
記住我



We analyzed medical records, postoperative radiographic findings, and histological results of patients with jaw bone atrophy who underwent alveolar ridge augmentation in the maxilla or mandible between January 2018 and March 2022 at the Oral & Maxillo-Facial Care Clinic, Yokohama, Japan, in preparation for receiving dental implant therapy. A total of 30 patients agreed to participate in this study and underwent or did not undergo ASC grafting for lateral bone defects. Patients were treated by bone augmentation with bone substitutes alone (carbonate apatite, CO3Ap; Cytrans®Granules) [15] (ASCs− group, n = 20) or with bone substitutes plus ASCs (ASCs+ group, n = 10). In both groups, patients with lateral jaw bone defects with fewer bone walls underwent horizontal and vertical lateral bone augmentation. In all cases, guided bone regeneration was performed in patients with similar bone defects of similar morphology. Patients with relatively extensive bone defects who required autologous transplantation of non-oral bone but agreed to treatment with the new approach to avoid autologous bone transplantation underwent bone augmentation with bone substitutes with ASC transplantation (Fig. 1). Other patients underwent conventional bone augmentation with bone substitutes without ASC transplantation. Patients excluded from alveolar ridge augmentation were those with systemic diseases that affect bone regeneration, such as diabetes, and those who were heavy smokers.
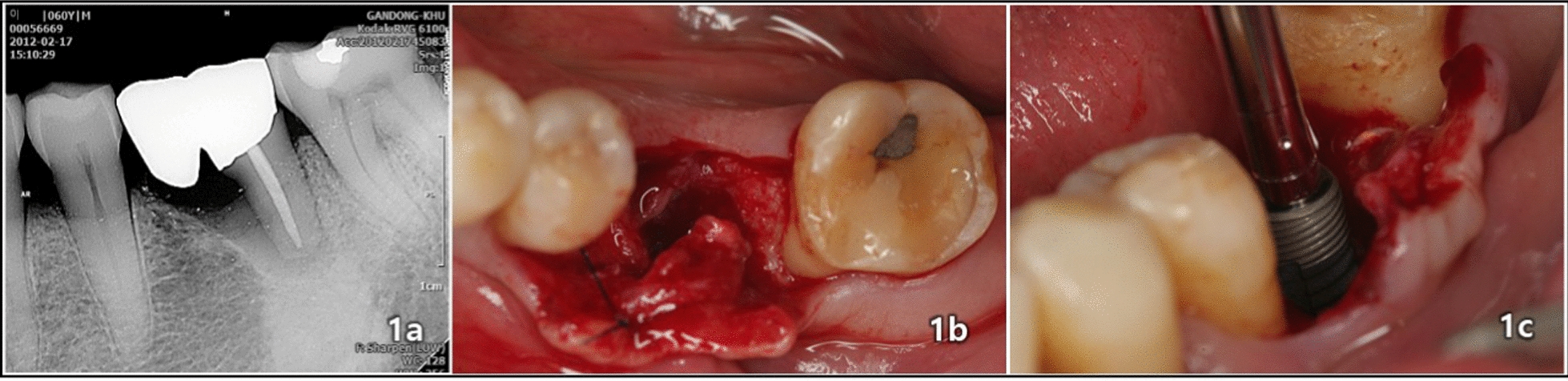
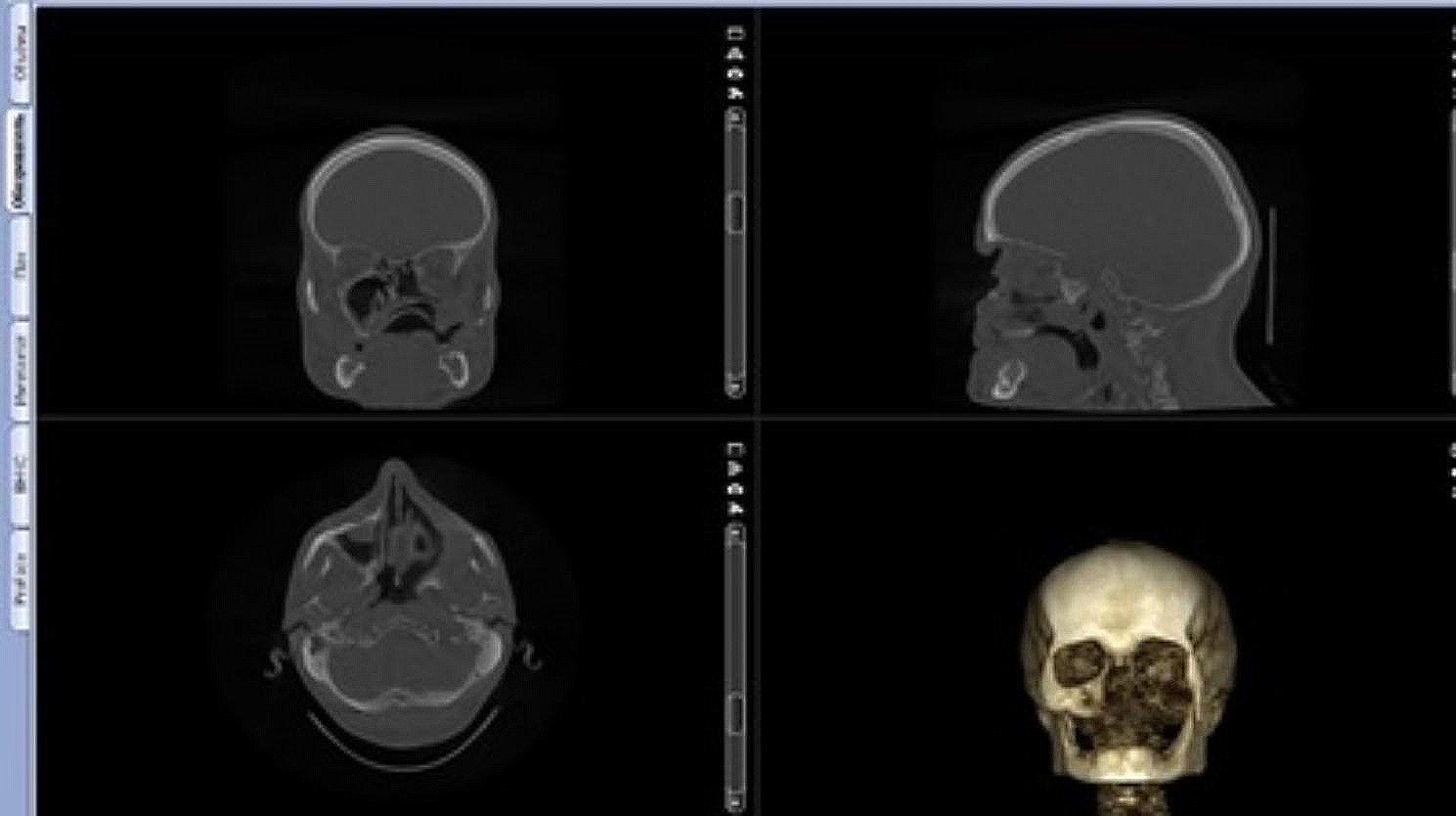
Fig. 1
Representative findings in a patient with a jaw bone defect with bone substitutes (carbonate apatite) mixed with adipose stem cells. a Computed tomography image of a patient with extensive lateral bone defects in the jaw as representative findings of patients in the group treated with bone substitutes (carbonate apatite) mixed with adipose stem cells. b Extensive severe maxillary atrophies and defects. c Lateral bone defects with horizontal and vertical bone atrophies in anterior teeth
Exclusion criteria for this retrospective evaluation included being considered ineligible for participation because of the medical history, for example, and deciding not to participate after the study content was posted in the hospital.
