
記住我

Neuromuscular blocking drugs (NMBDs) are usually administered by an intravenous injection, but accidental extravasation may occur when a peripheral intravenous catheter is not positioned correctly. Risk factors for extravasation are small or fragile veins, advanced age, obesity, multiple venipunctures, high injection pressure, poor cannula fixation, the presence of disseminated skin diseases and patient movement during cannula placement.1 One study found that up to 39% of the cannulas were dislocated after 72 h.2 Depending on the injected drug, leakage in the surrounding extravascular tissue may cause harmful effects such as local irritation or even tissue necrosis.3 Moreover, the injected drug may be absorbed into the circulation and cause systemic effects.
As NMBDs are often used during induction of anaesthesia, it is likely that anaesthetists may encounter accidental extravasation of NMBDs. However, little is known about the absorption of NMBDs injected into the subcutaneous tissue and their effect on the onset and the duration of the neuromuscular block. This review aims to summarise the current evidence on extravasation of NMBDs and its systemic adverse effects. Additionally, a flowchart will be presented to guide clinical decision-making after the extravasation of NMBDs.
MethodsThe recommendations and checklist from the PRISMA 2020 statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) were used to construct this narrative review. A literature search was performed on 5 February 2023 in the Ovid MEDLINE and Ovid EMBASE database using the search terms ‘rocuronium’, ‘pancuronium’, ‘vecuronium’, ‘atracurium’, ‘cisatracurium’, ‘mivacurium’ or ‘succinylcholine’ in combination with ‘subcutaneous’, ‘paravenous’, ‘extravasation’ or ‘extravascular leakage’.
All abstracts and titles that contained a combination of these search terms, were published before February 2023 and were written in English, were considered. Three authors assessed the articles independently for their relevance. The exclusion criteria were defined as follows: the NMBDs were injected intramuscularly, only the abstract was available, articles concerning the paediatric population or animals and studies where agents other than NMBD agents were injected subcutaneously. References of the selected articles were also screened using the above-mentioned exclusion criteria.
