
記住我

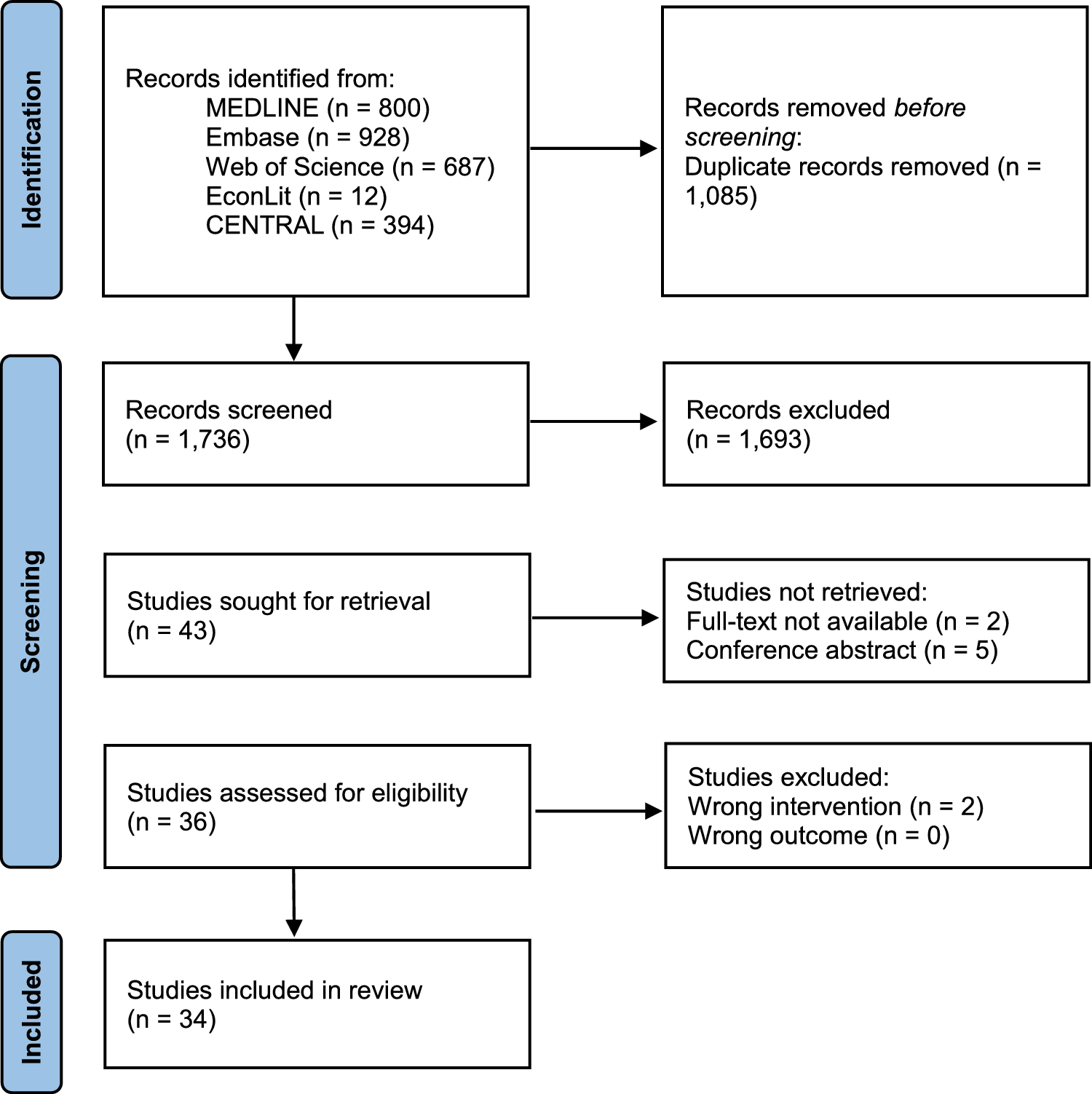
Figure 1, the PRISMA flowchart, presents the systematic review process and search results.