This retrospective study was approved by the ethical review board of Tokyo Dental College on June 24, 2022 (medical ethical review number: 1118). Participants provided written informed consent for their data to be included in the study.
Bone augmentation procedurePatients in the ASCs+ group underwent bone augmentation with CO3Ap mixed with ASCs and filled with AFG; this treatment is certified as a type 2 regenerative medicine to be provided under the Act on Securing Safety of Regenerative Medicines in Japan (certification no. PB3170030). Patients in the ASCs− group underwent bone augmentation on the alveolar ridge with CO3Ap alone and filled with AFG.
To obtain ASCs, liposuction was performed by a plastic surgeon. First, under general anesthesia an adequate amount of tumescent solution (anesthetic solution: lactated Ringer’s solution 500 mL + 1% lidocaine 20 mL + 1 mg epinephrine) was infused into the subcutaneous adipose tissue at the adipose tissue harvest site (abdomen or thigh). Approximately 30 min after infusion of the solution, a suspension containing adipose tissues was manually aspirated with a dedicated syringe and cannula.
After removal of the adipose tissue (100 to 250 mL; mean, 171 mL), the tissue was washed with lactated Ringer’s solution, and ASCs were separated from adipose tissue with a Celution 800/CRS device (Cytori Therapeutics, Inc., San Diego, CA, USA). After separation, the cell suspension containing ASCs (about 5 mL) was extracted with a centrifuge (Fig. 2). A small amount of the cell suspension was used for assessment of cell viability and measurement of the number of living cells with a Nucleocounter NC-100 (ChemoMetec A/S, Allerod, Denmark). The optimal characteristics for cell transplantation therapy were set as a cell viability of 70% or higher and a minimum concentration of living cells of 1 × 106/5 mL [9].
Fig. 2
Extraction of adipose stem cells from harvested adipose tissue. a A plastic surgeon harvesting adipose tissue (100 to 200 g) by liposuction. b Harvested adipose tissue. c Celution 800/CRS device (Cytori Therapeutics, Inc., San Diego, CA, USA), which was used to extract adipose stem cells from harvested adipose tissue. d Cell suspension containing extracted ASCs (about 5 mL)
Jaw bone augmentation in the maxillary and/or mandibular alveolar ridges was performed by an oral surgeon. Bone augmentation was performed by transplanting a graft with bone substitutes mixed with ASCs (ASCs+ group; Fig. 3) or not (ASCs− group) and further filled with AFG.
