
記住我

The results from a recent large prospective international cohort study described a 3.3% incidence of chronic postsurgical pain (CPSP) at 12 months after non-cardiac surgery.1 In 2019, the International Association of the Study of Pain redefined CPSP as pain that develops or increases in intensity after a surgical procedure, persists for at least 3 months and is localised to the surgical field.2,3 It is estimated that over 50 million surgical procedures are performed in Europe each year and the potential burden of CPSP is likely to be large.4
CPSP has a negative impact on the quality of life, as well as on emotional and physical well being.5,6 Thus, clinical prediction models are needed to identify patients at high risk of developing CPSP and to support pre-operative and postoperative clinical decision-making based on an individual patient's risk profile. To reach this goal, we need large prospective studies to determine the CPSP risk factors, incidence and characteristics.
In a recent systematic review of existing prediction models for CPSP, the models posed several statistical and practical limitations for use in clinical settings. These included, most notably, small sample sizes, poor reporting or inappropriate handling of missing data, lack of model performance measure evaluation, and absence of model validation.7 There was also significant heterogeneity in the tools used to measure CPSP, pain intensity cut-off values to distinguish between individuals with and without CPSP, and length of follow-up times. Additionally, most models were limited to specific populations and surgical procedures and therefore lack generalisability.
The IMI-PainCare project, targeting improved care of patients suffering from acute or chronic pain, is supported by the IMI-PainCare consortium, a public–private partnership supported by the European Union's Horizon2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations (EFPIA) within the Innovative Medicines Initiative 2 (IMI-PainCare, 2018: https://www.imi-paincare.eu). PROMPT (Providing Standardised Consented PROMs (Patient Reported Outcome Measures) for Improving Pain Treatment), a subsidiary study of the IMI-PainCare project, aims at improving management of acute and chronic pain by identifying a core set of PROMs that are predictive indicators of treatment success, in both clinical practice and controlled trials. To achieve this aim, an extensive literature search and a consensus process on core outcome domains were executed then completed by a review of literature on factors of pain persistence after surgery.8 As an integral part of the PROMPT study, the current study (Non-Interventional Trial-1, NIT-1), was conducted as a large prospective, non-interventional, multicentre study to collect clinical and PROM data from hospitals across Europe. The primary goal of NIT-1 was to use these data to propose a score to predict those patients likely to having CPSP at 6 months after surgery. Secondary endpoints were the differences in the incidence and characteristics of CPSP for the four types of surgery as well as pain-related functional impairment at 6 months.
Methods Recruitment of European participants centresTo ensure sufficient inclusion numbers, we advertised participation in our study throughout Europe, using a network of former study sites and the webpage of the well established projects PAIN OUT and QUIPS.9,10 If the estimated number of procedures of interest and potential patient recruitment were sufficient, conclusion of a co-operation-agreement was the next step. This co-operation agreement ensured adherence to the standard operating procedure, confidentiality, data exploitation rules, and regulated the remuneration.
Ethical considerationsApproval for the study was obtained from the local ethics committee at each centre, and General Data Protection Regulation clearance was needed for all participating hospitals. Patients’ consent could be oral or written, depending on the local requirements. Ethics requirements vary considerably across Europe.11 Ethics approval for the study was obtained at Jena University Hospital's Ethics Board (Reg. No. 2019-1298-Bef on 06.02.2019). The PROMPT NIT-1 study was registered (clinicaltrials.gov ID: NCT03834922)
Population of patients includedPatient inclusion criteria in NIT-1 were as follows: the patient was due to undergo elective surgery of one of the four different types (i.e., breast surgery for cancer, total knee arthroplasty (TKA), sternotomy and endometriosis surgery); was ≥18 years old; fluent in one of the languages of the available questionnaire; and agreed to participate in the study (Table 1). A pre-existing chronic pain condition at the site of surgery or as a comorbidity was not an exclusion criterion. The four types of surgery were chosen to cover surgery with or without pre-operative pain, pain in both sexes, and visceral pain after endometriosis surgery.