Fig. 1
Literature search flow diagram using the PRISMA checklist. From: Page MJ, McKenzie JE, Bossuyt PM, et al., The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372: n71. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses, QoL quality of life
A total of 26,434 studies were identified. Of these, 16,010 duplicate articles were removed, resulting in 10,424 studies. A further 12 were identified through web searching via Google Scholar. Titles and abstracts were screened, and 10,374 studies did not meet the inclusion criteria and were removed. The reasons for exclusion were (1) adult population and (2) childhood HRQoL PROMs that do not use pictorial response scales or items. Full texts for 44 studies were assessed independently by the three reviewers. A total of 22 PROMs, including 28 unique versions, were identified in the review. The reviewers’ overall agreement (inter-rater reliability) was calculated using Cohen’s kappa and yielded a good agreement (k = 0.72).
3.2 Overview of Identified PROMs3.2.1 Origin, Population, and SettingTables 1 and 2 provide a detailed summary of the identified generic and condition-specific PROMs, respectively. More measures were developed in the USA (n = 9, [32%]) [31,32,33,34,35,36,37,38] and the UK (n = 8, [29%]) [39,40,41,42,43,44] than elsewhere. Four PROMs were from the Netherlands (n = 4, [14%]), three from France (n = 3, [11%]) [45,46,47], and one each from Finland [48] and Australia [49]. Two PROMs, the DISABKIDS Smileys TAKE 6 [50] and the Hvidoere Smiley Faces International diabetes quality of life assessment tool for young children (Hvidoere Smiley Faces) questionnaire [51], were developed as part of multi-country collaborative projects.
Table 1 Summary of characteristics of included generic preference-based and non-preference-based childhood patient-reported outcome measuresTable 2 Summary of characteristics of included condition-specific non-preference-based childhood patient-reported outcome measuresAll the PROMs were developed for children < 18 years, except for one (Dartmouth Primary Care Cooperative Information Project Charts [COOP Charts]) [33], designed for children 12–18. Study participants were recruited from schools, clinics, hospitals, or the general public.
Description of PROMsA detailed description of the identified generic and condition-specific PROMs is provided in Tables 1 and 2. We identified 22 PROMs, including 28 unique versions. Two PROMs were versions of the Auto Questionnaire Enfant Image/Child Pictured Self Report (AUQUEI), i.e. AUQUEI Nursery and AUQUEI Primary [46]. Two were different versions of the Pediatric Quality of Life Inventory (PedsQL): PedsQL Generic Core Scales—Young Child (PedsQL GCS—Young Child) [34] and PedsQL Short Form 15—Young Child (PedsQL SF15—Young Child) [35]. Three were different versions of the Dutch Children’s AZL/TNO Quality of Life (DUX): the Short Form (DUX-25) [52], the celiac disease version of the DUX-25 (CDDUX) [53], and the Bone Tumour DUX-25 (Bt-DUX) [54]. Another three were different versions of the Childhood Asthma Questionnaire (CAQ): Childhood Asthma Questionnaire-A (CAQ-A), Childhood Asthma Questionnaire-B (CAQ-B), and Childhood Asthma Questionnaire-C (CAQ-C) [42]. A further three PROMs were versions of the Child Health Rating Inventories (CHRIS): CHRIS—general health scales [32], CHRIS—preoperative anxiety, and CHRIS—postoperative pain management [36]. The remaining 15 were single-version measures, presented in Box 1.
Box 1 Single-version pictorial patient-reported outcome measures (PROMs)Of the 28 unique PROM versions, two (7%) are generic PROMs accompanied by preference-based value sets (i.e. Child Health Utility 9 Dimension [CHU9D] animation/Children’s Health States Preferences Learnt from Animation [CHILDSPLA] and 17-dimensional measure of health-related quality of life [17D]), and the remaining 26 (93%) are not preference-weighted measures.
All the PROMs were developed between 1993 and 2021, with the majority developed after 2000 (n = 20, [71%]). The earliest measures to be developed were the CAQ-A, CAQ-B, and CAQ-C in 1993. The most recently developed are the CHRIS—preoperative anxiety and CHRIS—postoperative pain management (2021).
