
記住我









This model examines the cost-effectiveness of adding plasma mcfDNA testing to UC diagnostic tests to further increase the diagnostic yield, expedite the diagnostic process, minimize delays in targeted treatment initiation, and enhance the precision of treatment decisions. This CEA was designed and validated in alignment with good modelling practice guidelines and recommendations [12,13,14]. The modelling approach was informed by a structured review of the clinical and economic literature and refined through a collaborative process utilizing expert clinical perspectives.
Currently, patients with suspected ICHP are initially treated with broad-spectrum antimicrobials prior to identifying the infectious etiology. They undergo various non-invasive (NI) and invasive diagnostic tests, including bronchoscopy, to determine the pneumonia-causing pathogen. As test results become available, treatment strategies are dynamically adjusted to ensure that they are appropriate for the identified pathogens and their susceptibilities to antimicrobials. This personalized approach optimizes therapy, leading to quicker recovery, earlier discharge, and reduced mortality risk.
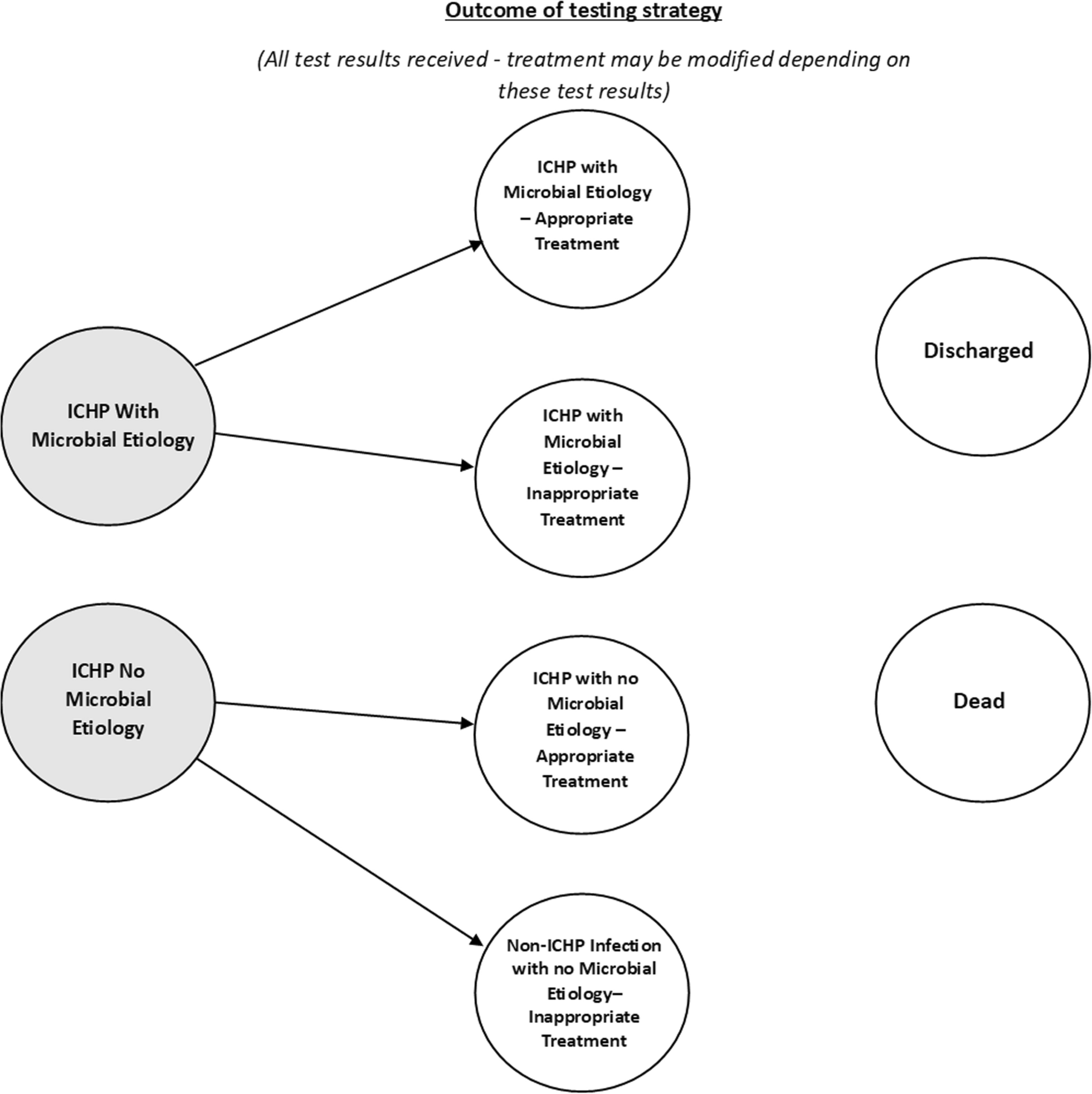
2.1 Model StructureA semi-Markov model structure was implemented in Microsoft Excel® (2023) to compare health outcomes and associated costs from the US payer perspective for the addition of mcfDNA to UC diagnostic testing, including NI and invasive testing. The model structure is presented in Fig. 1. A semi-Markov model relaxes the Markov assumption for sojourn time, allowing for dynamic transition probabilities between health states. The model describes the pathways as patients receive test results and treatment, which may or may not be appropriate given the test result. The primary endpoints of the model were discounted costs, life-years (LYs), equal value life-years (evLYs), quality-adjusted life-years (QALYs), and the incremental cost-effectiveness ratio (ICER) per QALY.
