
記住我
Seventeen IDI were held with HCW from participating sites (CBO1 4, CBO2 5, TH1 4, TH2 4). The fifth interview was added at CBO2 in order to reach saturation, as its two clinic locations added additional nuance. Participants came from diverse fields from nursing and midwifery to dental and pharmacy, had a range of 1 to 3 children, and breastfeeding duration of the most recent child ranged from 3 months to 3 years.
Themes from IDI mapped to the conceptual framework as summarized in Table 1; Fig. 2. In the workplace, responsive implementation of workplace policies (Theme 1) was an important facilitator of breastfeeding success, with critical supports differing for different women (Theme 2). The local concept of arr-nar/kreng-jai (Burmese/Thai words for a sense that one is imposing on or bothering others, Theme 3) [33, 34] was prevalent in the workplace environment. Arr-nar/kreng-jai discouraged mothers from taking needed breaks from work to breastfeed or express breastmilk, regardless of official policies and positive relationships with co-workers. When HCW discussed their own breastfeeding outcomes, breastmilk production (Theme 5) and mother-infant bonding (Theme 6) were frequently discussed, both of which were threatened by separation of mother and baby due to work. Personal experience of breastfeeding was universally credited with improved confidence and skills caring for breastfeeding dyads professionally (Theme 7). Family support was essential to breastfeeding success and maternal wellbeing, and was most frequently discussed when support was absent (Theme 8). Culture (Theme 9) was a powerful behind-the-scenes force which participants discussed in the context of patients but not themselves. The practice of giving neonates water was identified as an impediment to exclusive breastfeeding in all local cultures, and Karen/Burman communities were recognized for longer duration and higher prevalence of breastfeeding. Finally, elements of the physical environment (Theme 10)– from rivers to day-care facilities– influenced women’s ability to stay close to their infants. Proximity to their infants was a major determinant of the degree of peace of mind that working mothers experienced.
Table 1 – Summary of qualitative themes with exemplary quotesWorkplace policiesResponsive implementation of policiesWritten policies about breastfeeding or the postpartum period beyond maternity leave were scarce at the CBO facilities (confirmed through IDI, discussions with HR staff, and review of staff handbook when available). Participants described rules that were negotiated and re-negotiated over the years. (Theme 1)
Negotiation at CBO1 often happened on a case-by-case basis, and two out of the four interviewees from CBO1 had special arrangements made by the administration to resolve problems in childcare related to their clinic duties. These women described feeling like the administration cared for them “like family”.
The leaders helped me to move to another department so I am okay now. I really appreciate that. [Laughing] They understand me and look out for mothers who are like me… It is really good for us how our organization helps us… They look after us and think for mother and baby.CBO1.
Negotiation at CBO2 was done at the department level, using meetings and consensus decisions.
There was no rule for when to start night shift after delivery, so we got some complaints from our staff… We called a meeting to decide when breastfeeding mothers should start night shift. We agreed on 5 months.CBO2.
Occasionally, changes were communicated from the central administration, and mothers resorted to informal agreements with their direct supervisors in order to reach their breastfeeding goals.
[HR] came and held a meeting and said, “Staff cannot bring children to the clinic at all.” Aaack. I felt very sad…. What can I do? I want to breastfeed… I said, (whispering) “Doctor, I will go back to breastfeed.” If the doctor allows, I would go back by bicycle quick quick quick and back again… I had to do that for 2 months. I couldn’t do that any longer… What could I do? Her grandmother came. If the baby was hungry she brought her to me and I gave breastfeeding in the back of the room.CBO2.
RTG Hospital employees worked under the same maternity policies but the implementation differed between the two sites. Half of the TH1 interviewees reported obtaining permission for extended maternity leave. In contrast, a TH2 interviewee reported trying to negotiate for additional leave after 3 months and being denied. Others said they did not consider asking for prolonged leave because it was “not done” at TH2.
I could take only 3 months’ leave. Actually I wanted to take leave for 6 months. They told me I could take 6 months’ leave according to the new policy, but my supervisor did not allow me to take leave. My supervisor said there were not enough people.TH2.
These differences in policies and their implementation had a direct effect on breastfeeding outcomes across both RTG and CBO settings. All four staff who were given accommodations to support breastfeeding were able to EBF-6 m and had positive breastfeeding experiences. Neither of the staff who described unsupportive supervisors reached their breastfeeding goals.
Six months maternity leave was suggested by multiple participants to match the period of exclusive breast feeding recommended by the WHO, and multiple staff expressed that night duty was particularly challenging for breastfeeding mothers.
