Study design and data collection
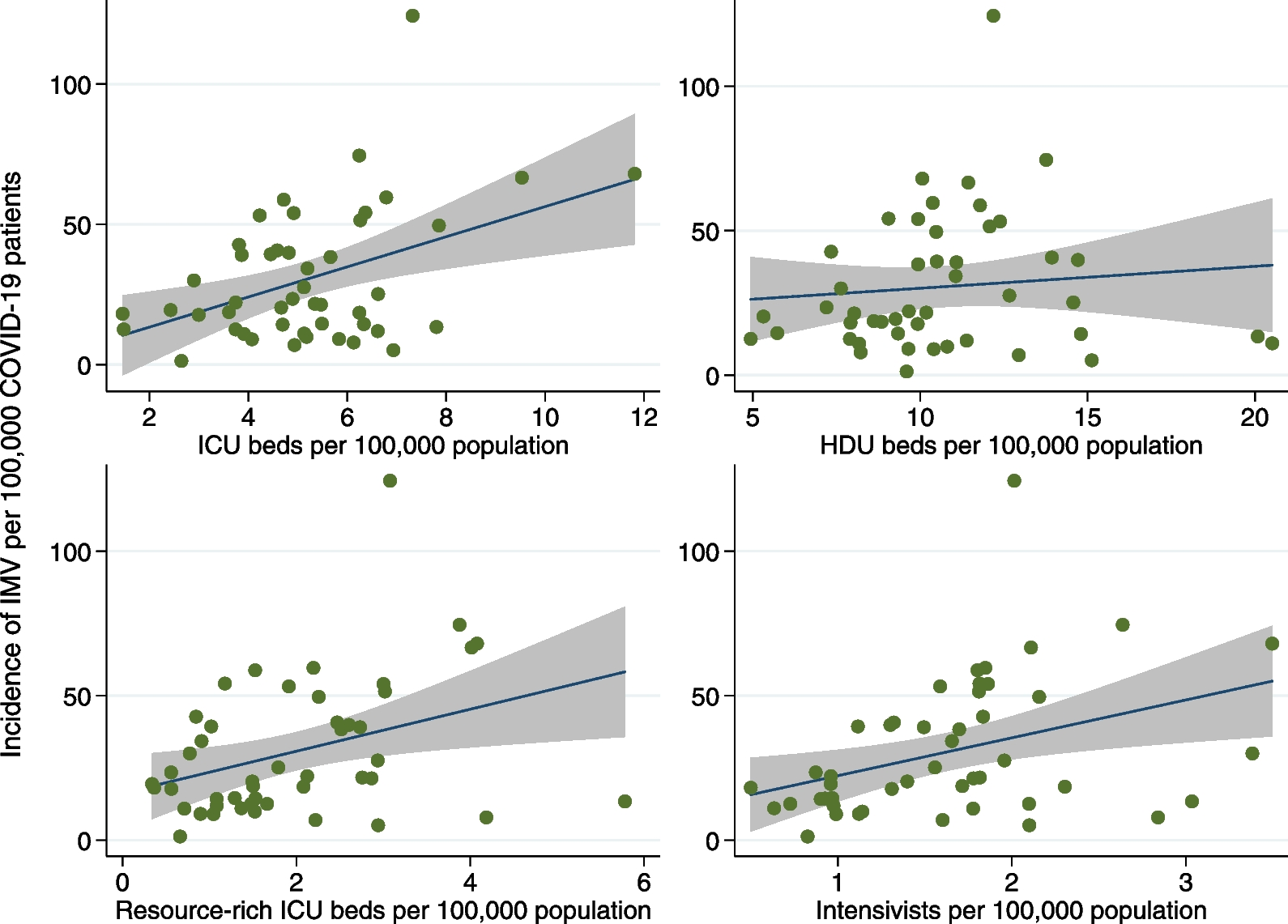
We aimed to evaluate the association between regional critical care capacity and the incidence of IMV for COVID-19 patients in Japan. This population-based cohort study included all Japanese citizens. The data used in this study were obtained from three sources: (i) CRoss Icu Searchable Information System (CRISIS) database; (ii) publicly available databases provided by the Japanese government; and (iii) published data from the Japanese Society of Intensive Care Medicine.