Table 1 - Specific surgical inclusion and exclusion criteria Inclusion criteria Exclusion criteria Breast surgery Woman ≥18 years oldCABG, coronary artery bypass grafting; CPSP, chronic postsurgical pain; HLM, heart lung machine; TKA, total knee arthroplasty.
We used five main components for data management and processing: a subject-ID-generator, OpenClinica (OpenClinica LLC and collaborators, Waltham, MA, USA), an address tool, a follow-up survey tool and LimeSurvey (LimeSurvey GmbH, Hamburg, Germany). After patients had given their informed consent, the study team generated a subject-ID and recorded the patient's contact details (name, e-mail-address, phone number and OpenClinica-ID). Survey invitations were generated and sent to patients as a private link. Most patients then completed the questionnaires online in LimeSurvey. If patients did not respond or did not have an e-mail address, the invitation link was sent to the hospital where the patient was recruited, so that the study team could contact the patient by telephone. In this case, the information was obtained verbally and entered into LimeSurvey by the study staff.
Evaluation around surgeryNIT-1 was conducted as a multicentre, noninterventional study in 18 hospitals across Europe in patients undergoing one of four surgical procedures: these were sternotomy, total knee arthroplasty (TKA), breast cancer surgery, and endometriosis surgery. The patients completed questionnaires about their pain at seven time points: pre-operatively (the patients were interviewed the day before surgery or the morning of surgery when surgery was ambulatory), on postop day (POD)1, POD3, POD7 and postop month (POM)1, POM3 and POM6. At these time points, patients were evaluated with established instruments measuring patient-reported outcomes, modified questionnaires, and selected single items. The data, timing of data collection and modality of analysis (i.e., continuous or dichotomous) are presented in Table 2. Twenty-eight different questionnaires in eight languages were used (7 time-points × 4 procedure specific questionnaires in English, French, German, Italian, Serbian, Finnish, Spanish and Portuguese). Three types of items were incorporated into the PROMPT NIT-1 questionnaires: existing questionnaires, modified existing questionnaires, and newly developed items. Translations were available for most of the existing questionnaires whereas modifications and new questions required translation. Translations were carried out according to a defined forward-backward-procedure with double-checks as previously reported.12,13
Table 2 - Questionnaires used in IMI PROMPT NIT1 observational study Questionnaires Pre-op Intra-operative POD1 P0D3 POD7 M1 M3 M6 Demographics X Educational level X Comorbidities X Clinical data - ICD-10-CM X - Anaesthesia X - Type of surgery X IPO (modified) X X X X PROMs (WP2) X X X X ASES adapted X Pain - BPI X X X X - DN4 interview X X X X X X - NPSI X X Analgesic use X X X X X X X X PSQ X Adverse events X Psychological profile - HADS X - PCS X - Pain expectation X QOL (EQ-5D-5L) X X X X Laboratory values - WBC, CRP X XASES adapted, 11-point scale using a modified version of the Arthritis Self-Efficacy Scale and used as a continuous scale; BPI, Brief Pain Inventory used as a dichotomous variable with the pain interference total score; CRP, C-reactive protein; DN4, Douleur Neuropathique 4 questions questionnaire used as a dichotomous variable; HADS, Hospital Anxiety and Depression scale used as a continuous variable; ICD-10-CM, International Classification of Diseases – Tenth Revision – Clinical Modification; IPO, International Pain Outcome Questionnaire; NPSI, neuropathic pain symptom inventory used as a continuous variable; Pain expectation, questionnaire on pain expectation used as a continuous variable; PCS, Pain catastrophising scale used as a continuous variable; PROMs,patient related outcome measures; PSQ, Pain sensitivity questionnaire used as a continuous variable; QOL, quality of life; WBC, white blood cell; X, indicates that the questionnaire was used at the time point.