Fig. 3
Bone augmentation on the alveolar ridge with grafts mixed with adipose stem cells and bone substitutes (carbonate apatite). Extracted adipose stem cells (ASCs) were mixed with bone substitutes (carbonate apatite) (a) and bone augmentation was performed at sites 13 to 11 and 21 to 23 with grafts mixed with ASCs (b, c)
Evaluation of bone regenerationIn both the ASCs+ and ASCs− groups, a dental cone beam computed tomography (CT) scan was performed approximately 6 months after bone augmentation to confirm bone regeneration (Fig. 4). Then, an oral surgeon performed dental implant placement (Fig. 5). After approximately 6 months, a screw-retained prosthesis was installed (Fig. 6).
Fig. 4
Cone beam computed tomography findings immediately after bone augmentation with adipose stem cells and bone substitutes (carbonate apatite). Three-dimensional image (a) and frontal plane image (b) 6 months after bone augmentation showing high gray scale values of bone augmentation
Fig. 5
Panoramic X-ray image after implant placement. Six implants were placed in augmented bone
Fig. 6
Screw-retained prosthesis. The prosthesis was installed approximately 6 months after placement of implants into the augmented bone
To evaluate the change in the amount of regenerated bone around the site of the dental implant, the height of the augmented bone was measured during the immediate postoperative period after bone augmentation and at 6 months postoperatively from CT images. The height of the augmented bone was measured at the site about 1 mm horizontally from the implant site, and the mean height was calculated. The bone survival rate was calculated from the height of the augmented bone during the immediate postoperative period after bone augmentation or at 6 months postoperatively.
To measure the bone density around the dental implant site, gray scale (GS) values were measured in the cone beam CT scan during the immediate postoperative period and at 6 months postoperatively. Measurements were made at 3 points on the same horizontal plane, 1 mm, 3 mm, and 5 mm from the implant site, and vertically from the existing bone on the alveolar ridge, and the means were calculated.
The cone beam CT system was ProMax 3D Mid with Romexis Ver: 4.6.2 software (Planmeca, Finland). The measured GS values were the values displayed as the mean of the Hounsfield Unit reference values in the 3 × 3 pixel range on the screen. The parameters of the CT image GS were as follows: bit number, 15; window, 2500; level, 2500.
Metal artifacts around the implant body are problematic when measuring GS values. Therefore, GS values were measured at a distance of 1 mm horizontally from the implant body after artifacts were removed by image processing with the Romexis Ver. 4.6.2 software of the cone beam CT system.
On the other hand, although GS values are a valid way to evaluate images because they measure the intensity of displayed pixels, it is difficult to use them to accurately evaluate the quality of the jawbone. Therefore, the quality of the regenerated bone was evaluated histologically.
Six months after bone augmentation, a CT image of the maxilla was obtained (Fig. 7a, b) to assist in harvesting a trephine bur (Fig. 7c, d) as an augmentation specimen for histological analysis as part of the treatment. The removed bone tissues were fixed with 4% paraformaldehyde-phosphate buffered saline (PBS, Nacalai Tesque, Inc., Kyoto, Japan) for 1 week and then decalcified with 0.5 M ethylenediaminetetraacetic acid (Dojindo Laboratories, Kumamoto, Japan)-PBS (pH 7.2) for 4 weeks. Subsequently, the decalcified bone tissues were cut into two pieces along a longitudinal axis and embedded in a paraffin block. Then, the paraffin blocks were cut into 4-μm-thick slices, mounted on a slide glass, and stained with hematoxylin and eosin (HE). Photographs of the HE-stained specimens of augmented bone areas were captured with a fluorescence microscope (BZ-9000, Keyence Corporation, Osaka, Japan) under normal and fluorescent (excitation, 470/40 nm; emission, 525/50 nm) light. Under fluorescent light, bone tissue areas were selectively brighter than the background [16]. The total area (T.Ar) and bone area (B.Ar) [17] were measured with ImageJ, and histological bone density was calculated as B.Ar/T.Ar (%) [18].
Fig. 7
Computed tomography images of sites where augmented bone was harvested. During implant placement 6 months after bone augmentation, 3-dimensional (a) and sagittal plane (b) computed tomography images of bone harvest sites were used to assist harvesting of augmented bone with a trephine bur (c) at the site related to tooth number 13. The bone harvest site is the blue circle in a and c and blue bar in b. Harvested augmented bone (d)
Statistical analysisNormality and homoscedasticity were analyzed before statistical analyses were performed. To compare two groups or conditions, we used the Mann–Whitney U test, and to compare three groups or conditions, we used the Kruskal–Wallis H test and confirmed the results by the Mann–Whitney U test with Bonferroni correction. All statistical analyses were performed with ystat2013 (an Excel® statistical program file, which was programmed by Dr. Yamazaki, Ohu University, Fukushima, Japan). Results are presented as means. P values of less than 0.05 were considered statistically significant.
留言 (0)