
記住我




Six cases of CC are included, patients with a median age of 16 years (from 14 to 17 years). The disease was predominant in male patients, representing 66% of the cases. The most frequently encountered histological type was mucinous adenocarcinoma, with signet ring cells in 83.3% (Fig. 1), with the remaining cases being well-differentiated adenocarcinoma. The primary site of involvement predominantly affected the descending colon and rectosigmoid junction in 50% of cases, followed by the ascending colon and vermiform appendix in 16.6% each. All patients presented with metastasis at diagnosis. Regional involvement was observed in all patients, including lymph nodes, peritoneal, diaphragm, and transverse colon carcinomatosis. Three patients had liver metastasis, one had bone metastasis, and another had bone marrow metastasis. One patient had metastasis in their small intestine (duodenum and jejunum), while another patient had metastasis on their spleen and pancreas. All were CC metastasis (Table 1) (Fig. 2).
Fig. 1
Histology findings. A A hematoxylin–eosin-stained photomicrograph showing a moderately to poorly differentiated malignant neoplastic lesion of epithelial origin. Cells are arranged in glandular formations and appear as poorly differentiated solitary cells in a solid pattern. B High-power dry magnification reveals loss of cohesiveness in non-glandular neoplastic cells. These cells exhibit enlarged eosinophilic cytoplasm, some containing a single intracytoplasmic vacuole displacing nuclei to the periphery, resulting in hyperchromatic oval and round nuclei with prominent nucleoli resembling a “signet ring” appearance. C The invasion pattern involves infiltrating neoplastic cells into mature adipose tissue with mucin production. This corresponds to a moderately poorly differentiated adenocarcinoma, with some cells displaying a signet ring pattern and reduced cell cohesion within infiltrated tissue
Fig. 2
Endoscopy and surgical tumor findings. A Finding on colonoscopy: inflamed and friable sessile polyp. B The same colonoscopy with other less inflamed and friable sessile polyp. C Inflamed, friable colon mucosa with tumor metastasis. D Surgical finding: tumor in the right colon at the ileocecal valve completely obstructing the Intestinal lumen. E Surgical finding: tumoral metastasis to the third duodenal segment and pancreas already resected. F Laparoscopic finding: tumoral implant at the jejunal level
Patients experienced a gradual onset of symptoms, and it took a median of 29.5 days with a median of 24.5 and a mode of 15 days from the first symptom to their initial hospitalization. Patients were admitted with abdominal pain and marked anemia. Hematochezia was present in 83.3%, and 66.6% reported asthenia, discomfort, fatigue, and weight loss. Palpable abdominal tumors were found in 50% of the patients. Three patients were admitted for the first time with acute abdominal symptoms that were surgically explored on an emergency basis. Fifty percent of the patients were managed with surgery for acute pain, while the rest were approached due to a history of abdominal pain and paresthesia in one case. During their hospital course, 50% progressed to third-space leakage with pleural effusions or ascites. Thiry-four percent of patients had a history of gastrointestinal vomiting, and less frequently, more nonspecific symptoms such as oral intolerance, distant adenopathy, and diarrhea were observed. After a fall, a patient experienced progressive paresthesia in their lower extremities; it was found that the symptoms were due to metastasis of the lumbar vertebrae (Tables 2 and 3).