Fifteen (54%) of the PROMs were generic, 11 (39%) were condition specific, and two (7%) were domain specific. The conditions targeted include asthma (n = 4), celiac disease (n = 1), chronic conditions (n = 1), cochlear implants (n = 1), bone tumour (n = 1), diabetes (n = 1), inflammatory bowel disease (IBD) (n = 1), and skin conditions (n = 1). The domains targeted were preoperative anxiety (n = 1) and postoperative pain (n = 1).
3.3 Criteria for Pictorial PROMs Administration3.3.1 Target Age GroupsThe youngest age for self-reported childhood PROMs with pictorial illustrations available is 3 years (TedQL), while the oldest is 18 years (COOP Charts). Of the 28 PROM versions examined, one measure, AUQUEI Nursery, targets children younger than 5. The PedsQL GCS—Young Child, PedsQL SF15—Young Child, and the Pediatric Asthma Quality of Life Questionnaire (PAQLQ)—Pictorial version target children aged 5–7 years, while three measures (17D, Paediatric Measure Yourself Medical Outcomes Profile [P-MYMOP], and CAQ-B) are intended for children 8–11 years. Measures explicitly designed for adolescents (12- to 18-year-olds) include the COOP Charts and the CAQ-C. Seventeen PROMs covered multiple age groups: the AUQUEI Primary, TedQL, Child Health and Illness Profile—Child Edition Child Report Form (CHIP-CE CRF), CHRIS, DUX-25, Exeter Quality of Life (ExqoL), KidIQoL, Quality of Life Scale for Children (QoL-C), the animated computer program for children with IBD, Bt-DUX, CAQ-A, Children’s Dermatology Life Quality Index (CDLQI), CHRIS—preoperative anxiety, CHRIS—postoperative pain management, DISABKIDS Smileys TAKE 6, and the Hvidoere Smiley Faces measure.
3.4 Development and Content Validity of Paediatric Pictorial PROMsTable 3 reports on the development process of paediatric pictorial PROMs, highlighting the involvement of children in the process, the graphic approaches employed, and the pivotal role of pilot testing.
Table 3. Methodological approaches used for developing pictorial measures of quality of life3.4.1 Content Generation MethodsIn the development of the identified paediatric pictorial PROMs, various methods were used, including literature reviews, expert consultation, focus groups, and interviews. The breakdown of these approaches among the PROMs is as follows: almost half (43%) of the identified PROMs (12 out of 28) utilised literature reviews in their development process. Similarly, 43% of the PROMs (12 out of 28) incorporated focus groups during development. Expert consultation played a role in developing approximately one-third (32%) of the PROMs (9 out of 28). Interviews were the most commonly employed method, with 17 out of 28 PROMs (32%) using them as part of their content and item generation process. These approaches highlight the diverse methodologies employed in the development of pictorial paediatric PROMs, contributing to their depth and comprehensiveness.
3.4.2 Children’s Involvement in the Development of Pictorial ElementsThirteen studies emphasised the active participation of children in crafting the pictorial elements for HRQoL measures. PROMs in this category include CHU9D animation/CHILDSPLA, KidIQoL, P-MYMOP, QoL-C, TedQL, PAQLQ—Pictorial version, Cochlear Implant Quality of Life (Cochlear Implants—QOL), CHRIS—postoperative pain management, CAQ-A, CAQ-B, CAQ-C, and DISABKIDS Smileys TAKE 6. This collaborative approach aimed to create instruments that are more child-friendly, engaging, and relevant to the unique experiences of children.
In contrast, 15 PROMs, including 17D, AUQUEI Nursery, AUQUEI Primary, CHIP-CE CRF, COOP Charts, DUX-25, ExqoL, PedsQL GCS—Young Child, PedsQL SF15—Young Child, CDLQI Cartoon version, CDDUX, Hvidoere Smiley Faces, Bt-DUX, CDDUX, and the animated computer program for children with IBD, did not explicitly mention the participation of children in the design of pictorial versions.
3.4.3 Diverse Graphic Methods for Varied Content DomainsVarious graphic methods were employed depending on the content of different domains in the development of paediatric pictorial PROMs. This approach was taken to address the potential challenges in visual representation and ensure that the instruments could effectively capture children's experiences in diverse aspects of HRQoL.
