The study population consisted of children born in 1995–2004 identified from the longitudinal population register of Statistics Finland. This individual-level register contains annual information on the full population residing in Finland with linkages between biological family members, allowing identification of parents and full siblings. The data were linked with individual-level information on medication purchases from the national prescription register maintained by the Social Insurance Institution of Finland [19], as well as information on the mode of delivery from the Medical Birth Register.
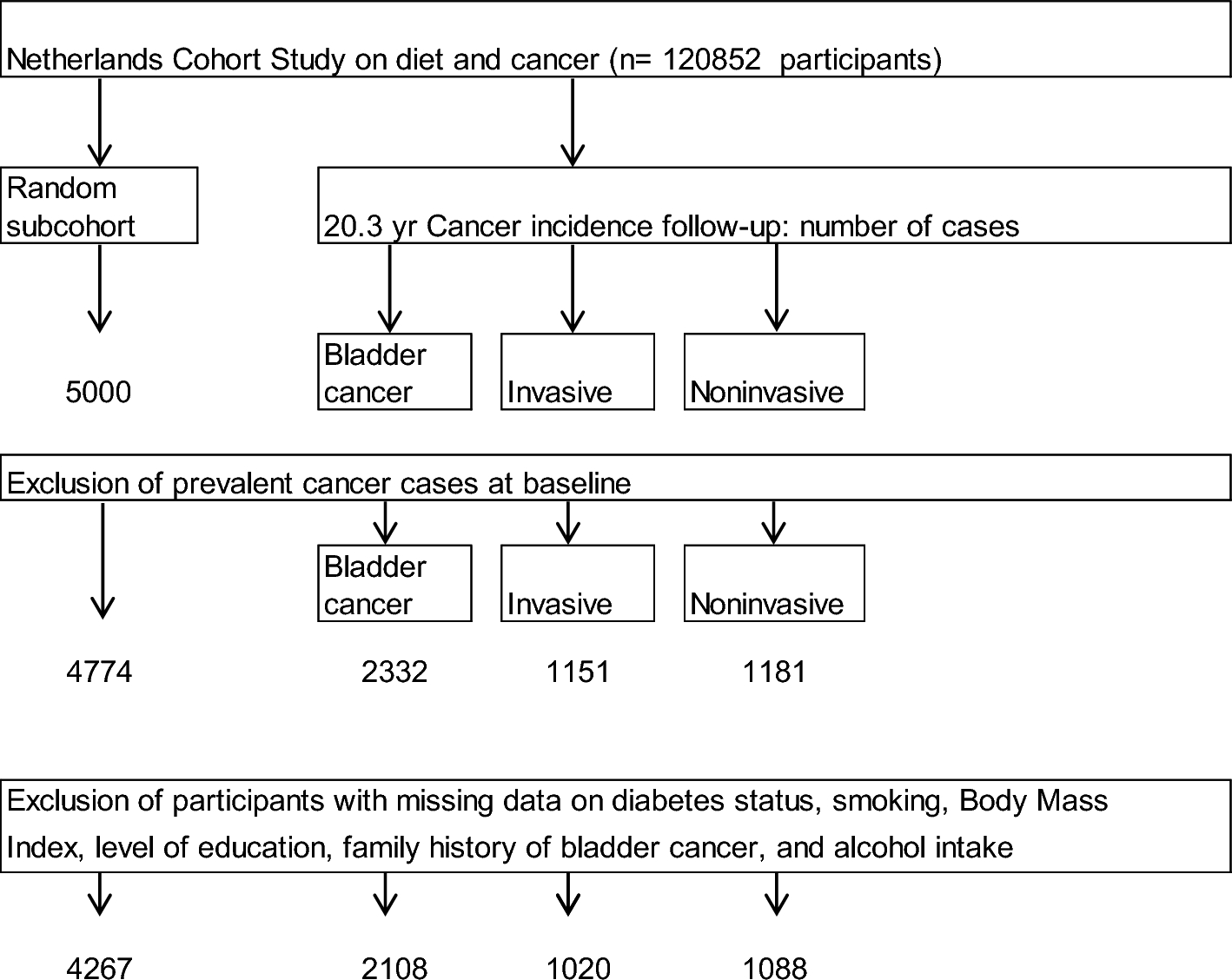
We included individuals present throughout ages 0–15 (N = 559,077), excluding those who emigrated (n = 20,015) or died (n = 3,275). In the within-family analyses of birth order, we restricted the sample to children with at least one full sibling to compare with (N = 324,306) and in the age-difference analyses we only included first-borns (N = 266,876).
