From the several articles regarding case reports and related review articles, the possible contributing factors of relevant PIOM could be summarized as: (1) dental implant corrosion and possible association between corrosion products and SCC; (2) the possible association between particulate titanium and SCC; (3) migration of malignant cells through the implant surrounding sulcus; and (4) the hypothesized carcinogenic effect of sustained metallic ion release after implant placement [7, 11, 12].
Commercial pure titanium (CP-Ti) or a Ti6Al4V alloy could deteriorate from the surrounding medium attachments causing electrochemical or galvanic currents, leading to the possible association between corrosion product release and SCC. This hypothesis could be accepted especially in failing or failed implants, which may occur in many cases of PI [13]. Titanium ions are well-known to be one of the most inert metallic ions with a very low corrosion rate of 0.003 μA/cm2 [14]. Particulated implant debris could result in inflammation round orthopedic implants. Therefore, inflammatory factors such as eicosanoids, collagenase, interleukin-1, and prostaglandin E-2 could lead to implant bursitis and bony resorption [15, 16]. Dental implant placement is a type of entrance for malignant cells and this migration through implants contacting the gingival sulcus has also been suggested for PIOM.
From these three hypotheses, the carcinogenic effect of metallic ion release has been suggested in a more detailed way and is divided into three separate issues including: (1) the carcinogenicity of the metallic ions; (2) exposure level to the patient; and (3) incidence of cancer in patients treated with implants [17,18,19]. Adding to the corrosive carcinogenicity of titanium ions, the exposure level to the patient would be dependent on the surface area of the implant and exposed time duration. The number of implants should be considered for these suggestions, and although it is difficult to establish a threshold of how many implants would constitute a significant total surface area, the only conceivable situation where a significant surface area would exist would be in patients with multiple implants. Unlike several case reports which were related to only a single implant, our retrospective results revealed that only two cases of patients No. 12 and 20 possessed a PIOM surrounding the upper first molar. Otherwise, the 19 other cases of PIOM were all multiple implant cases between two to five implants (Table 1). Our results could support the hypothesis that PIOM would be observed relating to patients with multiple implants where the exposed surface area and incidence would be higher. Unfortunately, the direct carcinogenic role of dental implants has yet to be established, but just hypothesized or proposed by several clinicians.
Although dental implants have seen tremendous clinical success over the last few decades, there are some worrying reports in literature describing SCC in close association with dental implants. This article also provides a critical assessment of the published literature relating to the presence of carcinomas in association with dental implants, analyzed previously published and hypothesized carcinogenic responses to an implant, and attempted to come to a conclusion regarding the plausibility and clinical risks for cancer formation in association with dental implants [2, 4, 7, 9, 20, 21].
An unusual case of an SCC noted in close proximity to a dental implant is also presented. A systematic search was conducted using Medline (PubMed), Cochrane Database, and Google Scholar with the search terms "cancer", "squamous cell carcinoma", "dental implant", "SCC", "peri-implantitis", "oral cancer", and "implantology" using multiple combinations with the boolean operators "or" and "and". The search was not limited to dental literature—orthopedic and biomedical literature were also included.
The results were then screen to locate relevant articles. In total, 14 previous published reports were found, where 24 dental implants were reported to be associated with SCC. Not all the reported patients had a history of cancer, but contributory factors such as smoking were observed. An analysis of the biological plausibility of previously proposed carcinogenic mechanisms such as corrosion, metallic ion release, and particulate debris did not support the etiologic role of dental implants in cancer development. PI must be assessed cautiously in patients receiving implants who have a previous history of cancer. Dental implants are a safe treatment modality based on the published data, and any changes in the surgical protocol are not mandated.
The sex ratio of PIOM was balanced as male 1.625 to female 1.0, which could be compared with the general OSCC ratio of 1.43 to 1.0. Individual living patterns including habits, occupation, foods, and oral hygiene must be supported for this gender ratio difference.