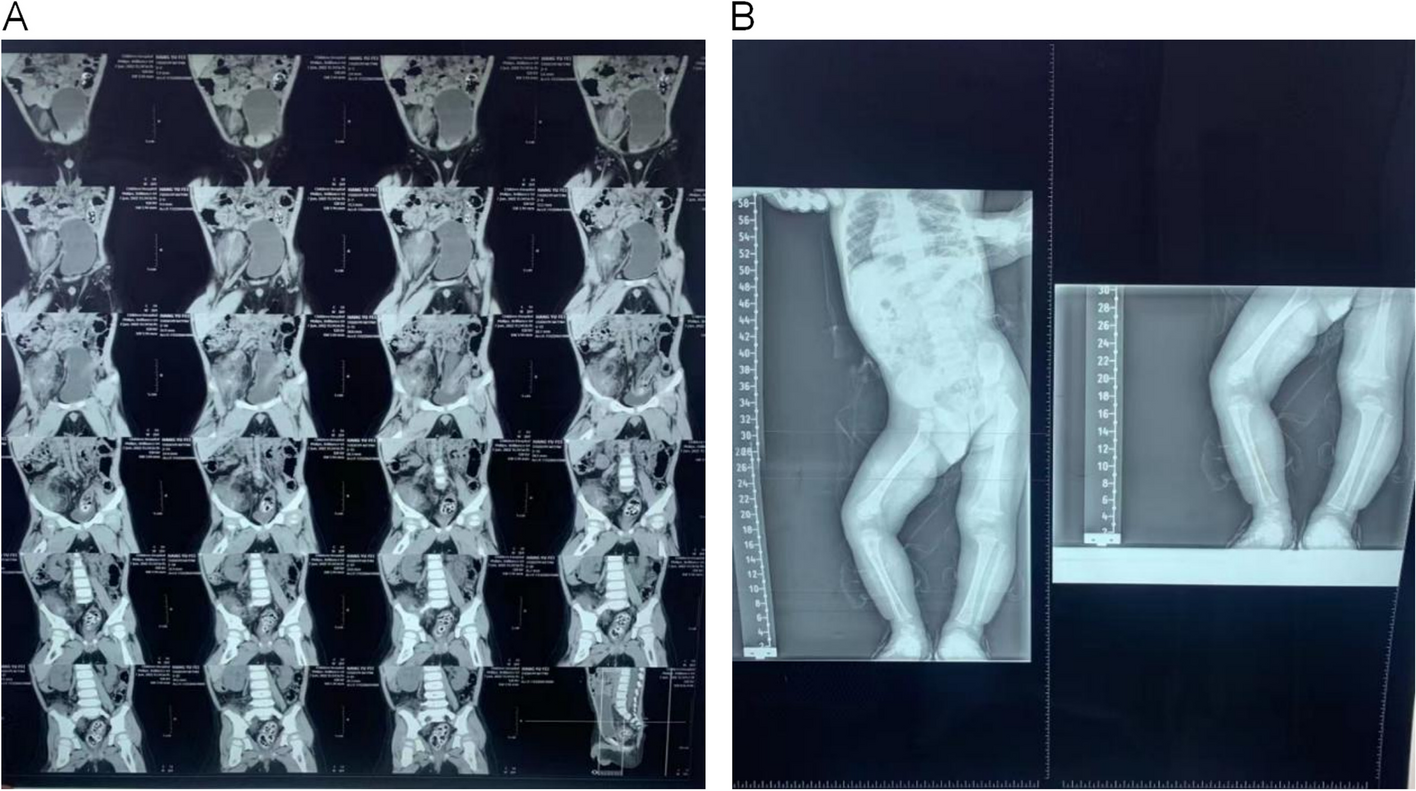
Table 2 General characteristics of the PCC patients, the primary site of affection, metastasis, and treatmentTable 3 Symptomatology and disease progressionAll patients underwent computed tomography to evaluate disease extent, with 50% having a prior abdominal ultrasound and only one patient undergoing magnetic resonance imaging due to symptoms. Four patients underwent endoscopic studies for lesion evaluation and biopsy when they had no abdominal emergency, and an adequate approach was made (Fig. 3). Two patients underwent positron emission computed tomography (PET CT), where primary lesions were visualized. The PET CT was used to identify the primary site of the disease. The use of the radiology modalities was based on the presentation of symptoms, the emergency of each subject, and the evolution.