The following variables were extracted from the selected articles: age, sex, weight, type of NMBD, injection site, difficult intravenous insertion, intravenous cannula already in situ, dose of NMBD (subcutaneous, intravenous and total dose), onset and duration of neuromuscular block, reversal of the neuromuscular block [time, train-of-four (TOF) count or ratio, agent and dose], type of surgery and duration of postoperative monitoring after extubation. The articles were also screened for risk factors that could influence the absorption and metabolism of NMBDs such as peripheral vascular disease, skin oedema, chronic renal failure, hepatic insufficiency, obesity, use of anticonvulsants, prolonged immobility and burns.
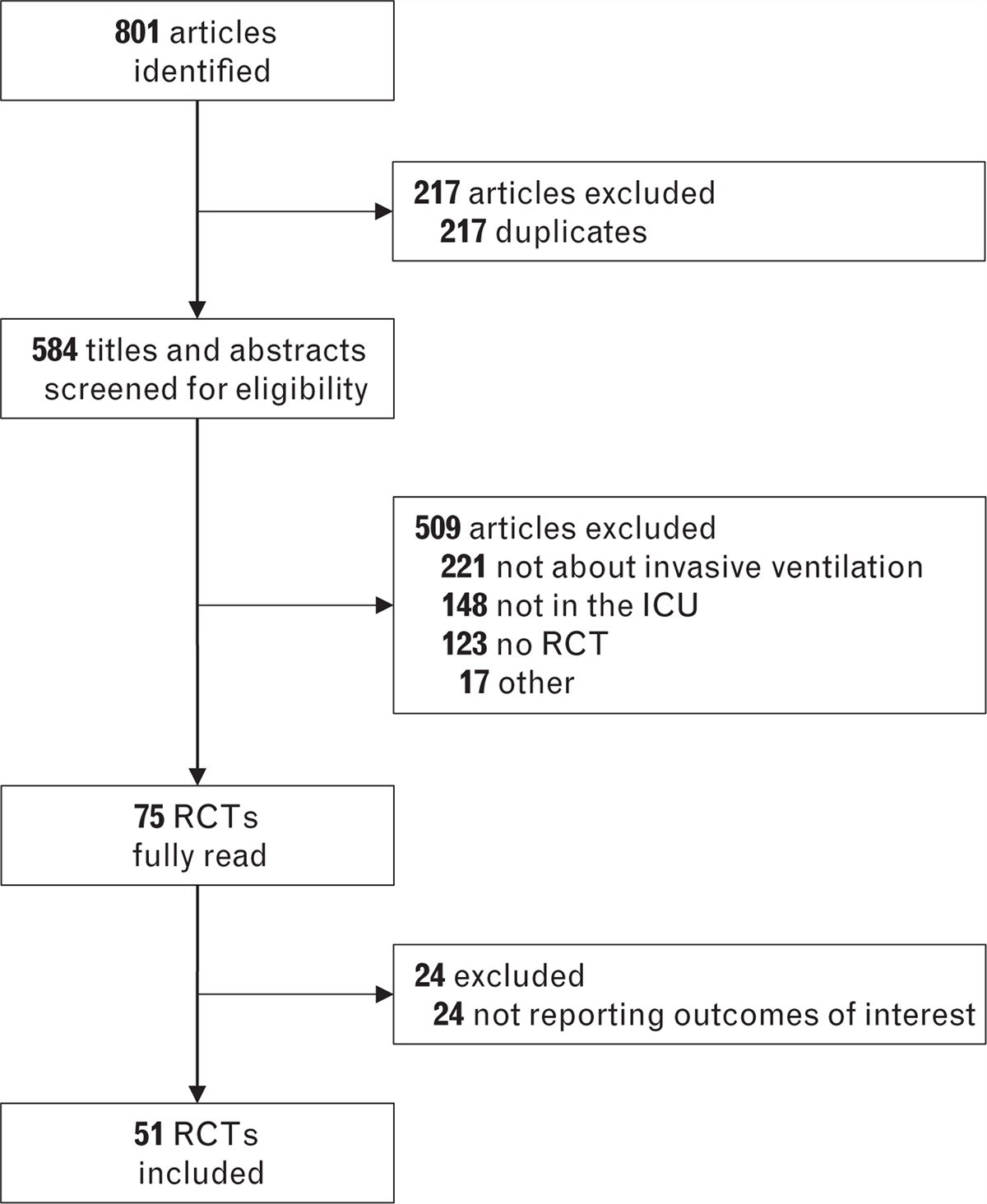
ResultsThe initial search revealed 77 articles after removal of duplicates. From these 77 articles, 71 were excluded based on the exclusion criteria. Most articles were excluded because no extravasation of NMBDs occurred. Ultimately, our search yielded nine articles: seven case reports,4–10 one case series describing four cases11 and one article reporting one case report with a consecutive clinical trial.12 The flow of the articles can be found in Fig. 1.
 Fig. 1:
Fig. 1: Flow of the articles retrieved on Embase and Medline.
The demographics of the patient and characteristics of the intravenous insertion and procedure are listed in Table 1. The median age was 59 years, the male/female distribution was 6/6 with an average BMI of 25 kg m−2. Two cases reported the presence of the intravenous cannula upon arrival in the operating room.6,8 Three cases reported difficult insertion of the intravenous cannula.7,8,10
Table 1 - Demographics, characteristics of intravenous insertion and type of surgery Case Age (years) Sex Weight (kg) BMI (kg m−2) Difficult i.v. i.v. present Type of surgery Comorbidity 14 69 M 86 NA NA NA Lymph node biopsy Chronic renal failure 25 65 F 114 NA NA NA PTA Morbid obesity, PAD 36 51 F 67 25 No Yes Knee debridement Chronic renal insufficiency, DM, Skin oedema 47 59 F 120 48 Yes No CCE Morbid obesity, AHT, CVA 58 38 F 82 33 Yes Yes Mastectomy Obesity 611 18 M 65 21 No NA Abscess debridement Hepatic insufficiency 711 21 F 80 28 NA NA Ovarian cyst resection Encephalitis, Immobility 811 75 M 30 13 NA NA Intracranial haematoma evacuation AHT, PAD 911 64 M 35 14 NA NA Electroconvulsive therapy Immobility 109 NA F NA NA NA NA Neurosurgery Chronic renal failure 1110 22 M NA NA Yes No Wound care after burn injury 1° Burns (4 days, 45% BSA) 1212 67 M 54 NA No No Brain tumour resection NAAHT, arterial hypertension; BSA, body surface area; case column, case number with reference in superscript; CCE, cholecystectomy; CVA, cerebrovascular accident; DM, diabetes mellitus; F, female; i.v., intravenous cannula; M, male; NA, information not available; PAD, peripheral arterial disease; PTA, percutaneous transluminal angioplasty.
