
記住我



A sequential explanatory mixed-methods study was conducted among a total of 482 female workers (452 for the quantitative part and 30 for the qualitative part) from four RMG factories in the capital city of Bangladesh. In addition, four female physicians (one from each) working in the factories, four (one from each) RMG factory managers, and four local pediatricians from the adjacent areas were included for the qualitative part of the study to get in-depth insight. The study included adult full-time RMG female workers who had at least one child within one year of age and had worked at least the past two years in the factory. A quantitative method was first used to identify the barriers of early initiation of breastfeeding, and a qualitative approach was used to help extract a better understanding of these barriers. We thus choose a sequential explanatory mixed-methods study [35], in which we applied the quantitative approach initially and the qualitative approach thereafter.
Integration of quantitative and qualitative approachWe discovered throughout the quantitative survey that several barriers to early initiation of breastfeeding can be further elaborated with the use of a qualitative approach. Then, to explore these barriers further, we developed a qualitative interview protocol and carried out a qualitative study with mothers who worked in the same RMG industries and shared comparable traits. We also considered the views of the relevant stakeholders, namely, female physicians, RMG factory managers, and local pediatricians from the adjacent areas to get in-depth insight. The same data collectors conducted the interviews.
Through a closed-ended data collection questionnaire, we collected quantitative data about the barriers to the early initiation of breastfeeding. With the data, we could not properly clarify our research question. We discovered some variables, most notably the place of birth delivery, colostrum feeding practices, and RMG facility-based barriers, which in-depth interviews (IDI) with the study participants and key informant interviews (KII) with the pertinent stakeholders could further explore.
Therefore, we developed a qualitative interview protocol based on the findings from the initial quantitative phase. This protocol was designed to delve deeper into the barriers to early initiation of breastfeeding by collecting and analyzing qualitative data in the second phase of the study.
We incorporated the results obtained from both the quantitative and qualitative stages while analysing the overall study findings. As indicated, we asked both quantitative and qualitative research questions to better understand the barriers to the early initiation of breastfeeding. In the result and discussion section, we integrated the findings from both study phases to comprehensively address the research questions and establish a stronger and more significant understanding of the research problem.
Initially, we interpreted the results that helped answer the study’s primary quantitative research question: “What are the barriers to early initiation of breastfeeding among RMG female workers?” Then, we discussed the IDI and KII findings, which were aimed at addressing the main research question in the qualitative stage of the study: “How did the selected factors identified in the quantitative phase affect the early initiation of breastfeeding of the RMG female workers?” This process allowed for the findings from the qualitative phase to further clarify and explain the statistical results from the first quantitative phase. Subsequently, we thoroughly discussed the study results by categorizing the findings into the respective quantitative and qualitative research subquestions that pertain to each of the investigated factors influencing the early initiation of breastfeeding. Finally, we enhanced the discussion by referencing relevant literature, encompassing both quantitative and qualitative published studies. Thus, integrating the quantitative and qualitative findings helped in clarifying the findings of the statistical tests, which underscored the purpose of using a sequential explanatory mixed-methods study design to provide more comprehensive insights.
Sample size calculation and participants selection criteriaSelection of factoriesWe prepared a list of six factories situated in Bangladesh’s capital, Dhaka. Compared to other factories, these factories employed a larger workforce, and a large proportion of the workers were female. In addition, these factories were situated in the heart of the city, which clearly justified the urban poor women included in the title. However, after consulting with the factory managers, two of them did not give us permission due to their busy schedules. We got permission from four factories, and we included them in the study.
For quantitative partThe sample size was drawn by using n = z2 (pq)/d2 formula. Where n is the desired sample size, z is the standard normal deviate (1.96) for a 95% confidence interval, p = estimated proportion (0.66) of outcome variable from the previous study, q = 1-p (0.34), d is the margin of error = 0.05 [24]. After fitting these values in the formula [n = /0.052=0.86/0.0025 = 344.82 ≃ 345}] our calculated sample size was 345. We considered a 10% non-response rate of the participants; therefore, our total sample size turned to 380. The study participants were selected using a multistage sampling method. Firstly, we collected a list of a total of 16,000 workers (both genders) from the four factories. Our study was conducted among women only; therefore, a list of 9503 female workers was constructed. Secondly, 2412 women who had at least one child were short-listed from these women. Finally, the women having a baby under one year of age were considered for the study. Thus, we got a final list of 752 eligible women for our survey. We have included 452 women in this study by using a random sampling technique.