Organizational supportSeveral interviewees described their workplace as supporting breastfeeding, but without practical mechanisms in place to help mothers, this “support” was experienced as pressure:
Yes, the hospital supports breastfeeding a lot. They want the children to get breastmilk… The first few days after I delivered this baby, I didn’t have any breastmilk. The first day, not even one drop of milk came out. It was a challenge for me because my husband started to feel sorry for the child and he wanted to go buy formula for the child. But because I am staff in the hospital the seniors wanted me to be a good example for the other people so I tried. So on the third day I even went to ask for medications to increase the milk production.TH2.
RTG staff suggested that helpful support would include mechanisms to get help for breastfeeding problems and share knowledge between mothers (Theme 2).
The Health Promotion Unit organized trainings on how to feed with breastmilk. I would like to participate when I have the opportunity. There were experiences from the experienced mothers shared to new mothers. We learned from them how to cope with problems.TH1.
CBO staff requests for organizational support focused on safe spaces for children at the clinics, and financial support to offset the burdensome cost of formula for mothers with (perceived or real) low milk production.
Workplace environmentNot wanting to impose: arr-nar/kreng-jaiIn many Southeast Asian cultures, including Burman, Thai and Karen, the concept of imposing on others– arr-nar or kreng-jai– is powerful. Feelings of arr-nar/kreng-jai towards their colleagues were brought up by participants at all the facilities, but were mentioned least at TH1. This manifested as a tension between participants’ physical need to breastfeed or express breastmilk, and cultural pressure not to burden others, particularly supervisors or seniors. Interviewees at TH2 and especially CBO2 described trying to finish their work before going to care for their baby, whereas at CBO1 two mothers described finishing care for their baby first, and then attending to their work (Theme 3).
[At 6 months] I didn’t try to express breast milk anymore. For the past 4 months I felt I had imposed on my colleagues. Now my baby is 6 months and he can eat. I can give formula. Since the baby was little I disturbed my colleagues. I feel I imposed on my colleagues. My colleagues might complain. I feel I took advantage of my colleagues. I don’t want to impose on my colleagues.CBO2.
On busy days I feel kreng-jai and try to finish as much as I can, and then I ask my colleagues if I can finish the rest after I come back. I planned to pump every 3 h but sometimes I couldn’t. I would feel engorgement but it was relieved when I could pump. And when I came home and my baby nursed, it was much better.TH2.
Feelings of arr-nar/kreng-jai contributed to decreased breastfeeding duration and exclusivity by creating an environment where women were uncomfortable taking breaks for breast milk expression, contributing to decreases in breast milk production and decisions to give formula.
HCW personal breastfeeding outcomesBreastmilk productionThe most commonly mentioned breastfeeding problem was perceived or real insufficient breastmilk (both delayed lactogenesis and underproduction of breastmilk, Theme 5). However, other breastfeeding issues such as overproduction, mastitis, rejection of breast after bottle and vice versa, and other special situations such as breastfeeding twins and HIV were also mentioned.
Underproduction of breastmilk was discussed equally between the different sites. Increasing fluid intake was the initial suggestion by most staff at all sites to increase breastmilk production, followed by herbal supplements and frequent breast emptying. RTG staff commonly described using electric breast pumps and more “scientific” explanations of regulation of milk production through hormonal signals. CBO staff did not describe a mechanism by which frequent breast emptying caused increased milk production, but recognized that frequent feeding usually led to adequate milk production. They rarely mentioned electric breast pumps or scheduled expression of breast milk, but described hand expression when direct breastfeeding was not possible, usually when their breasts were already engorged.
The difficulty finding time to empty breasts at work regularly was clearly identified as the reason for decreased milk production, formula supplementation, and early breastfeeding cessation by several RTG staff, whereas CBO staff struggling with low milk production seemed to have no way to explain it.
I could only pump 3 times a day, lunch time, evening time, and night time. Yes, so the milk starts to decrease… I think if I took 6 months of leave and my child always directly breastfeed, I might have milk.TH2.
Sometimes there is just not enough breast milk.CBO2.
Both the RTG and CBO staff expressed that being with the baby continuously and directly breastfeeding frequently would prevent many of the challenges they experienced as working mothers.
For my friends in the village who don’t go to work, they just easily breast feed, just fine. But for my working friends, I think it will be a bit worse, they will all be a bit sad.CBO2.
HCW professional outcomesImproved care for breastfeeding mothersAll the interviewees expressed perceived increased competence caring for breastfeeding dyads after breastfeeding their own babies (Theme 7).
It is helpful because I have a child so I can relate more in detail to them, and I can use my experience to talk to them, compared with someone who doesn’t have children. Those who don’t have children will use whatever they have learned and seen, but since I have a child and I have experience raising a child, I use my experience in addition to what I have learned. And I think it helps a lot.TH2.