The primary end point was the incidence of moderate to severe CPSP (NRS > 3/10) at 6 months using the average pain on the BPI (Brief Pain Inventory) questionnaire (‘Please rate your pain by circling the one number that best describes your pain on the average’). Secondary outcome measures were the incidence of moderate to severe CPSP at 1 and 3 months; and neuropathic pain characteristics and pain interference with daily activities for patients with CPSP at 6 months. The neuropathic component of pain was evaluated with the DN4 interview questionnaire which has been validated previously to distinguish neuropathic pain (positivity if score on the DN4 questionnaire ≥ 3/7).14,15 This questionnaire was used both pre-operatively and postoperatively to create a dichotomous variable. The functional interference with daily activities was evaluated with the pain interference total scores (PITS) obtained from the BPI questionnaire.16 The psychological interference was evaluated with the Hospital Anxiety and Depression Scale (HADS).17 The quality-of-life interference was evaluated with the EQ-5D-5L questionnaire.18 The location of pain in the pre-operative and the postoperative period was identified in the BPI diagram with the question ‘the area that hurts the most’ since we considered it was the most problematic type of pain for the patient. The CPSP was defined according to this area that hurts the most whatever the location
The power calculation was based on an expected incidence of 15% for moderate-to-severe CPSP and an expected follow-up rate of 67%.19,20 Thus, 4000 data sets (1000 for each surgical procedure) had to be included to result in 400 patients with CPSP.
We applied the least absolute shrinkage and selection operator (LASSO) regression as the method of variable selection for the primary outcome of CPSP after 6 months with all potential predictors as independent variables.21 Most demographic and clinical variables collected before surgery and at the other time points after surgery were included in the model before variable selection. LASSO is a regression