Table 2 shows the characteristics of the subcutaneous injection of NMBDs. Rocuronium was used in nine cases,4–8,11 vecuronium in two cases9,10 and pancuronium in one case.12 No case reports were retrieved describing the extravasation of atracurium, cisatracurium, mivacurium or succinylcholine. Only three cases mentioned that the intravenous line was checked prior to induction.6,8,9 Except for one case, all cases suspected extravasation because of the observation of local swelling.11 None of the cases reported a high injection pressure during initial injection. The subcutaneous injections occurred at the level of the upper (n = 8),4–7,9,11 the lower (n = 2) extremity8,12 and the neck (n = 1).10 One case did not specify the site of injection.11 The median doses of the subcutaneous injection of rocuronium and vecuronium were 1.1 and 0.1 mg kg−1, respectively. The dose of pancuronium was 0.1 mg kg−1. After the suspicion of extravasation, seven patients received an additional dose of intravenous NMBD (five patients rocuronium and two patients vecuronium) to facilitate intubation and achieve adequate surgical relaxation before the start of the surgery.5,7–9,11 All intravenous top-up doses of NMBDs were administered through a newly placed intravenous line. In four cases, the additional intravenous top-up dose of NMBD was given prior to measurement of the TOF count.5,9,11
Table 2 - Parameters of the neuromuscular block Dose (mg kg−1) NMB Reversal Case NMBD Injection site Total SC IVa Onset Onset (min) Duration (min) TOF Agent Dose (mg kg−1) Duration of monitoring after reversal (h) 14 Roc Dorsum hand 1.2 1.2 0 Delayed 35 80b 1/4d Sug 4 5 25 Roc Elbow 0.4 0.4 Vec 5 mg Delayed NA 60b 4/4d Neo 0.04f NA 36 Roc Elbow 1.0 1.0 0 Delayed 20 140b 2/4d Sug 4.5 6 (ICU) 47 Roc Dorsal wrist 0.8 0.4 0.4 Delayed NA 120b 2/4d Sug 2 4 58 Roc Greater saphenous vein 1.2 0.6 0.6 Delayed NA 180b 4/4d Sug 2 4 611 Roc Forearm 1.2 1.1 0.1 NA NA 75b 100%d Sug 2.3g 1 711 Roc NA 1.9 1.3 0.6 Delayed NA 201c 1/4e Nonei None ICU 811 Roc Forearm 2.7 1.7 1.0 Delayed NA 337c 1/4e Nonei None ICU 911 Roc Forearm 0.9 0.9 0 NA NA NA 4/4d Sug 17.1h 5 109 Vec Elbow 0.2 0.1 0.1 Delayed NA 240c 4/4e Nonei None ICU 1110 Vec External jugular vein 0.1 0.1 0 Delayed NA 130b NA Neo 2.5 mgj NA 1212 Pan Ankle 0.1 0.1 0 Delayed 10 330b 46%d Neo 0.05 2Case column: case number with reference in superscript. ICU, transfer to intensive care unit; IV, intravenous; NA, information not available; Neo, neostigmine; NMB, neuro muscular block; NMBD, neuro muscular blocking drug; Pan, pancuronium; Roc, rocuronium; SC, subcutaneous; Sug, sugammadex; Vec, vecuronium.
aIV dose of NMBD via a new intravenous cannula.
bDuration is time between injection of the NMBD and the time of reversal.
cDuration until measured start of spontaneous recovery of train-of-four (TOF).
dTOF at time of reversal.
eTOF at measured start of spontaneous recovery.
fPatient remained ventilated and sedated because she had to lie flat postoperatively for 4 h. Reversal was given after 4 h because of unknown absorption of the s.c. NMBD.
gReversal was given because of unknown absorption of SC NMBD.
hThe first dose (200 mg) of SUG was probably given SC, the second dose (200 mg) completely reversed the NMB, the third dose (200 mg) was because of unknown absorption of the SC NMBD.
iSedation and mechanical ventilation until complete spontaneous recovery of the NMB.
jWeight not mentioned.
