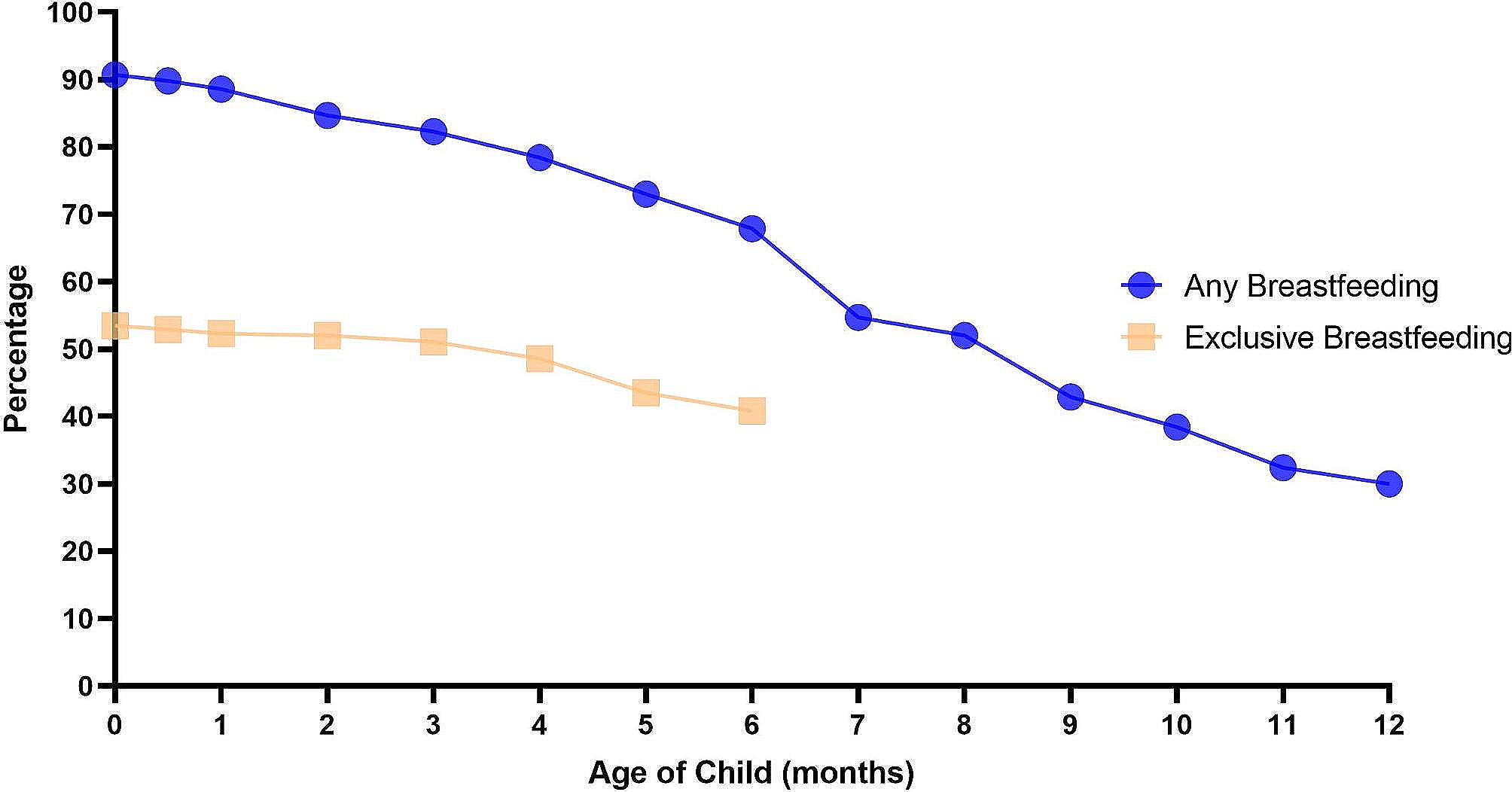
To our knowledge, our study is the first investigation describing breastfeeding in women of childbearing age after undergoing surgery for benign breast disease. In our study, after undergoing surgery for BBD, the rate of ever breastfeeding for this group of patients was 91.0%, which was slightly lower than the national average of 93.7% [12]; the rate of any breastfeeding at 12 months was 30.0%, which was well below the national average of 66.5%. The six-month exclusive breastfeeding rate for these patients was 40.8%, which seems higher than the national average of 29.2% [12] but still below the 50% WHO recommendation. In addition, the first-tier cities are significantly better than the non-first-tier cities in China in many aspects, such as economy, education, health care, and public facilities. However, our investigation found that the mean duration of exclusive breastfeeding for the first child born after surgery was significantly higher in patients living in non-first-tier cities than in those living in first-tier cities (6.07 vs. 4.69 months, P = 0.044). Moreover, the rates of exclusive breastfeeding at six months and any breastfeeding at 12 and 24 months were higher among patients living in non-first-tier cities than among those living in first-tier cities, which was likely due to the higher work pressure.
