, hoarseness and vocal cord and tracheal injuries. The assessment process for sore throat is not sufficiently objective, which can easily affect the results of the study. The main outcomes of this study were the incidence of tracheal injury and vocal cord injury, which are more objective criteria for evaluating the impact of VDLT on tracheal intubation complications. Our study found that there was no significant difference in the incidence of tracheal injury and vocal cord injury between the VDLT group and the DLT group. However, the absolute increase in the incidence of moderate-to-severe tracheal injury in the VDLT group was 13.3%. According to the relative risk (1.38) for moderate-to-severe tracheal injury in the VDLT group, we found that the risk of moderate-to-severe tracheal injury was 1.38 times greater with the VDLT than with the DLT. Studies by Heir et al.16 and Rolf Schuepbach et al.17 suggested that the use of VDLT is associated with a higher incidence of airway injuries. However, their study was limited by the small sample size and lack of sufficient power to account for the differences in airway injuries.
The level of tracheal injury differed between the two groups. The incidence of the level of main tracheal injuries in the VDLT group was higher than that in the DLT group, which may be related to the larger outer diameter of the VDLT. The incidence of injury at the bronchial level was lower in the VDLT group than in the DLT group. The reason may be that, with the help of the continuous visual characteristics of the VDLT, the tube stopped immediately when it entered the appropriate position, avoiding injury caused by repeated adjustment due to a poor position of the tube.
In addition, this study found that the incidence of postoperative 24 h sore throat and hoarseness was higher in the VDLT group than in the DLT group. This may be related to the larger diameter and harder quality of the VDLT. This suggests that intubation with VDLT may result in more adverse patient experiences on the day after surgery. In the future, we need to explore more ways to alleviate the adverse experiences of patients. However, the incidence of sore throat and hoarseness in the two groups was similar and lower at postoperative 48 h. It has been suggested that the use of VDLT intubation causes more sore throats and hoarseness, which last for a shorter time and are easy to resolve. There were no serious complications such as tracheal rupture or mucosal laceration in either group.
In this study, the incidence of postoperative 24 h sore throat was 23.3% in the DLT group and 38% in the VDLT group. In previous studies,17,18,19 the reported incidence of sore throat was 14–90%. Compared with those studies, our experiment showed that the incidence of postoperative 24 h sore throat in the two groups was lower. It may be that the extubation of the DLT under anaesthesia, allowed for avoidance of a severe cough caused by the DLT stimulating the trachea during the extubation process, thus reducing the injury during the entire extubation period. Replacing DLT with laryngeal mask ventilation under anaesthesia may reduce the incidence of postoperative sore throat and reduce the adverse experience of patients, which needs further research to be proven in the future.
We also assessed the intubation process. We found that the VDLT group had a shorter intubation time and a higher first-attempt success rate, which benefited from the visualisation afforded by the VDLT. Our results are consistent with previous results.20–22 In the DLT group, the DLT was blindly advanced until reaching an adequate depth or facing considerable resistance, preventing further advancement. The first-attempt success ra
留言 (0)