Apart from the doses mentioned in Table 2, no additional doses of NMBDs were given during the procedure. This resulted in an average total (intravenous with subcutaneous) injected dose of 1.4, 0.2 and 0.1 mg kg−1 for rocuronium, vecuronium and pancuronium, respectively. One of these patients received an intravenous injection of vecuronium after an initial extravasation of rocuronium and was thus not included in our calculation of median and average doses.5 All cases noticed a delay in onset of neuromuscular blockade, based on TOF measurement and clinical findings such as persistent spontaneous respiration. Three of the cases reported a time of onset of the neuromuscular block with a median delay of 20 min.4,6,12 The depth of neuromuscular block throughout the procedure was measured using TOF count or ratio, except for one case in which the patient had extensive burn injuries and placement of electrodes was impossible.10 With exception of cases 2 and 9, which did not specify electrode placement, all cases using TOF measurement applied electrodes to the ulnar nerve to evaluate thumb adduction.4,6–12 All of the subcutaneous injections of NMBDs were the result of an accidental extravasation during administration of NMBDs through a peripheral venous catheter.
Nine patients had a measured residual neuromuscular block at the end of the surgery.5,10,11 The median time of the surgical procedures was 138 min. In nine patients, the neuromuscular block was reversed at the end of the surgery: in six patients, sugammadex was administered and in three patients, neostigmine was used.4–8,10–12 Sugammadex was only used in cases where rocuronium was administered as sugammadex was not yet available when the case with extravasation of pancuronium occurred. The median time of the administration of the reversal agent after induction was 125 min. The median doses of sugammadex and neostigmine were 3.2 mg kg−1 and 45 μg kg−1, respectively. The other three patients were sedated and mechanically ventilated in the intensive care unit (ICU) until complete spontaneous recovery of the neuromuscular block occurred.9,11 The patients not admitted to the ICU spent a median of 4 h in the recovery room after extravasation of NMBDs.
DiscussionIn most cases, extravasation of NMBDs resulted in an unpredictable neuromuscular block with a delayed onset and prolonged duration of the neuromuscular motor block, requiring reversal agents for safe extubation of the patients.
The plasma concentration of inadvertent extravascular injection of NMBD is dependent on the balance between the rate of absorption of the NMBD from the subcutaneous tissue and the elimination of the NMBD from the plasma. In contrast to intravenous injection where the plasma concentration immediately peaks after administration, subcutaneous injection results in the formation of a subcutaneous depot, from which the NMBD is slowly absorbed into the systemic circulation. The pharmacokinetics of the subcutaneous injected NMBDs may be altered as this depends on many factors such as lipid solubility, protein binding and local tissue perfusion. Therefore, most of the cases report a delayed onset, failure of muscle relaxation and a prolonged duration of action of the NMBDs. However, seven patients received a supplemental dose of NMBDs through a newly placed intravenous cannula and this explains the high total dose of NMBDs administered. The additional dosing of NMBDs makes interpretation of the pharmacokinetic effects after subcutaneous administration of NMBDs impossible. Moreover, the initial dose of NMBD may be partially injected intravenously considering some cases reported a loss of consciousness despite extravasation. Only a small portion of the case reports mention that they had checked the intravenous line prior to intravenous injection. It is hard to know whether this was simply not reported in some articles, but we would like to highlight that not checking the patency of the intravenous line prior to intravenous injection is unsafe practice and that the intravenous line must always be checked, particularly when NMBDs are used or if there is a pre-existing intravenous line of uncertain quality.
Absorption is dependent on the site of the subcutaneous depot. Iwasaki et al.12 compared the TOF ratio of the same dose of pancuronium after intravenous injection, subcutaneous injection in the hand and subcutaneous injection in the ankle. The onset of the neuromuscular block in the subcutaneous ankle group was delayed in comparison to the subcutaneous hand group and the intravenous group. Furthermore, twitch recovery was much slower in the subcutaneous ankle group in comparison to the subcutaneous hand group and the intravenous group. In the subcutaneous hand group and the intravenous group, a complete neuromuscular block was observed in all subjects. In contrast, only one patient in the subcutaneous ankle group achieved a complete neuromuscular block. These findings suggest that the site of extravasation influences the pharmacokinetic profile. The skin blood flow is generally higher in the upper than in the lower body half, as a result the absorption from a subcutaneous depot is faster in the upper body half.13 This skin blood flow is also increased by general anaesthesia.14 NMBDs injected in more vascularised regions will likely have a faster onset and recovery than regions that are less vascularised. For the same reason, factors that affect the local circulation such as diabetes and atherosclerosis, may decrease the absorption of the subcutaneous NMBD, making it very difficult to predict its onset and duration of action. Longer duration of action may occur in patients when elimination is impaired, such as in chronic renal failure, where rocuronium has a 37% longer elimination half-time.15
LimitationsThis article reviewed the literature on extravasation of NMBDs, but there are several limitations.