For example, in domains related to emotional well-being and mood, some PROMs, such as CHU9D animation/CHILDSPLA, CAQ-A, CAQ-B, and CAQ-C, used ‘smiley’ faces or emoticons with different expressions (such as happy, sad, or neutral) to help children express their feelings. This graphic method made it easier for children to convey their emotional states.
In contrast, for domains related to physical health or daily activities, different graphic approaches were used. Some instruments employed interactive characters, animations, or cartoons to represent various aspects of a child's life, making it more engaging and relatable for them. For instance, the CHU9D animation/CHILDSPLA PROM utilised interactive group sessions with children and an animation filmmaker to create engaging characters that children could relate to.
Additionally, in domains where the assessment required quantifying bother levels or responses to specific items, thermometers or visual scales were used. These visual tools allowed children to indicate the extent to which they were bothered by certain issues, helping in a more precise assessment. For instance, the PAQLQ—Pictorial version PROM used thermometers to gauge bother levels, providing children with a clear and visual way to express their discomfort.
By adapting graphic methods to suit the specific content domains, instrument developers aimed to create measures that were child-friendly, comprehensible, and relevant. This approach recognised the importance of considering the unique challenges associated with visual representation when assessing HRQoL in children.
3.4.4 Pilot TestingPilot testing was found to be an important component of the development phase of 11 of the identified PROMs, playing a vital role in refining the measures. For example, in the case of KidIQoL, children actively took part in the testing process and provided feedback on the instrument, leading to refinements in item representation. Similarly, in the case of P-MYMOP, a pilot feasibility study involving children aged 7–11 was conducted to identify and address challenges, ensuring alignment with children's comprehension and preferences. This thorough pilot testing process ensured that the measures effectively captured children's experiences.
3.4.5 Adaptation from Existing MeasuresSix PROMs were adapted from existing ones: the CHU9D animation/CHILDSPLA (adapted from the CHU9D); the CDLQI Cartoon version (adapted from the CDLQI); the CHIP-CE CRF (adapted from the CHIP CE Parent Report Form [CHIP-CE/PRF]); the QoL-C (adapted from the EQ-5D); the PAQLQ—Pictorial version (adapted from the PAQLQ—Established version); and the P-MYMOP (adapted from the adult MYMOP). Adjustments were made to item and response options and the inclusion of pictures, cartoons, photographs, happy–sad faces, and illustrations to enhance children's understanding. Preferences of children for certain images were observed, emphasising the importance of visual elements in paediatric HRQoL assessment.
3.5 Design and Format of the PROM3.5.1 Response Scales and the Use of Pictorial RepresentationsTables 1 and 2 show that PROMs’ response options and presentation formats were divided into Likert and VAS response scales or a combination of the two. Both scale types were supported by pictorial representations and are thus referred to as pictorial Likert or pictorial VAS hereafter. Almost all the identified PROMs (n = 26, [93%]) used a pictorial Likert scale to present response options. The pictorial Likert scales ranged from a 3-point scale (PedsQL GCS—Young Child, PedsQL SF15—Young Child, QoL-C, PAQLQ) to a 7-point scale (P-MYMOP). Most PROMs (n = 17, [61.0%]) used 4- or 5-point scales. Two PROMs employed the VAS to present response choices [55, 56], i.e. the ExqoL, whose VAS ranged from ‘not like me’ to ‘exactly like me’ [55]. Another PROM, the QoL-C, used a combination of the pictorial Likert scale and the VAS (a horizontal child-friendly health meter ranging from 0 to 10 anchored with happy–sad faces at the extreme ends and in the middle) [41].
