
記住我

The clinical characteristics of each patient with TA from each of the 11 families included in this study are displayed in Table 1. There were five males and six females, with ages ranging from 8 days to 29 years. None of the patients were related to each other, and none were born to a consanguineous couple. Intracardiac repair was completed in all but two infant patients (Patients 1 and 7). We identified putative biallelic pathogenic variants in TMEM260 in five patients, a de novo heterozygous pathogenic variant in GATA6 in one patient, and a de novo heterozygous probably pathogenic variant in NOTCH1 in one patient (Fig. 1, Table 1, Supplementary Table 1). Patients 1−3 harbored the biallelic c.1617del (p.Trp539Cysfs*9) variant in TMEM260. A compound heterozygous patient containing a c.1617del variant reportedly exhibited a SHDRA-like phenotype [10]. Patients 4 and 5 had other heterozygous pathogenic variants, c.332dup, p.(Thr112Hisfs*36) and c.1960C>T, p.(Gln654*), respectively, in addition to the heterozygous c.1617del variant. The p.(Gln654*) variant identified in Patient 5 was located in the last exon. This variant is expected to escape NMD but is expected to cause a loss of the end of the TPR domain, which is likely involved in substrate recognition and selective recruitment of IPT domains for O-linked mannose glycosylation (Supplementary Fig. 1) [8]. Additionally, the substantial loss of protein length can affect the stability of the protein. Therefore, we considered p.(Gln654*) to be a likely pathogenic variant. A de novo missense variant, c.1367G>A, p.(Arg456His), in GATA6 was identified in Patient 6. There have been reports of CHD patients with the same variant [28], and patients with TA or tetralogy of Fallot harboring p.(Arg456Cys) [28]. A de novo missense variant, c.545G>A, p.(Cys182Tyr), in NOTCH1 was identified in Patient 7. This variant has been reported in a large nonsyndromic tetralogy of Fallot cohort [29] although its pathogenicity has not been functionally evaluated. No additional potential pathogenic variants were identified in this study.
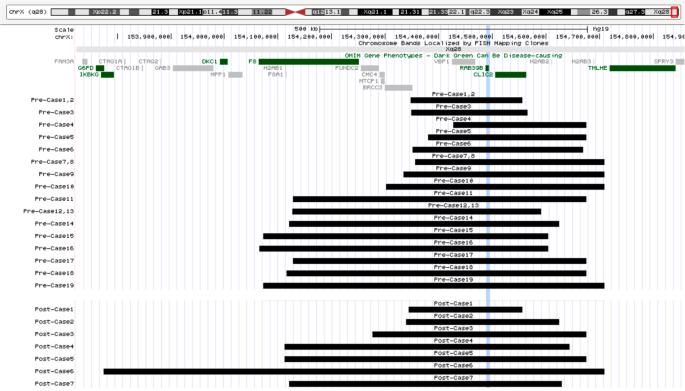
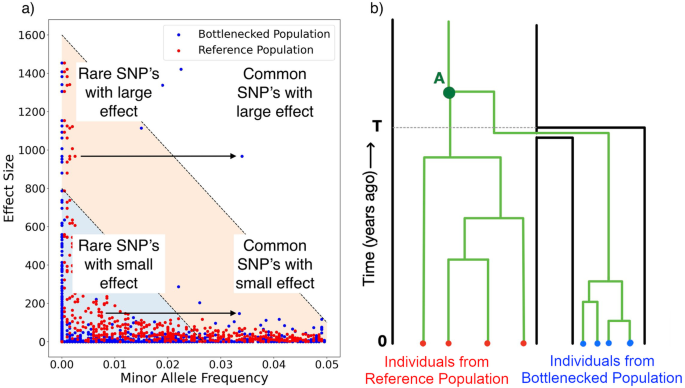
Fig. 1
Schematic of the gene structure of long isoform of TMEM260 (ENST00000261556.6) and short isoform of TMEM260 (ENST000005338838.1). The variants reported in this study (shown in bold and red) and the pathogenic variants have been published previously [8,9,10,11,12]
Among the five patients who had TMEM260 variants, regarding the types of TA, three were type I (Collett and Edwards classification) and type A1 (Vanpraagh classification), and two were type II and type A2 (Table 1). Other cardiac malformations included cor triatriatum and coronary artery fistula (CAF) in Patient 1, right aortic arch (RAA) in Patient 2, persistent left superior vena cava (PLSVC) in Patients 1 and 5, and partial anomalous pulmonary venous return (PAPVR) in Patients 1, 3, and 5. With regard to renal function, no chronic elevation of creatinine levels was observed in Patients 1 through 5. However, Patient 1 developed heart and renal failure after the palliative Rastelli procedure, requiring the induction of dialysis, was unable to withdraw from dialysis, and died. Patients 2–5 have not had renal dysfunction to date, although Patient 5 had hydronephrosis. Neurodevelopmental delay was present in Patients 2 and 4, although in Patient 2 it was unclear whether the delay was congenital or due to posthemorrhagic hydrocephalus. Hearing impairment was observed in Patient 2.