Both alcohol and tobacco consumption were observed in three patients who exhibited very low proportions of classical risk factors of OSCC. As previous report of upregulation of the interferon-γ and nuclear factor kappa B in risk factor studies of nonsmokers and nondrinkers demonstrated [9, 22], different carcinogenesis of PIOM could be suggested in the point of typical “smoking and alcohol” risk patterns. Among our cases, three patients had a history of previous cancer treatment. This is also a lower proportion compared with other previous reports.
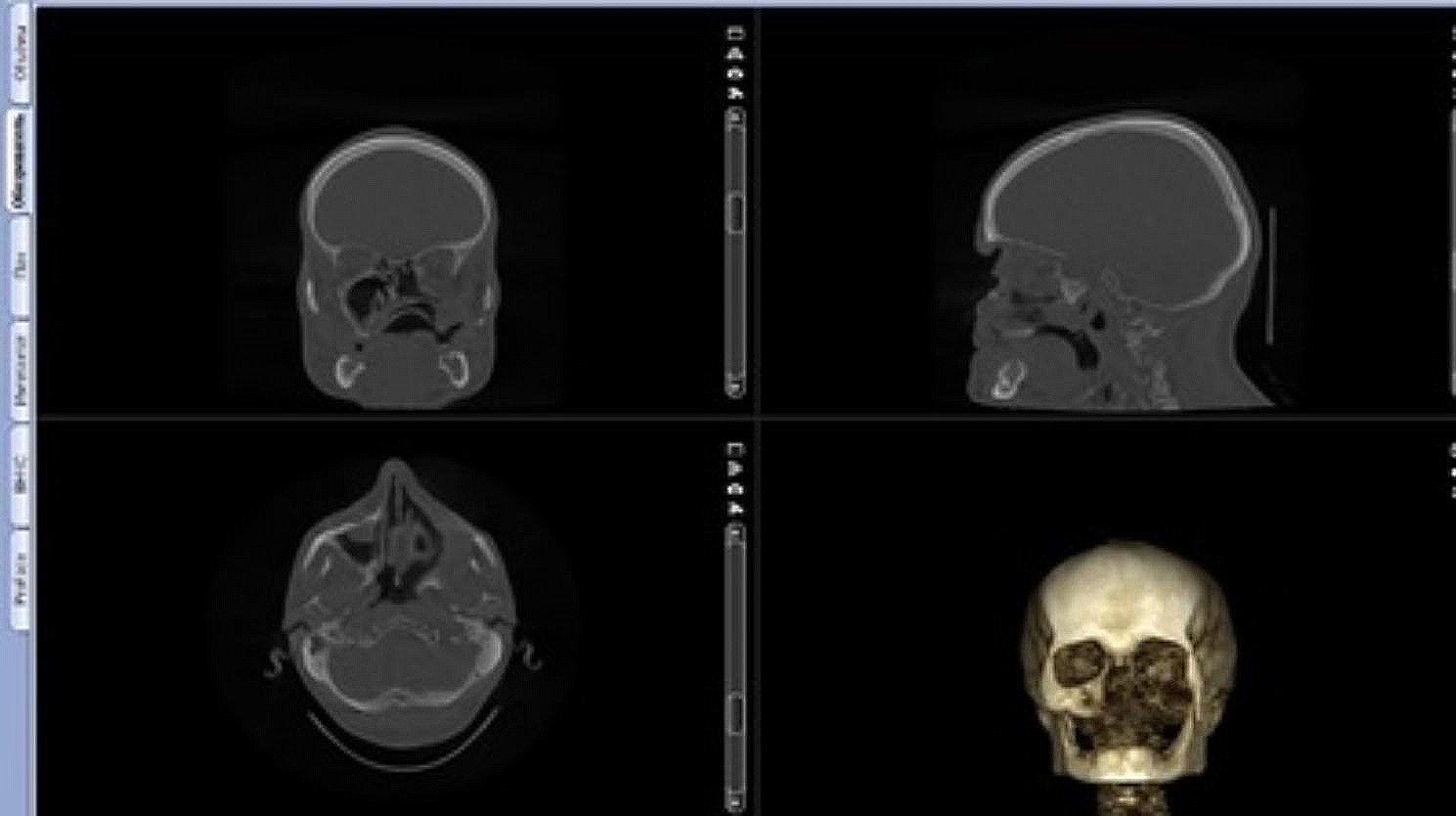
The most common clinical feature was an exophytic mass with ulceration around the implants, followed by an exophytic mass without ulceration. All patients were treated for PI before diagnosis, and routine dental radiography was not a valuable criterion for differential diagnosis. In panoramic or periapical view, the incidence of observed marginal bone loss was 61.9% of the total cases. Buccal bone loss was frequently noted in the CT, it may not manifest in the bone levels at the peri-implant fixture on the distal and proximal side. Furthermore, it is believed that PIOM is characterized by an exophytic growth pattern, influencing clinical features. Additionally, when bone destruction around implants is irregularly evident on CT scans, it may not be apparent in plain film imaging. The use of plain film for measurements has limitations in reflecting the level of marginal bone loss, and CT scans are challenging due to metal artifacts. In this study, only 61.9% demonstrated marginal bone loss, but all patients had a history of previous diagnosis and treatment for PI including debridement.
In the differentiation of tumors, well-differentiated SCC was the most common type. In patients excluding one case of melanoma, the 5-year survival rate was 80% with 75% of the patients being stage IV, and patients with bone involvement accounted for 75% of advanced stage surgery, which exhibited good prognoses. 85.71% of PIOM patients had prostheses containing metal components and not natural teeth. 72.2% of opposing prostheses were made of PFM. Although the PIOM patient group have a relatively low risk factors, we carefully speculate that the galvanic currents formed by contacting various types of metals may have contributed to the occurrence of PIOM. Additional research is needed to support this thesis.