Five pictorial presentation styles were identified, with the majority using the happy–sad faces: happy–sad faces (15), cartoons/pictures (9), graduated circles (1), lines (1), thermometers (1), and props (1). For example, the CHU9D animation/CHILDSPLA used a cartoon character, which was then animated and presented in an interactive application on a touchscreen device (Fig. 2). The CHIP-CE used two illustrations depicting each question's two end extreme health states. Each question had five possible response circles, which gradually increased to show the increasing severity as response options advance from ‘never’ to ‘always’ (Fig. 3). In another example, the TedQL used a response scale with circles and lines along with props (two teddy bears) presented by the interviewer to the child (Fig. 4) [44]. Finally, the PAQLQ—Pictorial version employed a response scale using thermometers (Fig. 5).
Fig. 2
Example of a response scale using cartoons (CHU9D animation/CHILDSPLA). The example depicts 5 levels of the sad dimension CHILDSPLA computer animation program, from left to right, 1—‘I don’t feel sad’, 2—‘I feel a little bit sad’, 3—‘I feel a bit sad’, 4—‘I feel quite sad’, and 5—‘I feel very sad’. Reprinted from Abrines Jaume, N., et al., CHILDSPLA: a collaboration between children and researchers to design and animate health states. Child: Care, Health & Development, 2015. 41(6): p. 1140–51, with permission from John Wiley &Sons. CHU9D Child Health Utility 9 Dimension, CHILDSPLA Children’s Health States Preferences Learnt from Animation
Fig. 3
Example of a response scale using illustrations and graduated circles (CHIP-CE). Reprinted from Riley, A.W., et al., The child report form of the CHIP-child edition: reliability and validity. Medical care, 2004: p. 221–231, with permission from Lippincott Williams & Wilkins. CHIP-CE Child Health and Illness Profile-Child Edition
Fig. 4
Reprinted from Lawford, J., Volavka N., and Eiser C., A generic measure of Quality of Life for children aged 3–8 years: results of two preliminary studies. Pediatric Rehabilitation, 2001. 4(4): p. 197–207, with permission from Taylor & Francis Ltd.
Example of a response scale using circles and lines (TedQL).
Fig. 5
Example of a response scale using thermometers (PAQLQ—Pictorial version). Reprinted from Everhart, R.S. and B.H. Fiese, Development and initial validation of a pictorial quality of life measure for young children with asthma. J Pediatric Psychology, 2009. 34(9): p. 966–76, with permission from Oxford University Press. PAQLQ Pediatric Asthma Quality of Life Questionnaire
3.5.2 Recall PeriodThe ISPOR task force report (2013) [12] suggests that shorter recall periods of 24 h or less are favourable for paediatric PROMs used within a regulatory context. A recent systematic review on the design of childhood PROMs in preliminary studies recommends a recall period of 48 h or less for children under 8 years old and 14 days and under for children above 8 [24]. Eight [29%] of the PROMs in this review had a recall period of today or current health: the CAQ-A, CAQ-B, CAQ-C, CHU9D animation/CHILDSPLA, DUX-25, TedQL, 17D, and QoL-C. Three [11%] measures, ExqoL, KidIQoL, and CDDUX, used a general recall period (did not specify a recall period). Another eight [29%] PROMs had recall periods ranging from the past week (CDLQI, P-MYMOP, PAQLQ—Pictorial version, Cochlear Implants—QOL) to the past month (CHIP-CE CRF, COOP Charts, PedsQL GCS, PedsQL SF15). The remaining nine PROMs [32%] did not state the recall period.
The available information for the paediatric pictorial PROMs does not offer specific details about how recall periods were dealt with graphically in these studies.
3.5.3 Mode of AdministrationIn terms of mode of administration, 71% of paediatric pictorial PROMs were designed for self-administration, while 29% were intended for interviewer-assisted administration using electronic and non-electronic data collection methods. Among these, seven PROMs (25%) used electronic data collection methods.
In terms of incorporating pictorial representations in the identified PROMs, there is considerable variability among the studies. The CHU9D animation/CHILDSPLA study notably utilised pictorial versions in multiple modes, including animated presentations, touch-screen interfaces with still images, and hard-copy questionnaires. Conversely, the KidIQoL study did not explicitly specify the use of pictorial versions in either administration method.
Other studies adopted unique approaches. The P-MYMOP study integrated faces scales within interviews, while the QoL-C study employed diverse administration modes, such as one-on-one interviews, classroom activities, and distribution through parents. The TedQL study conducted individual interviews, while the animated computer program for children with IBD employed computer-based animations.