Fig. 1
Structure of semi-Markov model. Arrows represent possible transitions between cycles; grey health states indicate the patient has been tested for ICHP but the test result has not yet been received. ICHP Immunocompromised host pneumonia
The model structure (Fig. 1) was designed to encompass the key aspects of a patient's journey when suspected of ICHP, focusing on microbiological testing results and subsequent changes in antimicrobial treatment. It considers antimicrobial treatment adjustments before and after receiving test results, appropriateness of therapy in response to test results, and patient outcomes including hospitalization, discharge, or death.
Patients start in one of the first two initial health states described below, awaiting a test result, with an ICHP pathogen that may or may not be identifiable. It was assumed that UC and mcfDNA sequencing can detect all identifiable ICHP pathogens, based on the overlap between detectable pathogens by the mcfDNA test and known pneumonia pathogens [15, 53]. Due to different factors that impact test sensitivity, such as time from infection to specimen collection and time on antimicrobials, UC and mcfDNA tests may miss some pathogens that the other might detect. After test results are received, patients transition between model states to indicate whether they receive appropriate or inappropriate treatment (defined below). In any health state, patients can experience mortality or be discharged from the hospital, unless they have an identifiable probable ICHP pathogen, in which case, a test result is always received first (transitions not shown). A half-cycle correction is applied to costs and benefits to account for the movement of patients at any point during a cycle.
The Markov health states in the model are defined as follows:
ICHP with microbial etiology: Patients with clinical signs/symptoms of ICHP with a microbiological evaluation in progress (test result not yet received) that will eventually identify an infectious ICHP etiology. Patients in this state may not be discharged. The proportion of patients that start in this state is informed by the proportion of patients in the population with an infectious ICHP etiology. From this state, patients may transition into the “ICHP with microbial etiology—appropriate treatment” or “ICHP with microbial etiology—inappropriate treatment” model states when test results are received, or they may die.
ICHP with no microbial etiology: Patients with clinical signs/symptoms of ICHP with a microbiological evaluation in progress (test result not yet received) that will not identify an infectious ICHP etiology. This may be due to non-infectious causes or limitations in testing (e.g., prior antibiotic use, low pathogen levels, fastidious organisms). The proportion of patients that start in this state is informed by the proportion of patients in the population without an infectious ICHP etiology. From this state, patients may transition into the “ICHP with no microbial etiology—appropriate treatment” or “Non-ICHP infection with no microbial etiology—inappropriate treatment” model states when a test result is received, or independently of the test result, they may be discharged or die.
ICHP with microbial etiology—appropriate treatment: Patients with clinical signs/symptoms of ICHP with the microbiological evaluation completed (test result received) and an infectious ICHP etiology is identified. Treatment is optimized as necessary so that it is appropriate for the identified pathogen(s). From this state, patients may be discharged, or they may die.
ICHP with no microbial etiology—appropriate treatment: Patients with clinical signs/symptoms of ICHP with the microbiological evaluation completed (test result received) and no infectious ICHP etiology is identified. Treatment is administered based on the clinical data and the assumption of unknown pathogen. From this state, patients may be discharged, or they may die.
ICHP with microbial etiology—inappropriate treatment: Patients with clinical signs/symptoms of ICHP with the microbiological evaluation completed (test result received), and while an infectious ICHP etiology is present, it is missed by the evaluation. Treatment remains unchanged, and thus inappropriate. From this state, patients may be discharged, or they may die.
Note: No further information will become available to guide treatment, meaning that patients in this model state cannot transition into an appropriate treatment health state.