However, there was a tendency for those who described less successful breastfeeding experiences to give less appropriate advice. Two CBO mothers who ended up supplementing with formula focused on formula supplementation as the main assistance that their organizations could give breastfeeding dyads who were struggling.
Contextual factorsProximity and peace of mindThe desire of mothers to be close to their infants was mentioned by women from all sites, and women described peace of mind when this was possible (Theme 10).
There were problems, but when I see my baby’s face I feel happy.CBO1.
Elements of the physical space that contributed to women’s experiences included proximity of their home to their work place, availability of physical space to feed their babies or express breast milk at work, and extreme separation from their infants in some cases. Mothers using daycare (at CBO1) or living very close to their workplaces typically described fewer barriers to breastfeeding, especially when proximity was coupled with strong family support.
In the beginning there were the challenges I mentioned before. But I was able to adjust to it… and my home is near my work. In the beginning I forgot the pumping equipment often so I would need to drive home to get it, but my house was not very far from work. It is around 5–6 min if I drive fast.TH2.
CBO2 and TH2 participants talked 3–4 times more frequently than staff at the other sites about a space where they could safely keep and visit their child at the clinic.
If we could have a room it would be more comfortable to bring a nanny. But now we have to use the corner here and there to do it. There is no designated place… a nursing room would be very helpful for us, it would be enough. I do not need anything special. A normal fan would be nice. A room with windows to get sunlight and some fresh air.CBO2.
Two out of the four TH2 participants and one out of the five CBO2 interviewees sent their infants to stay with distant relatives because other solutions to child care were unaffordable or unavailable. In these cases, mothers and infants were separated for weeks or even months at a time, and breastfeeding was invariably terminated.
I had a problem because there was no one to watch my baby. There was nothing I could do, I had to send my daughter to my mother-in-law. My baby was just 6 months old, I felt so sorry for her… I wanted to keep her with me longer, but there was nobody to take care of her… If her own mother can care for her, her mother will feel more at ease. But I cannot– I have to leave her.CBO2.
Survey resultsOverall, 312 eligible participants participated in the survey, representing 78% of participants invited (Additional File 3). As expected, CBO health workers were predominantly born in Myanmar, took the survey in Burmese or Karen, and had their professional training outside the formal Thai system, through NGO, CBO, or Ethnic Health Organization training programs. The RTG staff were almost exclusively born in Thailand, all did the survey in Thai, and received their training through Thai formal health education programs. Baseline characteristics for all participating staff are summarized in Table 2.
Table 2 Baseline characteristics for all survey participants – Data are presented as n (%) unless otherwise indicated. Worksite refers to worksite at the time of the surveyAmong the facilities in this study, breastfeeding rates were highest at CBO1 by all measures, and lowest at TH2. In general, breastfeeding duration and exclusivity was highest in the Burman/Karen culture-dominant CBO clinics, and lower in the Thai culture-dominant RTG Hospitals, but significant variation was apparent within each of these categories (Fig. 3). When work sites were categorized as “high breastfeeding support” (CBO1 and TH1) or “low breastfeeding support” (CBO2 and TH2) based on the qualitative analysis, high breastfeeding support compensated for a lower community breastfeeding prevalence at TH1, resulting in comparable breastfeeding outcomes at 6 months at TH1 and CBO2.