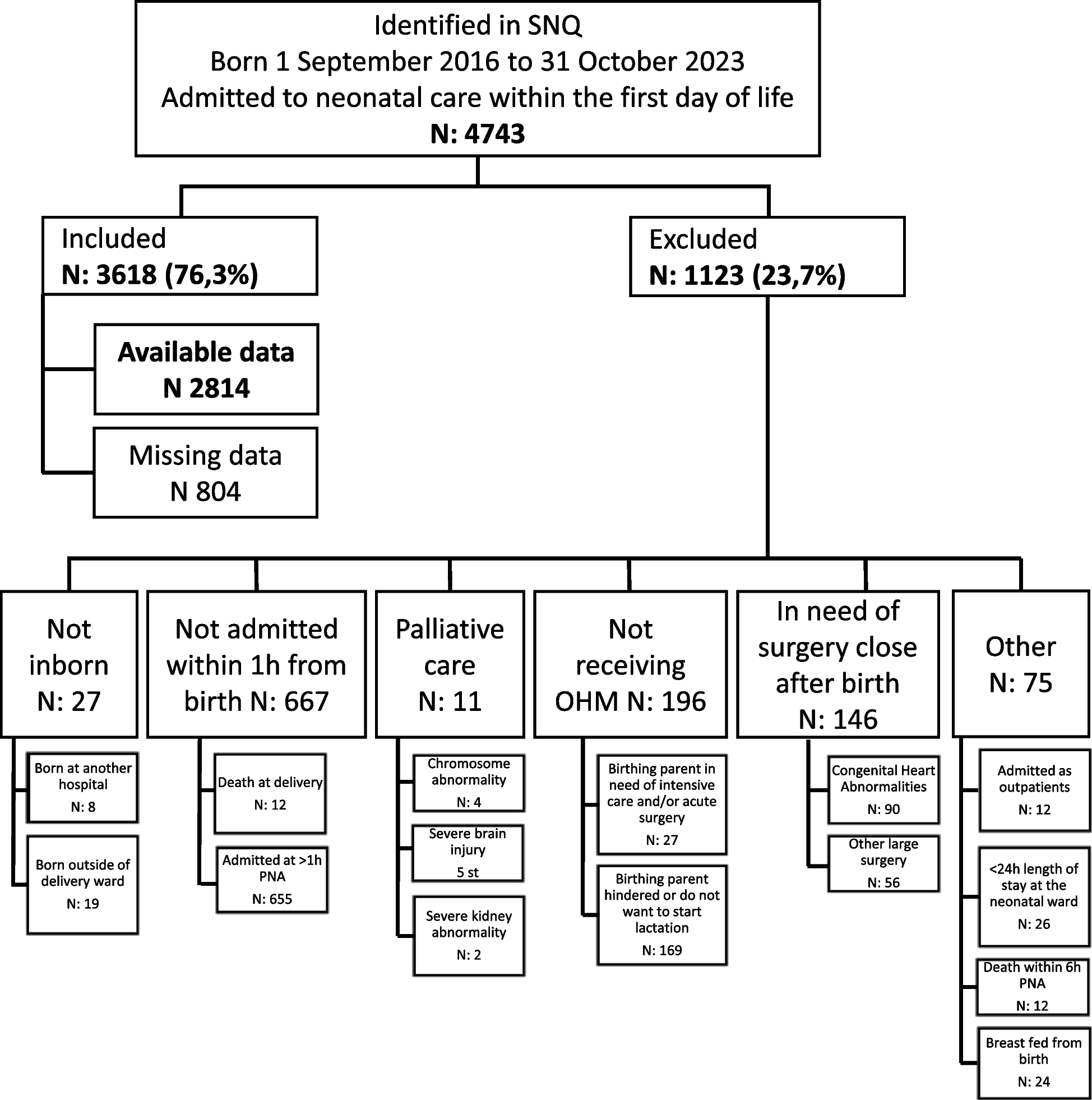
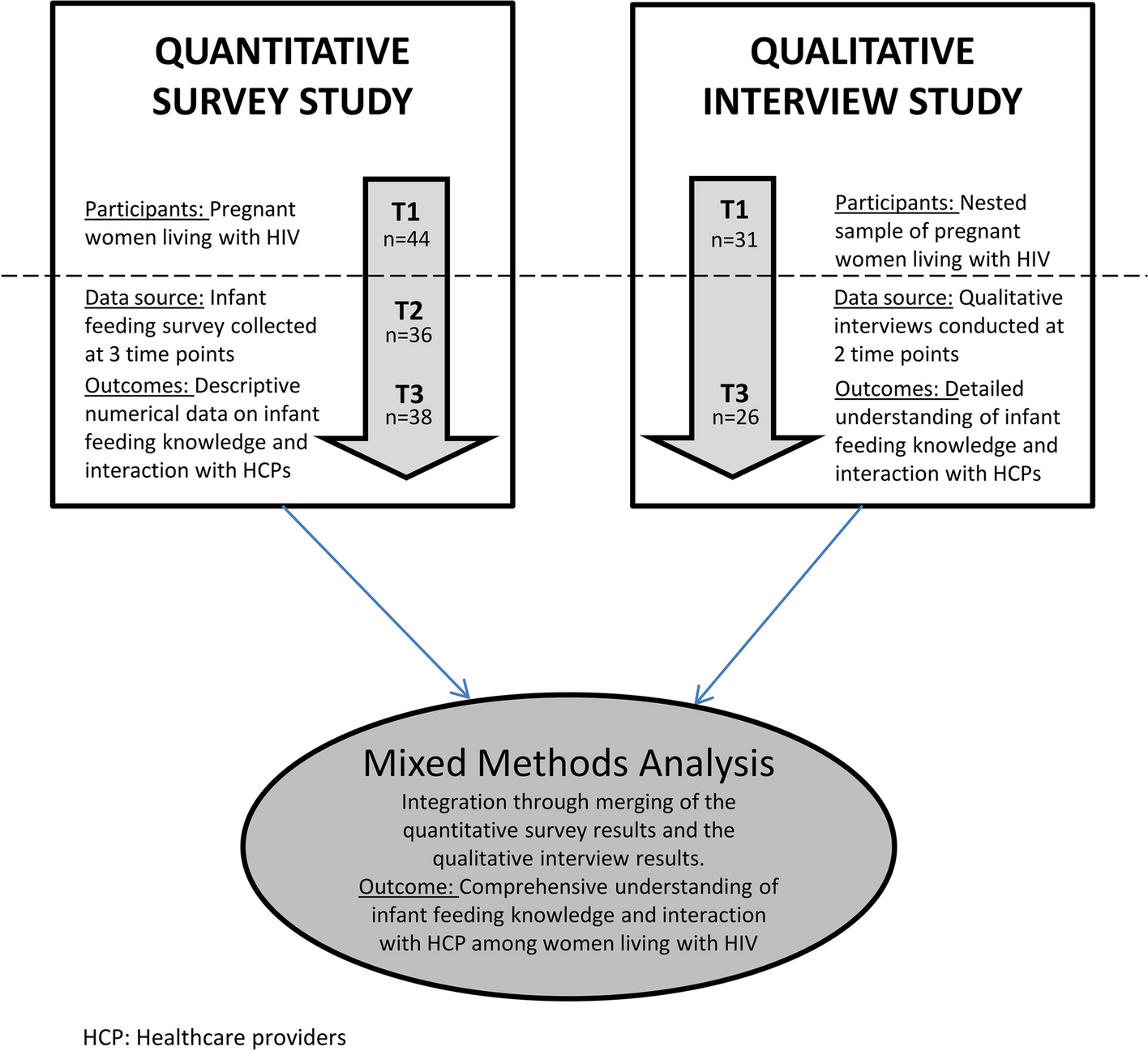
For qualitative partA data saturation point was applied to estimate the sample size for IDI and KII of qualitative investigation. When we found the data had been saturated to a point and almost similar responses were coming from all the respondents, we stopped recruiting new respondents. We finally recruited a total of 30 mothers from four factories. All of them were selected randomly. In addition, we randomly included four female physicians (one from each) who were employed in the factory and were the primary contact point for the health problems of the female workers, four RMG factory managers who directly supervised the female workers to explore the barriers to the failure of early initiation of breastfeeding. Most of the women get their services from local pediatricians, so they know the actual scenario of the issue. Therefore, we also randomly selected four pediatricians from the nearest area to explore the barriers to obtain complete insight (Fig. 1).