Non-ICHP infection with no microbial etiology—inappropriate treatment: Patients with clinical signs/symptoms of ICHP with the microbiological evaluation completed (test result received) and no infectious ICHP etiology is identified. Treatment remains unchanged, and thus inappropriate.
Note: This model state is only relevant for patients in the UC comparator. No further information will become available to guide treatment, meaning that patients cannot transition into an appropriate treatment health state.
Discharged: Patients who have been discharged from the hospital.
Dead: Patients who have died—all patients in the model are at risk of mortality.
2.2 Target PopulationThe populations considered in the analysis were based on the PICKUP study: immunocompromised hospitalized adult patients undergoing diagnostic bronchoscopy to establish the microbiological etiology of clinically suspected infectious ICHP [11]. The recently published guidelines for ICHP defined the main patient populations at risk by underlying disease states: cancer and hematopoietic cell transplant recipients, patients with HIV, chronic immunosuppression, solid organ transplant, and inborn errors of immunity [1]. The group with one of the highest risks of ICHP is represented in the PICKUP study population: patients receiving treatment for an active hematological malignancy, recently undergoing hematopoietic cell transplantation, or receiving immunosuppressive therapy for active graft versus host disease [1, 9, 16]. The per protocol population (N = 173) was previously defined [11]. The second population (N = 223) encompasses the per protocol population and represents all patients with an adjudicated plasma mcfDNA test, including patients with plasma mcfDNA collected close to but outside 24 h from study enrollment. The median age of the per protocol population in the PICKUP study was 61 years, and 65.3% of patients were male.
2.3 Treatment ComparatorsThe following comparators were considered in this analysis:
All UC utilized a range of NI tests alongside invasive testing (including early bronchoscopy). All tests were administered (assumed to be at the same time) to patients, and then test results were received over time as they became available.
All UC & mcfDNA consisted of the All UC comparator described above with the plasma mcfDNA administered at the time of other testing.
NI UC & mcfDNA & conditional UC Bronch consisted of the plasma mcfDNA and NI tests administered at the outset, followed by further invasive tests and later bronchoscopy 5 days after the initial tests for patients who are negative in the initial tests. Note that prevalence and delay data from the PICKUP study were not collected specifically for this comparator. Therefore, data from the trial and other sources were combined to assess the potential cost-effectiveness of this comparator.
The turnaround time of test results and the ability to detect infectious ICHP etiology directly impact patient outcomes in the model. Before a test result is received a proportion of patients in the population will experience adverse outcomes (e.g., longer hospital stays, higher mortality risk) to reflect the presence of infectious ICHP etiology. After receiving the test results, similar adverse outcomes occur if the test misses the infectious ICHP etiology, leading to inappropriate treatment.
2.4 Time Horizon and Cycle LengthA lifetime time horizon (maximum age is 100 years old) initiated at the time of testing was implemented in the base-case analysis. A time horizon of 1 year was evaluated as part of scenario analyses. In order to parameterize the model using diagnostic delay data that is reported hourly (see Fig. 3), a cycle length of 1 h was used for the first 3 months of the analysis. Beyond the time span of the diagnostic delay data, in order to increase the speed and efficiency of the model, the time cycle was 3 months for the remainder of the first year, and 1 year from the second year onwards.
2.5 Discount RatesDiscount rates of 3% per year for benefits and costs were applied in the base case as per the Institute for Clinical and Economic Review reference case [17]. Additional scenario analyses evaluated outcomes for benefits and costs without discounting and with discounting at 5% per year.
2.6 Disease PrevalenceThe overall proportion of patients with relevant infectious ICHP etiology was informed by the test results in the PICKUP study and based on the All UC and All UC & mcfDNA comparators as shown in Fig. 2. In the All UC arm, an etiology of pneumonia was identified by All UC testing in 52 of 173 patients (30.1%). At time zero, the proportion of patients with ICHP microbial etiology in the model was 42.2% (73/173). Among these 73 patients, an etiology of pneumonia was identified by All UC alone in 25, All UC & mcfDNA in 27, and mcfDNA alone in 21. It was assumed that the comparators with mcfDNA eventually diagnosed all infectious ICHP pathogens, subject to delays to diagnosis or mortality.
Fig. 2
Infectious ICHP positive etiology identified in 173 patients. ICHP immunocompromised host pneumonia, mcfDNA microbial cell-free DNA, UC usual care
2.7 Appropriateness of TreatmentIt would never be the case that patients would knowingly be given inappropriate treatment. However, by comparing the testing results for UC and plasma mcfDNA, conclusions can be drawn as to the proportion of patients that may receive inappropriate treatment.