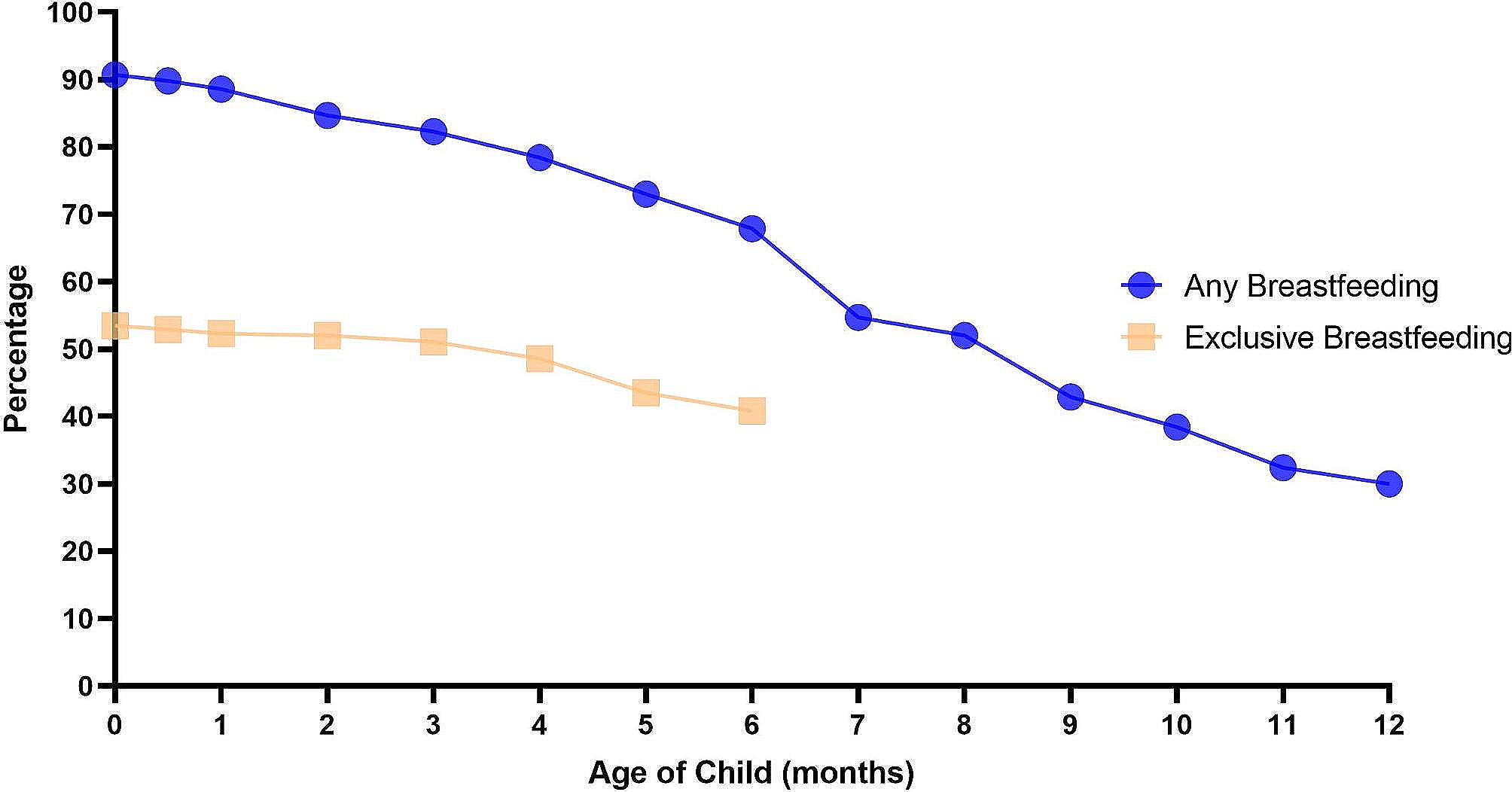
Fig. 3
Survival curves for exclusive (A) and total breastfeeding (B) by site. Exclusive and total breastfeeding duration is visualized by site using Kaplan-Meier curves. Abbreviations: EBF exclusive breastfeeding, CBO community based organization, TH Thai hospital, TBF total breastfeeding
WHO recommended breastfeeding practicesOverall, 53% of mothers who participated in the survey reported EBF-6 m, 31% reported TBF2y, and 21% met both goals. Detailed characteristics and outcomes for mothers are found in Table 3. CBO1 had the highest breastfeeding rates with 46% of CBO1 staff reaching both WHO recommendations.
Table 3 Baseline characteristics and outcomes for mothers – Summary statistics are provided for mothers who completed the survey. Worksite for mothers refers to worksite at the time of birthFactors associated with reaching the WHO recommendations of EBF-6 m and TBF2y are presented in Table 4; Fig. 3. The strongest predictor of EBF-6 m was working at a site with high levels of breastfeeding support: CBO1 (adjusted odds ratio (aOR) 7.3 95%CI 1.8–29.1, p 0.005) or TH1 (aOR 6.3 95%CI 1.8–21.6, p 0.003). EBF-6 m was significantly more common for mothers in the youngest age quartile (< 28 years old, aOR 3.5 95%CI 1.2–9.6, p 0.018), and mothers who set breastfeeding goals (aOR 4.4, 95%CI 1.7–11.5, p 0.002).