analysis method, which performs variable selection in order to minimise the prediction error. This is achieved by imposing a constraint on the model parameters shrinking the regression coefficients towards zero: this is achieved by forcing the sum of the absolute value of the regression co-efficients to be less than a fixed value λ. Considering a linear regression with p potential predictors xij and outcome values yi for i = 1, …, n and j = 1, …, p the LASSO algorithm performs the minimisation of ∑i=1nyi−∑j=1pxi,jβj2+ λ ∑j=1p|βj|,21
For the binary outcome CPSP a logit link function was applied in the model. Variables with a regression coefficient ßj of zero after shrinkage are excluded from the model. In this way the complexity of the model will be reduced, including only the variables that are predictive for the outcome variable. Reducing the number of variables in the final model also prevents the issue of overfitting. Traditional approaches like stepwise selection methods (e.g. backward elimination and forward selection procedures) are also capable of identifying a subset of relevant variables, however, the resulting final model depends on the order of the variables which are entered or removed. In LASSO regression all potential variables are entered simultaneously, which avoids this problem and therefore should be preferred for variable selection instead of conventional approaches.22
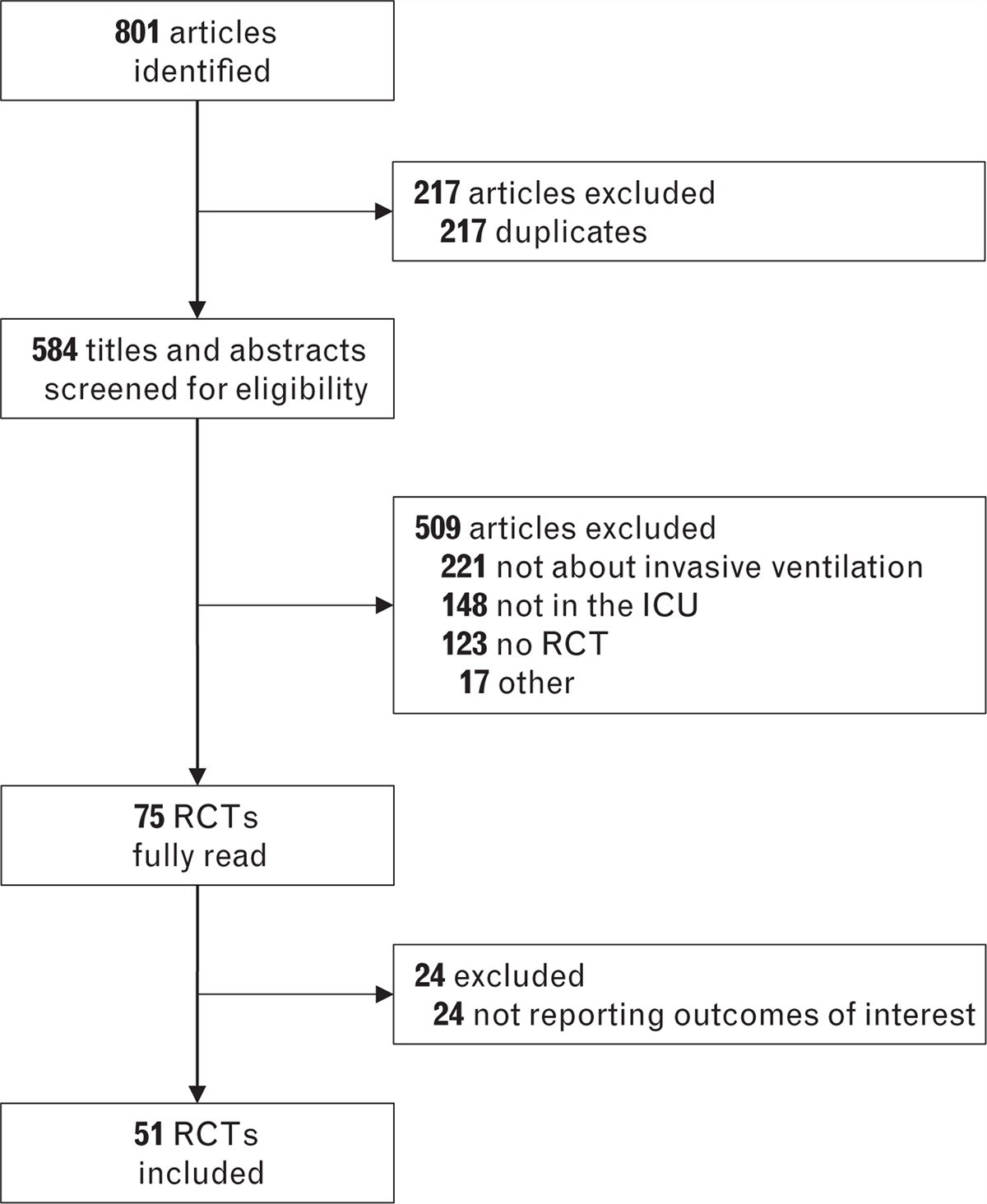
Results Sample characteristicsThe data collection took almost 3 years (first patient in was August 2019, last patient out was June 2022) as the number of elective surgical procedures was significantly reduced due to the COVID-19 pandemic. However, despite the pandemic, the 6 consortium and 12 non-consortium hospitals included a total of 3297 patients during this period. Sufficient case numbers were reached and follow-up rates on POM1, POM3 and POM6 were very good (70 to 80%). The flow chart is described in Fig. 1. Demographic characteristics are listed in Table 3 and missing values are listed in Table 4.
 Fig. 1:
Fig. 1: Flow chart.