Appropriate treatment is defined here as patients that have received a test result and then receive treatment that is appropriate for an identified ICHP or non-ICHP microbial etiology. It is assumed in the base case that All UC & mcfDNA can detect all infectious ICHP pathogens.
Inappropriate treatment is defined as patients that receive a test result, but due to the shortcomings of testing, do not receive appropriate treatment for an ICHP or non-ICHP microbial etiology. A total of 21 out of 173 patients that would otherwise have been missed with UC testing were found to be positive for infectious ICHP etiology by plasma mcfDNA (Fig. 2). It is assumed in this study that a proportion of patients in the All UC arm may receive inappropriate treatment, leading to adverse outcomes. The proportion is informed by data (see Section 2.9).
The presence of relevant non-ICHP pathogens can also lead to some patients receiving inappropriate therapy. These pathogens are detected for all patients that receive plasma mcfDNA testing in addition to All UC (and therefore appropriately treated), but not for all patients in the All UC group. This proportion of patients at risk of inappropriate treatment was estimated based on the subgroup of patients in the PICKUP study for whom mcfDNA would have changed the choice of antimicrobial therapy (22/223, 9.9%) (manuscript under review).
Note that once patients receive a test result and have their treatment possibly modified as a result, no transitions between inappropriate or appropriate treatment states are possible.
2.8 Transition ProbabilitiesPatient transitions between model states per cycle were informed by data on the length of time spent in each state and the probability of patients experiencing an event.
2.8.1 Delays to DiagnosisTransitions between model states as test results are received (see flows from grey to white states in Fig. 1) were informed by data from the PICKUP study (manuscript under review), shown in Fig. 3. These data illustrate the proportion of patients identified with positive infectious ICHP etiology by test type over time. It was assumed that the time to either a positive or negative diagnosis was the same.
Fig. 3
Delays to diagnosis of infectious ICHP relevant etiology. All UC invasive and non-invasive usual care only, All UC & mcfDNA invasive and non-invasive usual care + mcfDNA, ICHP immunocompromised host pneumonia, I UC invasive usual care only, mcfDNA plasma microbial cell-free DNA, NI UC non-invasive usual care only
2.8.2 Probability of DiagnosisThe probabilities of diagnosis for each comparator over time were calculated by scaling each curve based on the maximum prevalence of an identifiable infectious ICHP pathogen. For example, the All UC & mcfDNA comparator is scaled to 100% as it is assumed that this test detects all relevant infectious ICHP pathogens. Based on the PICKUP study, the All UC comparator is scaled to 52/73 (i.e., number of patients with pathogen identified by All UC alone divided by number of patients with pathogen identified by All UC & mcfDNA). From the resultant curves, hourly transition probabilities for diagnosis were calculated using Eq. (1), where t is time (hours) and α is the value on the scaled diagnosis curve at time = t. Thus, the probability of diagnosis at 5 h is based on the difference in delay curve values at hours 4 and 5. As can be seen from the delay curves in Fig. 3, the curves are sometimes flat and the corresponding probability of diagnosis is zero.
$$_=1-\left(\frac_}_}\right)$$
(1)
As noted above, as data for the NI UC & mcfDNA & conditional UC Bronch scenario were not collected, assumptions about time to diagnosis must be made. The model assumed this delay curve followed the NI UC curve until the mcfDNA test delivered results, and then the curve increased based on the mcfDNA test. The curve then followed the invasive UC curve until the remaining infectious ICHP pathogen had been diagnosed. The scaled values, including the estimated NI UC & mcfDNA & conditional Bronch curve, are shown in Fig. 4. This has been scaled to the prevalence estimates in Fig. 2 combined with the delay curves in Fig. 3.
Fig. 4
Delay to diagnosis curves scaled to infectious ICHP prevalence estimates. All UC invasive and non-invasive usual care only, All UC & mcfDNA invasive and non-invasive usual care + mcfDNA, ICHP immunocompromised host pneumonia, I UC invasive usual care only, mcfDNA plasma microbial cell-free DNA, NI UC non-invasive usual care only, NI UC & mcfDNA—conditional UC Bronch non-invasive usual care + mcfDNA + conditional usual care bronchoscopy
2.8.3 Probability of Hospital Discharge and In-hospital MortalityThe probabilities of discharge from hospital and mortality in hospital (46/173) were calculated from data collected during the PICKUP study [10], which observed an average length of hospital stay of 22.2 days. These probabilities are defined in Eq. (2), where P is the probability of an event per unit time, l is the length of time spent in the state (e.g., time spent in hospital), and t is the time period of interest, depending on the length of the time cycle.
$$P=1-exp \left(-\frac\right) t$$
(2)
The final transition probabilities used in the model for discharge and mortality are summarized in Table 1.