First, few randomised controlled trials are available, and most literature consists of case reports. As a result, there is a lot of heterogeneity between the different reports. Furthermore, because of the small sample size, no statistical analysis was performed.
Second, we were not able to retrieve articles that discussed the subcutaneous injection of atracurium, cisatracurium, mivacurium or succinylcholine. Extravasation of short-acting NMBDs, such as succinylcholine or mivacurium, might not be of clinical importance because of a faster elimination than absorption rate.
Third, we could not extract any data from these case reports concerning the delayed extubation time, incidence of postreversal recurarisation nor the quality of reversal.
Last, the topic of extravasation of NMBDs remains subject to publication bias. Cases with a bad or good outcome may be underreported in the literature. Clinicians may not have related the bad outcome to extravasation of NMBDs. Therefore, it would be beneficial to have qualitative randomised clinical trials that examined the effects of subcutaneous injection of NMBDs.
Guidelines for management of extravasation of neuromuscular blocking drugsA clinical pathway based on current literature is suggested in Fig. 2. Preventive measures include correct labelling of medication as well as assessing the quality of the intravenous line. If an intravenous cannula is present, the injection site should be checked for oedema, inflammation and pain. We recommend that the administration of NMBDs via an intravenous cannula with absence of backflow or increased injection pressure should be handled with caution.
 Fig. 2:
Fig. 2: Management pathway
After suspicion of extravasation, a new intravenous line should be secured as soon as possible to ensure safe anaesthesia. After accidental subcutaneous injection, a prolonged and unpredictable duration of neuromuscular block must be presumed, certainly if additional intravenous doses of NMBDs were administered. Quantitative monitoring of the neuromuscular block should always be applied as there is a risk for ongoing neuromuscular block. Ideally the application of the TOF monitoring should take place at the start of induction of anaesthesia to assess the onset of the neuromuscular block. After suspected extravasation of NMBDs, we advise TOF measurement before an additional intravenous dose of NMBD is administered to accommodate anaesthesia best practices. NMBDs might have a delayed absorption from subcutaneous tissue, therefore, spontaneous recovery or stabilisation of the neuromuscular block must be observed before reversal. Prolonged ventilation and sedation may be required at the end of the surgery.
Once the TOF count or ratio is increasing, reversal of NMBDs can be obtained with sugammadex and neostigmine. Though, because of its pharmacological profile and the possibility of a prolonged neuromuscular block, sugammadex is the product of choice after aminosteroid NMBDs.16,17 Not only can any further absorbed NMBDs be neutralised by the circulating sugammadex, it also has no unwanted muscarinic side effects, less residual muscle paralysis and a longer elimination half-life compared with neostigmine (100 to 150 vs. 50 to 90 min).18 Sugammadex has been associated with perioperative anaphylaxis, though the incidence is rare.19 A local subcutaneous injection of sugammadex could theoretically encapsulate aminosteroid NMBDs, yet this remains to be explored.
When a TOF ratio of greater than 0.9 is observed, the patient can be safely extubated.20 Monitoring after extubation should include regular measurement of the neuromuscular block, full ASA-monitoring and extended stay in a postanaesthesia care unit (PACU) for a minimum of 4 to 5 h. This prolonged observation is certainly important when long acting NMBDs are used. If there is a decline in TOF ratio during this period of observation, an additional dose of sugammadex is necessary when an aminosteroid NMBD has been used. If the maximum dosage of neostigmine is given to reverse a neuromuscular block caused by a nonaminosteroid NMBD and this results in an insufficient recovery of TOF ratio, we advise not to repeat the dose but to observe the patient in the ICU under prolonged sedation and ventilation.
We would like to highlight that the recommendations in our clinical pathway include guidelines that were not studied or explored but rather based on clinical expertise and scientific basis. Further research is required to assess any clinical benefit.
ConclusionExtravasation of NMBDs is a potentially dangerous complication that requires adequate anaesthetic management. Current literature consists of articles with heterogeneous data. The available literature suggests that extravasation of NMBDs can result in a neuromuscular block with delayed onset and prolonged and unpredictable duration. Currently, no guidelines exist on how to approach an accidental subcutaneous administration of NMBDs. Therefore, we suggest a clinical pathway that can be used after extravasation of NMBDs. This pathway includes observation with thorough monitoring, the potential need for prolonged sedation and ventilation and a suggested method to reverse the neuromuscular block.