The CRISIS database was developed by Japan ECMOnet for COVID-19 to accurately track real-time information from ICUs across Japan during the COVID-19 pandemic from February 2020 [20,21,22,23]. Participation in the CRISIS database was voluntary for hospitals; however, most hospitals certified by the Japanese Society of Intensive Care Medicine and Japanese Association for Acute Medicine participated initially. Hence, there were 666 participating hospitals with 6186 ICU beds and 10,058 HDU beds in the database as of March 31, 2023. As of July 2020, participating hospitals comprised 86.7% of all the ICU beds (6,181/7,132 beds) and 71% of all the HDU beds (10,058/13,546 beds) in Japan, indicating that most hospitals with critical care beds in Japan participated in the CRISIS database. Participating hospitals were requested to register all COVID-19 patients who received IMV and extracorporeal membrane oxygenation (ECMO) in the CRISIS database. In the CRISIS database, COVID-19 patients were defined as those with a positive severe acute respiratory syndrome coronavirus-2 polymerase chain reaction test result and pulmonary involvement typical of COVID-19. The CRISIS database collected data on the number of patients who received IMV and ECMO, hospital characteristics, patient background (age, sex, and body mass index), start and end days of IMV and ECMO, and mortality.
Three publicly available databases from the Japanese government were used: trends in newly confirmed COVID-19 cases [24], Survey of Medical Institution 2020 [25], and Japanese Population Estimates 2020 [26]. The number of newly confirmed cases is provided by the Ministry of Health, Labour and Welfare, Japan, and is calculated based on the Health Center Real-time Information-sharing System on COVID-19 (HER-SYS) database [27]. HER-SYS allows information to be shared instantly among local public health centers, prefectures, municipalities, medical institutions, and other relevant parties. In the HER-SYS database, newly confirmed cases of COVID-19 were defined as those diagnosed with COVID-19 by physicians, regardless of the diagnostic method. The number of newly confirmed cases, including recurrent positive cases in each prefecture, is calculated by summing the cases published through press releases. The Survey of Medical Institutions 2020 is provided by the Ministry of Health, Labour and Welfare, Japan, and includes facility information and statistics on all hospitals in Japan as of July 1, 2020. The Survey of Medical Institutions included data on the types of wards (e.g., ICU, HDU, and resource-rich ICU) and the number of beds in each ward for 47 prefectures in Japan. The Japanese Population Estimates 2020 is provided by the Ministry of Internal Affairs and Communications. The annual estimates of “population by age (5-year groups) and sex for prefectures” as of October 1, 2020, were used in this study.
The number of intensivists certified by the Japanese Society of Intensive Care Medicine in each of the 47 prefectures as of April 1, 2021, was obtained using data published by the Japanese Society of Intensive Care Medicine [28].
Study and patient populations
The patient population included COVID-19 patients diagnosed between February 1, 2020, and March 31, 2023, as recorded in the HER-SYS and CRISIS databases. Patients with missing data on age at admission or sex in the CRISIS database were excluded. All eligible patients in the CRISIS database were followed up until death, hospital transfer, or hospital discharge.
Regional critical care capacity
The variable of interest in this study was the regional critical care capacity of 47 prefectures in Japan. Prefectures in Japan are administrative divisions similar to those in the United States, and medical plans stipulate the formulation of critical care capacity systems at the prefectural level. To assess regional critical care capacity, we used four indicators: (i) numbers of ICU beds, (ii) HDU beds, (iii) resource-rich ICU beds, and (iv) board-certified intensivists per 100,000 individuals. The numbers of ICU beds, HDU beds, and resource-rich ICU beds were obtained from the Survey of Medical Institutions 2020, and the number of intensivists was obtained from published data from the Japanese Society of Intensive Care Medicine. When calculating these indicators, the population of each of the 47 prefectures was standardized to the total population in 2020 based on age (5-year groups) and sex.
Definition of critical care beds
In Japan, the ICU is defined as a separate unit providing critical care services with at least one physician onsite 24 h per day; full-time, around-the-clock nursing; equipment necessary to care for critically ill patients; and a nurse-to-patient ratio of 1:2 [1, 29]. The term “ICU” includes all ICU types, including medical, surgical, medical-surgical, emergency, neuro, cardiac, and pediatric ICUs. An HDU, also called an “intermediate care unit” or “step down unit”, is defined as an area where critical care services (mechanical ventilation and vasopressor administration) are provided, with patient care levels between those of the ICU and the general wards [30, 31]. In this study, the HDU differed from the ICU because it had a nurse-to-patient ratio of 1:4 or 1:5 and did not require intensive staffing [29]. Among the ICUs defined previously, a resource-rich ICU was defined as ICUs with two or more intensivists working as full-time employees, ≥ 20 m2 per ICU bed, and a medical engineer in the hospital 24 h per day [32]. The medical reimbursement for resource-rich ICUs is 1.5 times that for other ICUs. The details of the Japanese procedure codes used to define care beds are shown in Additional file 1: Table S1.


留言 (0)