Some studies employed VAS, as demonstrated in the Bt-DUX study. However, others like CAQ-A, CAQ-B, and CAQ-C did not provide explicit information regarding the use of pictorial versions in administration. The CDLQI Cartoon version study lacked specific details on administration methods, and the CDDUX study did not address this aspect at all.
Furthermore, the PAQLQ—Pictorial version study did not specify the mode of administration for pictorial versions, and the Cochlear Implants—QOL study utilised computer-administered methods without providing detailed specifics. Finally, the DISABKIDS Smileys TAKE 6 study did not mention the mode of administration for pictorial versions.
In summary, the incorporation of pictorial versions into the mode of administration for PROMs varied significantly across studies, with some employing diverse methods, while others either did not specify or lacked detailed information on this aspect.
3.5.4 Length of PROMAll the measures contained multiple items, ranging from four (P-MYMOP) to 45 for the CHIP-CE CRF. The estimated time to complete the PROMs ranged from 3 to 5 min (CHU9D animation/CHILDSPLA) to 20–30 min (17D)Footnote 1. Comparing the number of items across versions of the measures showed slightly more items in the versions of the PROMs for older children than those for younger children. For instance, the AUQUEI Nursery version for ages 3–5 years has 26 items, whilst the AUQUEI Primary version for ages 6–11 has 31 items (a difference of 16%). Similarly, the CAQ-A for ages 4–7 years has 14 items, the CAQ-B for ages 8–11 years has 23 items, and the CAQ-C for 12- to 16-year-olds has 41 items.
3.5.5 Scoring of PROMsThe PROMs were scored in one of three main ways: (1) multi-item PROMs only yielding a summary score; (2) multi-item, multidomain scales producing both domain-specific and summary score; and (3) preference-weighted measures that use a value set based on stated preferences for the health states. The scores for the former two are typically determined directly through summary scoring of responses to individual items in the measure.
3.5.6 DomainsTable 4 outlines the domains covered by the PROMs that employ pictorial representations. We combined similar constructs of PROMs under common domain definitions developed for this review. The final ten PROM domains were physical health, social functioning, mental health, emotional health, school, environment, autonomy, pain, disease-specific concepts, and overall QoL.
Table 4. Pictorial patient-reported outcome measures (PROMs) domainsPhysical health refers to PROM items that examine physical functioning status, activity impairment, physical conditions, and related symptoms. Social functioning refers to items that address the ability to engage in social interactions. Items assessing acceptance, friendship, family life and relationships, and social support were also classified under this domain. Mental health refers to items that capture mental and cognitive health conditions. Emotional health refers to items describing one’s experience, perception, and expression of emotions. It includes items such as sadness, worry, and distress. School has facets that address school attendance and participation in schoolwork and activities. Environment covers different aspects of the immediate environmental living conditions. Autonomy refers to items that address a child’s ability to manage their everyday tasks, become more independent, and make their own decisions, e.g. daily routine and looking after myself. Pain relates to items about bodily pain and discomfort. Disease-specific concepts address disease-specific issues, e.g. disease severity, diet, and device management. This domain was limited to condition-specific PROMs only. Overall QoL refers to a single overview item asking respondents to rate their QoL.
The most examined domain was physical health (measured by 21 PROMs), followed by emotional health and social functioning (assessed by 16 PROMs each). The least measured domain was environment, captured by only two PROMs.
3.6 Cross-Cultural IssuesPROMs are generally designed for widespread usage. As such, it is important to address differences due to culture and language during the development of the PROM, as they may impact use and acceptance.
Three measures addressed cultural issues in the PROM development stage. The animated computer program to assess QoL in children with IBD was designed to be culturally acceptable to all Dutch children [57], while the DISABKIDS Smileys TAKE 6 was developed across seven European countries (Austria, France, Germany, Greece, the Netherlands, Scotland, and Sweden) [50, 58]. The Hvidoere Smiley Faces questionnaire was developed in 17 countries as part of a multi-collaborative study [51].
留言 (0)