Table 4 Characteristics associated with staff meeting WHO exclusive or total breastfeeding goals. The results of univariable and multivariable logistic regression analysis of relationships between work site and personal factors and attaining the WHO exclusive and total breastfeeding recommendations are presentedTBF2y was less strongly associated with identified variables. The aOR of TBF2y was at least 3 times higher for the sites with high breastfeeding prevalence or support compared with TH2 (low breastfeeding prevalence and low support), but this was only significant at CBO1 (high breastfeeding prevalence and high support, aOR 6.3, 95%CI 1.6–24.6, p 0.008). When community breastfeeding prevalence, rather than site, was used in the multivariable analysis, Karen/ Burman community members were twice as likely to breastfeed to 2 years (aOR 2.6, 95%CI 1.0-6.6, p0.054). In addition, mothers were less likely to TBF2y if their reason for stopping breastfeeding was low milk production (aOR 0.2, 95%CI 0.1–0.7, p 0.012) or difficulties continuing breastfeeding while working (aOR 0.3, 95%CI 0.1–0.9, p 0.028).
Meeting both WHO goals (Additional File 4) was associated with working at CBO1 (high breastfeeding prevalence and high support, aOR 8.3, 95%CI 1.4–48.4, p 0.018), setting breastfeeding goals (aOR 5.5, 95%CI 1.1–27.3, p 0.029), and having the most recent child after 2015 (aOR 3.3, 95%CI 1.2–9.5, p 0.030).
Reasons for breastfeeding cessation: work and low milk productionLow milk production (perceived or real) was the most common reason cited for breastfeeding cessation (46/169, 27%, details in Tables 3 and 5) and was strongly associated with a negative experience of breastfeeding (aOR 9.2, 95%CI 1.2–71.9, p 0.034). Stopping breastfeeding due to insufficient milk production was less common among staff working for a CBO: CBO1 (high breastfeeding prevalence and high support, aOR 0.1, 95%CI 0.0-0.5, p 0.005) or CBO2 (high breastfeeding prevalence and low support, aOR 0.2, 95%CI 0.0-0.9, p 0.040).
Table 5 Characteristics associated with attributing the decision to stop breastfeeding to low milk production or difficulties faced breastfeeding while working. The results of univariable and multivariable logistic regression analysis of relationships between work site and personal factors and reasons for cessation of breastfeeding are presentedAlmost a quarter (39/169, 23%) of women reported the reason they stopped breastfeeding was work. (Tables 3 and 5). Multivariable regression found a lower risk of stopping breastfeeding due to work challenges among women who could see their babies during the work day (aOR 0.3, 95%CI 0.1–0.8, p 0.024), or whose most recent baby was born in the most recent year quartile (2018–2021, aOR 0.2, 95%CI 0.0-0.8, p 0.027), and a higher risk for women with two or more children before the most recent baby (aOR 8.3 compared with firstborn, 95%CI 1.4–48.8, p 0.020).
Caring for breastfeeding patientsThe theme of the impact of personal breastfeeding experience on ability to care for breastfeeding dyads was also explored in the surveys through self-reported confidence caring for breastfeeding patients, congruence of advice given to patients about breastfeeding duration with WHO guidelines, and breastfeeding knowledge. Details are found in Table 6 and Additional File 5.
Table 6 Characteristics associated with improved confidence caring for breastfeeding dyads and with giving correct advice about recommended duration of breastfeeding. The results of univariable and multivariable logistic regression analysis of relationships between work site and personal factors and confidence and correct advice when caring for breastfeeding dyads are presentedPersonally meeting both WHO breastfeeding recommendations (aOR 2.6, 95%CI 1.1–6.4 p 0.033) was associated with high confidence in caring for breastfeeding dyads, as were older age (≥ 30 years, aOR 1.9, 95%CI 1.1–3.6, p 0.032), being a nurse or a midwife (either formally or informally trained, aOR 2.6, 95%CI 1.4–4.7, p 0.001), and caring for patients with breastfeeding problems (aOR 3.3, 95%CI 1.6–6.5, p 0.001).
Caring for pregnant or breastfeeding patients (aOR 2.1, 95%CI 1.2–3.7, p 0.001), and higher breastfeeding attitude scores (for the highest quartile compared to the lowest: aOR 2.6, 95%CI 1.2-6.0, p 0.021) were associated with correct breastfeeding duration advice. Notably, TH2 (low breastfeeding prevalence, low support) staff reported the most correct advice, significantly better than TH1 (low breastfeeding prevalence, high support, aOR 0.4 95%CI 0.2–0.8, p 0.009). Overall knowledge scores were low (Additional File 5), with a mean score of 34.7% (sd 15.5, Table 2). Higher scores were associated with formal Thai or Myanmar training (aOR 3.5, 95%CI 1.3–9.6, p 0.013), or working for the more supportive sites: TH1 (aOR 4.1, 95%CI 1.6–10.6, p 0.003) and CBO1 (aOR 3.2, 95%CI 1.0–10.0, p 0.050).
Sensitivity analysis of the impact of non-random sampling in TH1 is included as Additional File 6.
留言 (0)