Table 3 - Demographics and pain, functional, psychological assessments at baseline Breast surgery (n = 655) Sternotomy (n = 1183) Endometriosis (n = 862) Total knee arthroplasty (n = 597) Sex (female) 650 (99.7) 287 (24.3) 862 (100) 365 (61.1) Age (year) 55.1 ± 11.9 66.4 ± 10.8 32.6 ± 8.1 68.3 ± 9 Height (cm) 165 ± 7 174 ± 9 167 ± 7 167 ± 10 Weight (kg) 70.9 ± 14.7 86.4 ± 16 69.1 ± 14.1 83.4 ± 17.4 Educational level - Primary school 120 (18.6) 180 (15.2) 17 (2) 167 (28.1) - Secondary school 195 (30.2) 551 (46.7) 229 (26.8) 172 (28.9) - Hich school completed 136 (21.4) 222 (18.8) 360 (42.2) 162 (27.2) - University or higher 193 (29.9) 228 (19.3) 248 (29) 94 (15.8) BPI short: preOP pain (yes) 111 (24.3) 152 (16.0) 494 (65.6) 420 (73.7) HADS – anxiety score 6.5 ± 4.2 4.4 ± 3.4 8 ± 3.9 5.7 ± 3.9 HADS – depression score 3.9 ± 3.5 3.1 ± 3.0 5.1 ± 3.7 5.6 ± 3.7 HADS – total score 10.4 ± 7.2 7.5 ± 5.8 13.2 ± 6.9 11.3 ± 7.0 PSQ minor 3.2 ± 1.9 2.4 ± 1.6 2.5 ± 1.3 4.1 ± 1.9 PCS 12.7 ± 10.0 11.4 ± 9.9 21.6 ± 11.2 17.5 ± 12.4 EQ5D VAS 69.2 ± 20.0 66.7 ± 19.7 68.1 ± 20.6 63.1 ± 18.9 PITS 2.5 ± 2.2 3.4 ± 2.2 3.8 ± 2.3 4.6 ± 2.2 Pain expectation – anxiety 50.4 ± 30.1 44.1 ± 27.7 56.5 ± 28.8 36.0 ± 29.6 DN4 (yes/no) 45 (17.0) 47 (10.3) 235 (38.0) 175 (31.7)Values are presented as mean ± SD or number (%).BPI, Brief Pain Inventory with specific question on pre-operative pain frequency; DN4, Douleur Neuropathique 4 questions questionnaire; EQ5D VAS, visual analogue scale of the quality of life EQ5D questionnaire; HADS, Hospital Anxiety and Depression scale with three subcores on anxiety, depression and total score; Pain expectation, questionnaire on pain expectation; PCS, pain catastrophising scale; PITs, pain interference total score extracted from BPI; PSQ minor, pain sensitivity questionnaire.
Data are presented as number or percentage.DN4, Douleur Neuropathique quatre question questionnaire; HADS, Hospital Anxiety and Depression Scale; IPO, International Pain Outcome questionnaire; PCS, Pain Catastrophizing scale score before surgery; PITS, functional Pain Interference Total Score on Brief Pain Inventory questionnaire before surgery; POD, postoperative day; PSQ, Pain Sensitivity Questionnaire.
Moderate to severe CPSP at 6 months was reported by 10.5% of the whole patient cohort with variations across the four surgical models: 6.9% for sternotomy, 7.4% for breast surgery, 12.9% for TKA and 16.2% for endometriosis (Fig. 1 and Table 5).
Table 5 - Incidence of persistent pain at 1, 3 and 6 months Breast surgery (n = 655) Sternotomy (n = 1183) Endometriosis (n = 862) TKA (n = 597) Total population (n = 3297) CPSP at 1 month - Missing data 175 289 173 121 758 - No 430 (89.6) 773 (86.5) 580 (84.2) 328 (68.9) 2111 (83.1) - Yes 50 (10.4) 121 (13.5) 109 (15.8) 148 (31.1) 428 (16.9) CPSP at 3 months - Missing data 200 281 225 137 843 - No 412 (90.5) 835 (92.6) 555 (87.1) 393 (85.4) 2195 (89.4) - Yes 43 (9.5) 67 (7.4) 82 (12.9) 67 (14.6) 259 (10.6) CPSP at 6 months - Missing data 194 317 251 140
留言 (0)