Outcome: atopic medication purchases
We used reimbursed purchases of prescription medications as measures for common childhood atopic diseases: allergic rhinitis, allergic eczema, asthma, and severe allergic reactions. All residents of Finland are entitled to partial reimbursement for prescription-issued medication, provided directly at pharmacies [19]. The medications were identified and categorised according to the Anatomic Therapeutic Chemical (ATC) classification (Table 1).
Table 1 Medication measuring different atopic diseasesNot all medications used for atopic diseases were captured by our data, as purchases of over-the-counter antihistamines and eczema medication as well as few of the prescription-only products are not reimbursed. However, there is a clear incentive to obtain a prescription and reimbursement in cases of long-term need, or need of more potent medication. All asthma medication require a prescription and are reimbursed [20]. In sensitivity analyses, we also used special reimbursement rights that are granted for individuals with chronic asthma confirmed with a medical evaluation including pulmonary function tests [21] as an additional measure for asthma. All Epinephrine medication also require a prescription, and a vast majority of products are reimbursed [20].
We measured purchases of each medication type with an indicator for at least one purchase by the end of the calendar year the child turns 15 years. In sensitivity analyses we used higher cut-points of having atopic medication purchases in > 1, >2 and > 3 years between ages 0–15.
Exposures: birth order and age difference
Sibling information was based on biological full siblings. In 2018, roughly 10% of Finnish children lived in families with half or step siblings [22]. As our measurement ignores the presence of other than full siblings, we also ran a sensitivity analysis among children who lived with both their biological parents without any step- or half-siblings between ages 0–15.
Birth order and family size
Birth order was classified as 1, 2, 3, 4+. Family size measured the number of biological children of the same parents, classified as 1 (only child), 2, 3, 4+. To assess birth order in families of different sizes, we also constructed a categorical variable measuring both birth order and family size: only child (#1/1), first-born of two siblings (#1/2), second-born of two siblings (#2/2) and so forth until fourth-born or later of four or more biological children in the family. Both family size and birth order were based on information on all siblings born alive by the time the index child was 15 years old.
First-born child’s age difference with second-born sibling
The age difference between the first and second-born siblings was rounded to the nearest full year with categories ranging from one to five or more years. We also included separate categories for twins, with no age difference, and only children. It should be noted that twins have an increased asthma risk due to shorter gestational age [23, 24], but to our knowledge, a similar relationship has not been documented with other atopic diseases. As a sensitivity analysis, we also assessed the second-born child’s age difference to their third-born sibling.
Observed confounders
We controlled for a number of important observed confounders measured in the year of birth unless otherwise specified. Model 1 controlled for sex and birth year of the child, and parental immigrant status (at least one parent born abroad), all important risk factors for atopic diseases [25].
In Model 2, we added controls for characteristics of the child’s place of residence at time of birth. Geographical area dummies (NUTS3 regions) controlled for potential regional differences in access to healthcare and prescription practices. We also controlled for the level of urbanicity, as less biodiverse and more polluted urban environments have been associated with increased rates of asthma and allergies as opposed to rural environments [16, 17]. This urban-rural classification by the Finnish Environment Institute is based on a 250 × 250 m grid that takes into account population density, building density and development and land use. It consists of seven categories spanning from inner city to sparsely populated countryside [26].
In Model 3, we added controls for household socioeconomic position: highest parental education (basic, secondary, or tertiary) and household income decile based on annual disposable income per household consumption units. These variables control for possible socioeconomic differences in the quality of housing, treatment seeking behaviour and affordability of medication.
Finally, in Model 4, we further controlled for the mode of delivery (Caesarean section vs. other), to address the higher likelihood of Caesarean sections among first-born children. We also controlled for parental atopic medication purchases (no vs. at least one purchase between offspring ages 0–15) as separate dummies for each medication type to address genetic liability for atopic diseases. Parents with experience of atopic diseases may also be more likely to seek treatment for their children.





留言 (0)