Acknowledgements relating to this articleAssistance with the study: none.
Financial support and sponsorship: none.
Conflicts of interest: none.
Presentation: none.
This manuscript was handled by Dan Longrois.
References 1. Schulmeister L. Extravasation management: clinical update. Semin Oncol Nurs 2011; 27:82–90. 2. Probe high extravasation rates [Internet]. Extravasation Information 2020. 2020 [cited 21 May 2023]. Available at: https://extravasation.org.uk/probe.htm. [Accessed 12 February 2023]. 3. Lake C, Beecroft CL. Extravasation injuries and accidental intra-arterial injection. Contin Educ Anaesth Crit Care Pain 2010; 10:109–113. 4. Navare SR, Garcia Medina O, Prielipp RC, et al. Sugammadex reversal of a large subcutaneous depot of rocuronium in a dialysis patient: a case report. AA Pract 2019; 12:375–377. 5. Awad N, Zalut S, Deutsch E. Successful management of subcutaneous infiltration of an intubating dose of rocuronium in a morbidly obese patient: a case report. J Anaesth Crit Care Case Rep 2018; 4:21–23. 6. Doshu-Kajiura A, Suzuki J, Suzuki T. Prolonged onset and duration of action of rocuronium after accidental subcutaneous injection in a patient with chronic renal failure-a case report. JA Clin Rep 2021; 7:18. 7. Timmermann TN, Mongan PD, Hoefnagel AL, Braunecker S. Management of subcutaneous infiltration of rocuronium: a case report. J Clin Anesth 2021; 71:110203. 8. Kim DH, Kim SM, Kim J, et al. Sugammadex reversal of large subcutaneous injection of rocuronium in an obese patient. Med Biol Sci Eng 2020; 3:16–19. 9. Tarmey NT, Edward AM, Eynon CA. Prolonged neuromuscular block following accidental subcutaneous injection of vecuronium. Anaesthesia 2011; 66:956–957. 10. Usha DR, Balasubramanyam M, Omkarappa S, et al. Accidental subcutaneous injection of vecuronium bromide in a patient with burns. J Evol Med Dent Sci 2014; 3:11903–11907. 11. Takagi S, Kijima M, Iwasaki H, et al. Extravascular leakage of induction doses of rocuronium: four cases in which both depth of neuromuscular block and plasma concentration of rocuronium were assessed. J Clin Monit Comput 2022; 36:587–592. 12. Iwasaki H, Namiki A, Omote T, et al. Neuromuscular effects of subcutaneous administration of pancuronium. Anesthesiology 1992; 76:1049–1051. 13. Tsuchida Y. Regional differences in the skin blood flow at various sites of the body studied by xenon 133. Plast Reconstr Surg 1987; 80:705–710. 14. Landsverk SA, Kvandal P, Bernjak A, et al. The effects of general anesthesia on human skin microcirculation evaluated by wavelet transform. Anesth Analg 2007; 105:1012–1019. 15. Miller R, Meistelman C, Lien C, et al. Pharmacology of neuromuscular blocking drugs. Miller's anesthesia. Philadelphia: Elsevier Saunders; 2015. 16. Hristovska AM, Duch P, Allingstrup M, et al. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev 2023; 8:CD012763. 17. Postoperative recurarization after sugammadex administration due to the lack of appropriate neuromuscular monitoring: the Japanese Experience [Internet]. Anesthesia Patient Safety Foundation. [cited 2023 Sep 16]. Available at: https://www.apsf.org/article/postoperative-recurarization-after-sugammadex-administration-due-to-the-lack-of-appropriate-neuromuscular-monitoring-the-japanese-experience/. [Accessed 15 September 2023]. 18. Abad-Gurumeta A, Ripollés-Melchor J, Casans-Francés R, et al. Evidence Anaesthesia Review Group. A systematic review of sugammadex vs neostigmine for reversal of neuromuscular blockade. Anaesthesia 2015; 70:1441–1452. 19. Zecic F, Smart MH, Abbey TC, et al. Sugammadex-induced anaphylactic reaction: a systematic review. J Anaesthesiol Clin Pharmacol 2022; 38:360–370. 20. Sauer M, Stahn A, Soltesz S, et al. The influence of residual neuromuscular block on the incidence of critical respiratory events. A randomised, prospective, placebo-controlled trial. Eur J Anaesthesiol 2011; 28:842–848.
留言 (0)