There is a debate regarding whether malignant changes occur in PI or if the manifestation of PIOM presents signs similar to PI. The question arises regarding whether the existence of dental implants poses a risk for malignancy. PI is characterized by persistent and prolonged inflammation. Chronic inflammation has been associated with malignant transformations in various types of cancers, as seen, for example, in patients with Crohn's disease developing colon cancer [11]. If inflammation persist, it can have sufficient potential to induce cellular proliferation and prolong cellular survival by activating the oncogenes and inactivating tumor suppressor genes, which would produce genetic instability and a greater risk of having cancers [23]. The concentration of titanium particles increases significantly at PI sites. However, it remains unclear whether this phenomenon also trigger inflammation and bone resorption [24]. As of now, there is no established association between the occurrence of dental implants and OSCC [23, 25].
Based on the review of these cases, it can be deduced that there is a possibility that implants and galvanic currents between different prostheses may constitute an irritant and/or inflammatory cofactor contributing to the formation and/or development of OSCC. Basic research is needed to establish a clear cause–effect relationship. The incidence of carcinomas next to dental implants is low but may attain clinical relevance with increasing dental implant treatment. Patients at risk potentially profit from individualized recall intervals and careful evaluations.
It is essential to perform a delicate oral cavity examination before implant treatment, and the patient’s risk factors of SCC must also be managed and controlled with strict follow-up protocols. Appropriate regular check-ups for the patients with risk factors must be conducted, and histopathologic biopsy examinations should be performed as soon as possible on any questionable lesions. Although frequent biopsies of every case of PI would not be justified, clinical PIOM resembling cases including hyperplastic papillomatous gingival growth or whitish alveolus covering the gingiva should be promptly biopsied promptly. During this strict periodic follow-up period, high-resolution self-photos with individual mobile phones could be an alternative for frequent visits to the clinics. Fortunately, most of our represented PIOM cases were recognized clinically, thus if patients had been educated properly, each patient could regularly send his or her intraoral photos to the specialized clinics. However, in order to elucidate the precise pathogenic mechanism involved in each of these disease processes, additional molecular genetic investigations should be performed.





留言 (0)