Table 1 Discharge- and mortality-related transition probabilities2.9 Changes in Antimicrobial TherapyThe potential changes in ICHP antimicrobial therapy following the mcfDNA test results are shown in Table 2. In the PICKUP study, the adjudication committee determined that knowledge of mcfDNA results in real time would have led to changes in antimicrobial therapy in 11 of 21 patients (52%) with a microbial etiology exclusively identified by plasma mcfDNA sequencing. Were these changes in therapy not undertaken, it was judged that these 11 patients receiving treatment directed by All UC testing would have received inappropriate treatment leading to adverse health outcomes.
Table 2 Appropriateness of treatment2.10 Adverse Events Due to BronchoscopyBronchoscopy is associated with the risk of multiple complications. The frequencies of adverse events associated with bronchoscopy were sourced from the per protocol population in the PICKUP study and are presented in Table 3.
Table 3 Frequencies of bronchoscopy-associated adverse events2.11 Risk of MortalityMortality probabilities used in the model are summarized in Table 1. The probability of dying in hospital was sourced from the PICKUP study (26.5%, 46/173 patients), while the odds ratio (OR) for the reduction in mortality among patients with infectious ICHP treated with appropriate antimicrobials versus not (OR 0.35, 95% CI 0.24–0.51) was estimated in a recent systematic review by Bassetti and colleagues [18]. Post-discharge from hospital, the mortality rate is assumed to follow the age-specific values for the general population [19].
2.12 Health-Related Quality of LifeLife expectancy was adjusted for quality of life using health state utilities. QALYs were derived by multiplying remaining years of life by the utility value for each health state and an age specific utility value [20]. Several alternative secondary sources were considered in the estimation of the utility values (Table 4). In the case of disability weights, these values were multiplied by the health states for hematopoietic cell transplantation (a proxy for the broader patient population considered here) depending on the presence or absence of infectious ICHP. Disutility values for infectious ICHP modified the health state for hematopoietic cell transplantation by adding the values together (disutility is negative, leading to a lower value). The impact of using alternative sources was examined in scenario analyses.
Table 4 Health-related quality of life utility values.
Table 5 Disutilities of bronchoscopy-associated adverse events,
2.13 Cost InputsThe base-case model included multiple costs: test administration, treatment, treatment administration, health care resource utilization, readmission, adverse events, productivity loss, and mortality. Productivity loss costs were excluded in the base-case scenario [17]. All costs were inflated to 2023 USD when necessary [29]. In the absence of available information, a multiplier of 2.24 was used to estimate commercial costs [30]. For the All UC and All UC & mcfDNA comparators, test administration and associated testing costs (including bronchoscopy and adverse event costs) are incurred in the model as a one-time cost at time zero. For the mcfDNA and NI UC comparator, bronchoscopy cost is applied when negative results of the NI tests are received (informed by the delay curves, Fig. 4). Health care resource costs, including treatment and bed days, are allocated over time to all patients in the in-hospital model states. Readmission costs, reported as an average over 12 months, are applied as a one-time cost to all patients in the discharged state.
A comprehensive description of all cost inputs and their sources are provided in the electronic supplementary material (“Supplementary Information”), with a summary of the key cost parameters shown in Table 6.
Table 6 Summary of key costs2.14 Sensitivity AnalysesProbabilistic sensitivity analyses (PSA) were conducted to account for simultaneous uncertainty in the input point estimate values. To conduct the PSA, probability distributions were assigned to inputs based on realistic levels of parameter uncertainty, estimated from sourced standard error values where available. In cases where the parameter uncertainty was not described, the standard error was assumed to be 10% of the point estimate. Beta distributions were used for proportions, percentages, and utilities; log-normal distributions were used for numbers that ranged from zero to infinity, including costs; and the normal distribution was used for patient weight (shown in the main text and electronic supplementary material). A total of 2000 Monte Carlo iterations of the model were run, with input values for each iteration simultaneously randomly drawn from associated distributions.
2.15 Scenario AnalysesAdditional scenarios were explored to evaluate the effect on results when the model incorporated different time horizons, discounting assumptions, included costs, utility values, the effectiveness of the mcfDNA test in terms of appropriateness of treatment and reductions in mortality, and the price of the mcfDNA test.
留言 (0)