Among the six patients without pathogenic variants in TMEM260, two had TA type I and type A1, one had TA type II and type A2, two had TA type A3, and one had TA type III. There were no cases of renal dysfunction. Neurodevelopmental disorders were observed in three patients: Patient 6 had dysplasia of the cortical gyrus and language developmental delay, Patient 8 had post hemorrhagic hydrocephalus, and Patient 9 had hyperactive tendencies. Hearing impairment was observed in Patient 11. Patient 6 had no symptoms suggestive of pancreatic abnormalities, a common extracardiac feature of GATA6-related disorders [30].
We inhibited NMD using cycloheximide to test whether the c.1617del variant leads to NMD. The c.1617del (p.Trp539Cysfs*9) transcript was detected at much lower levels than the wild-type alleles in EBV-LCLs from the parents of Patient 1. Suppression of NMD by cycloheximide treatment increased the levels of frameshift transcripts. These results indicate that frameshift alleles led to unstable transcripts that were subject to NMD (Fig. 2).
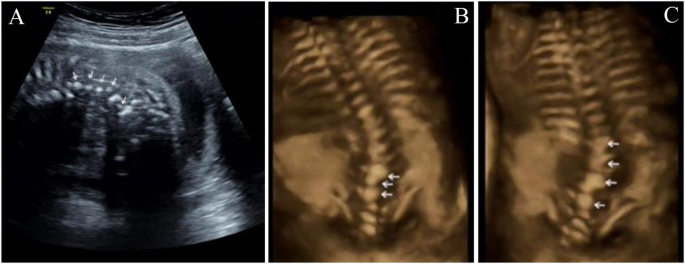
Fig. 2
The frameshift variant c.1617del in TMEM260 leads to NMD. EBV-LCLs from the parents of Patient 1 were treated with cycloheximide to suppress NMD. Sanger sequencing of the c.1617del variant was also performed. The red arrowheads indicate the location of c.1617del. The upper and lower panels show the results before and after CHX loading, respectively
In the Japanese population, the allele frequency of c.1617del was much higher (0.36%) than that in other populations (Table 2). Although less frequent than in the Japanese population, the allele frequency in the South Korean population was also elevated (0.14%; Table 2). In contrast, the variant was absent in the databases we analyzed for the Chinese, Taiwanese, Thai, and Vietnamese populations.
Table 2 Allele frequency of the c.1617del variant and estimated incidence of homozygous c.1617del variant in the Japanese and other populationsWe estimated the age of the c.1617del variant. The allele frequency in the haplotype dataset of 3,552 Japanese was 0.32% (23/7104 haploids). The genotype frequencies were 99.4% for the reference homozygous genotype and 0.6% for the heterozygous genotypes. No alternative homozygous individuals were identified in the dataset. The c.1617del variant occurred approximately 23 kiloyears ago (kya). This estimate did not change when the mutation rate was changed by a factor of 100 or 0.01 (22 kya for both 10–8 and 10–12). The estimate was also not significantly affected when the generation time was changed to 20 or 30 years (18 kya and 27 kya, respectively). These results suggest that the variant occurred at approximately 23 kya.
Among the 54,302 Japanese individuals participating in ToMMo 54KJPN, the data on serum creatinine, BUN, and uric acid were available for 38,207 individuals, and serum cystatin C was available for 38,206 individuals. Of these, 274 had the c.1617del heterozygous variants. There were no significant differences between individuals with heterozygous c.1617del variants and those with the wild-type allele in any of the above indices (Supplementary Fig. 2). Data on the presence of CHD were available for 13,508 individuals, of whom 88 were heterozygous for the c.1617del variant. None of the heterozygous c.1617del individuals had CHD. None of the individuals in the ToMMo 54KJPN cohort were homozygous for the c.1617del variant.
留言 (0)