Fig. 1
Participant selection for the quantitative and qualitative data collection
Outcome variableThe outcome variable of the study was early initiation of breastfeeding, which was categorized as “≤1 h after birth” or “>1 h after birth”. According to the WHO, when a child is breastfed within one hour of birth, it’s called early initiation; if not done, then it is called late initiation or delayed initiation [36].
Explanatory variablesBased on the literature review from previous studies [24, 37,38,39], Age of the mother (18-25yrs, 26-30yrs, 31-45yrs), religion (Muslim, Hindu), Maternal education (Illiterate, Primary, Secondary or Above), maternal body mass index (Normal, Thin, Overweight or obese), monthly family income in thousand Bangladeshi Taka (10,000–20,000, 21,000–30,000, 30,000 or above), head of the family (Male, Female), ANC visit (No ANC, 1–4 ANC, 4 visits or more), breast feeding counseling during ANC (Yes, No), Age of the infant in month (M) (0 to 2 M, 3 to 4 M, 5 to 6 M), infant’s gender (Male, Female), number of children (1st child, 2nd child, 3rd or over), place of delivery (Home delivery, Facility delivery), mode of delivery (Normal, Cesarean section), pre-lacteal feeding (Yes, No), and colostrum feeding (No, Yes), were considered as the explanatory variables for the study.
Data collection methodQuantitative data collectionData were collected using a semi-structured interviewer-administered questionnaire through a face-to-face interview method. A group of trained data collectors, comprised of three qualified public health specialists and two trained physicians, performed the interviews. There was only one male data collector, and the rest of the data collectors were female because every participant was a woman. The data collectors had three days of training before beginning data collection. Each aspect of potential bias in data collection has been addressed. The same interviewer pre-tested the checklist and data-collection questions to ensure greater understanding. For ease of understanding, the questionnaire was prepared in English and then translated into the local language (Bengali). The interviewers were also trained to avoid asking leading questions to reduce bias. Before the data collection, each participant received information about their autonomy and the objectives of the study. We also trained data collectors on how to build rapport with the RMG women in a friendly manner. Besides we also reassured them that their information would be kept private and anonymous, which encouraged them to be open and truthful. Finally, we trained our data collectors about the cultural sensitivity and privacy of the women. The interview was conducted in Bangla and it was recorded with the permission of the respondents. The data collection tools were validated by both the existing literature and relevant quantitative and qualitative research experts. Before constructing the questionnaire, we did a thorough literature review, from where we set a number of variables to be included in the study. Prior to data collection, we conducted pretesting among 50 RMG mothers with similar characteristics (different from the main study participants). From the pretesting, we edited and corrected the questions and their sequences. Then, we again referred back to test the understandability of the data collection tools and confirmed their reliability.
Qualitative data collectionIDI of 30 RMG workers, KII of four female RMG physicians, four RMG factory managers, and four local pediatricians were conducted in the study. All the IDIs and KIIs data were collected by qualitative interview protocol, and they were recorded using a digital recorder during data collection upon their permission. Written informed consent was collected by the interviewers after describing the objectives and purpose of the study.
Data analysisWe used the statistical software Stata 14 for quantitative data analysis and Microsoft Excel for the qualitative data. Univariate analysis of the variables, including mean, frequency, and percentage, was used as a descriptive statistic. For bivariate analysis, we used the Pearson chi-square test, and the association between the outcome variable and explanatory variables was determined using a binary logistics regression model. For all statistical analyses, a 95% confidence interval (p < 0.05) was considered significant. The recorded qualitative interviews were transcribed in English. Each applicable text unit underwent initial open coding using theme analysis methods by two qualitative researchers who separately generated an Excel spreadsheet containing all of the comments provided by the study participants. The final axial coding scheme, commonly acknowledged as an adequate technique for breaking down core themes, was developed by expanding each theme further in light of the themes that emerged from the comments provided by the participants. By manually classifying the text units into themes and sub-themes, two researchers independently applied the axial codes methodically to the data. A comment was marked as “unclear” if its meaning was not clear to both investigators. Any differences of opinion about the theme analysis were resolved by a discussion between the two researchers and a discussion with two senior researchers. The codes and themes were confirmed and discussed at multiple stages of this procedure, and consensus was reached among the members of the research team. Subsequently, it helped us develop an internally validated codebook, which was implemented to encode the data. Finally, the findings are presented in the text.
留言 (0)