Many studies have indicated that insufficient breastmilk is the most common reason for stopping breastfeeding [19, 21]. Similarly, our study found that the majority of women who had undergone surgery for benign breast disease reported that their early cessation of breastfeeding was due to insufficient breastmilk, and a small proportion had early cessation of breastfeeding due to underlying diseases, blockage of the milk ducts, work and fatigue. Most of the patients who stopped exclusive breastfeeding within six months stated that it was due to work, followed by insufficient breastmilk, and most of the patients who stopped breastfeeding within 12 months also stopped due to work, followed by insufficient breast milk, and the baby’s refusal to suck. There was no significant difference in the reasons for breastfeeding cessation between patients in first-tier cities and those in non-first-tier cities. Work can affect breastfeeding in several ways. From the line graph of breastfeeding status, we can see that the curve for any breastfeeding declines the most after six months, which may be related to the paid maternity leave system [22]. In the Pearl River Delta region of Guangdong Province, China, the duration of paid maternity leave in most establishments ranges from three to six months, with six months of paid maternity leave being more common, so that patients have enough time for rest and breastfeeding. After the six-month paid maternity leave, busy schedules make many patients choose to stop exclusive breastfeeding or to stop breastfeeding completely. In addition, most of the institutions in China lack special breastfeeding rooms and do not provide special time for breastfeeding, so women who return to work encounter many difficulties if they wish to continue breastfeeding.
Moreover, there are many different brands of infant formula currently available in the community. To pursue profits, businesses produce advertisements, and some of the advertisements go so far as to falsely exaggerate the benefits of infant formula, to profit by deception [19]. Studies have shown that baby food marketing undermines breastfeeding by favourably influencing women’s attitudes and decision-making towards commercial baby food. Women who experienced baby food marketing at health facilities were four times more likely to feed commercial milk formula (CMF) to their children than those who did not experience such marketing [23].
There is a very close interrelationship between breastfeeding and BBDs. In young women, breastfeeding and pregnancy are protective against malignant breast disease but are likely to promote the development of BBD due to hormonal changes [24, 25]. Studies have shown that there is no significant difference in breastfeeding among women with different types of BBDs, but the duration of lactation is significantly correlated with the number of fibroadenomas [5]. The main treatment for benign breast disease is surgery, which can relieve the pressure of the tumour on the milk ducts, but at the same time, surgery may also damage the milk ducts, which may lead to a reduced or inability to breastfeed. There have been a handful of studies exploring the intrinsic relationship between breast surgery and breastfeeding, but no definitive answer has been reached yet [26].
Research has shown that lactation seems to depend on the presence of intact lobules in the breast, intact lactiferous ducts, and an intact nerve supply to the nipple to respond to the sucking reflex [27]. The impact of surgery on breastfeeding depends on the type of intervention and surgical technique [28]. Lactation is altered after either reduction or augmentation breast surgery [14, 26, 29]. In addition, the type of breast incision is significantly associated with lactation outcomes [29]. For cosmetic reasons, the majority of surgical incisions for benign breast disease are now made at the areola margin, which may increase the risk of damaging the nerves around the nipple areola, resulting in altered nipple sensitivity and thus affecting the reflex arc, which is normally stimulated by sucking. It has been shown that periareolar incision and nipple hypoesthesia after surgery are likely to result in diminished lactation [28]. However, techniques that preserve the column of subareolar parenchyma appear to lead to a greater likelihood of breastfeeding [14]. Consequently, the surgical technique, location of the incision, distance between the tumour and nipple, amount of glandular tissue removed and resultant nipple sensitivity have been considered to be important factors influencing lactation [27].
Studies have shown that many women report either not trying to breastfeed or failing to breastfeed after breast surgery. The primary reason for not being able to breastfeed was insufficient milk production, while the main reason for not trying to breastfeed involved psychosocial factors, including personal discouragement, dissuasion by health professionals and occupational demands [30,31,32,33,34]. Our study found that 29% of the enrolled patients reported that they had previously voluntarily reduced the frequency and duration of breastfeeding on the operated breast because of the surgery. Surgery can cause some damage to the structural integrity of the breast, but whether this structural change affects breastfeeding function is not known at this time. However, we can see from the questionnaire that the surgery did have some negative impact on the patients’ psychology regarding breastfeeding. Therefore, we must focus on providing more breastfeeding education to women of childbearing age who have undergone breast surgery, regardless of whether they have undergone surgery for benign breast diseases or malignant tumours, and society and families should also provide more support and encouragement. Next, we will recruit women of childbearing age who have undergone mammary lumpectomy and those who have not, and prospectively observe and analyse the effects of such surgery on breastfeeding and associated risk factors.
Strengths and limitations
The greatest strength of our retrospective survey study is that it is the first to describe breastfeeding in women of childbearing age after BBD surgery and to further analyse the reasons for breastfeeding cessation in this population. Although our study could not prove whether BBD surgery affects breastfeeding function, the survey data showed that the average duration of breastfeeding after surgery for this group of women is not worse than the national average. This could help to reduce concerns about surgery in young women with benign breast disease. Our findings could greatly encourage these patients to breastfeed actively after surgery, reduce their psychosomatic stress, increase their self-confidence in breastfeeding, and prolong the duration of postoperative breastfeeding.
The limitations of our study include the following: first, the number of patients enrolled was not large enough; second, as it was a retrospective study, patients were asked to recall the duration of breastfeeding, so the data may be somewhat biased; third, our study only included patients who underwent surgery for benign breast disease and finally, we did not have access to patient information from other studies, therefore we were not able to add statistics for control variables. Further prospective clinical studies are still needed if we want to investigate whether surgery for benign breast disease affects breastfeeding.

留言 (0)