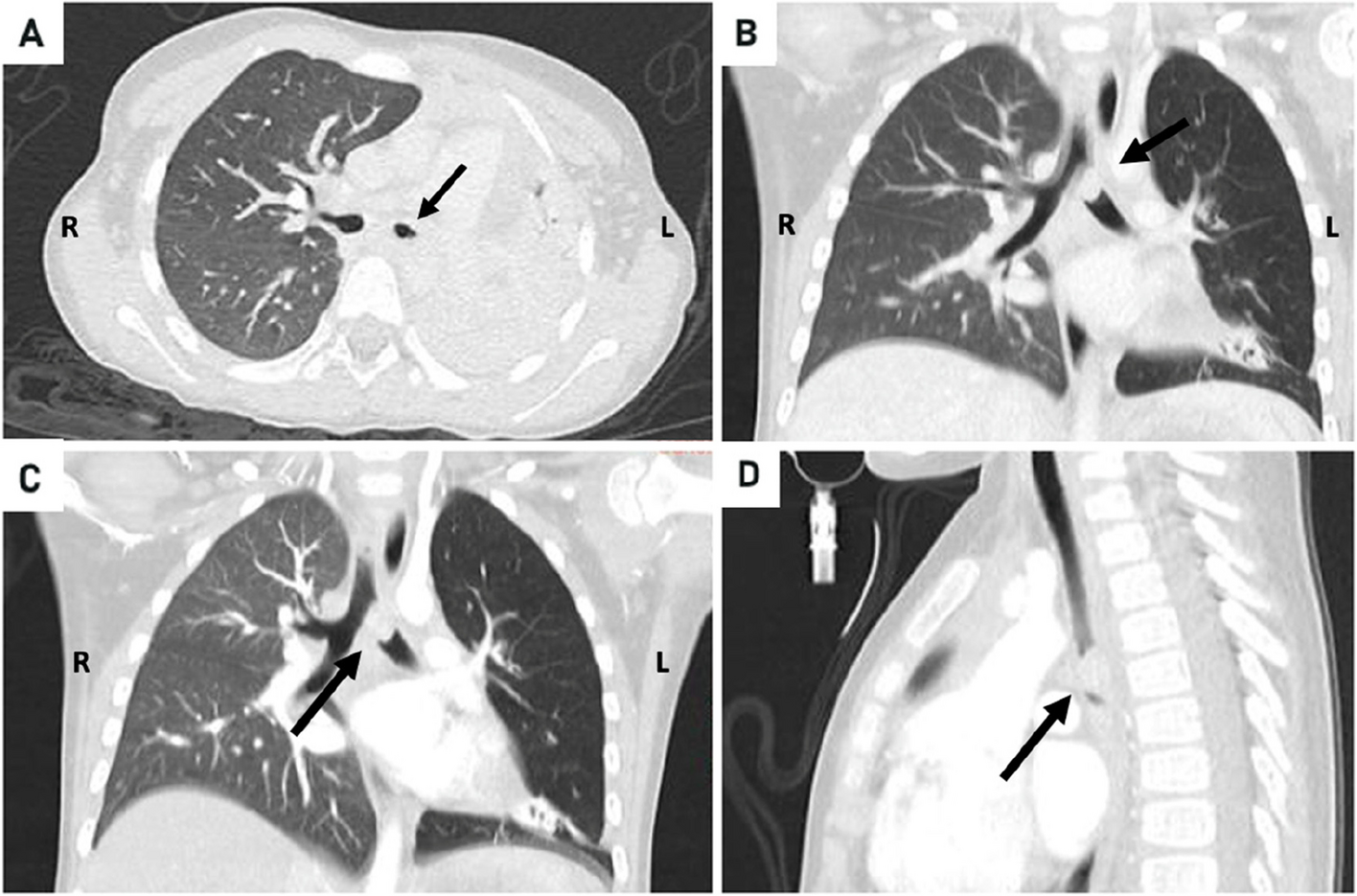
Fig. 3
Imaging findings in pediatric colorectal carcinoma patients. A Abdominal ultrasound of the left colon, demonstrating intestinal wall thickening and luminal occlusion with an isodense lesion with hypodense centers. B Contrast-enhanced chest and abdominal computed tomography showed significant bilateral pleural effusion. C Chest and abdominal computed tomography display thickening of the left colon wall with mural infiltration, accompanied by dilatation of the proximal intestine extending to the stomach. D Abdominal magnetic resonance imaging reveals hypointense lesions with hyperintense capsules in the liver. E Bone scintigraphy shows increased uptake at the site of skeletal metastasis in the lumbar vertebra
Based on the initial presentation of acute abdominal pain, we can differentiate between early and late surgical intervention. When early was a surgical emergency procedure based on the acute abdominal presentation, and late when an adequate approach of the patient could be made.
Two patients underwent laparoscopic procedures for diagnosis, while three were approached by exploratory laparotomy depending on the availability of laparoscopy equipment and the surgeon’s experience. Fifty percent of the patients required surgery: ileostomy, colostomy, hemicolectomy, or appendectomy. Only one patient underwent percutaneous biopsy with a coaxial system. Neoadjuvant and adjuvant chemotherapy was offered to all patients, and only 2 underwent immunomodulatory therapy (Table 1).
It was discovered that two patients had a significant family history of hereditary conditions (Fig. 4). Five patients had passed away, and only one was still receiving palliative care due to the rapid progression of the disease. On a median, patients lived for 10.5 months after diagnosis, with a median of 13 months and a mode of 15 months until death.
Fig. 4
Pedigree of the two patients with a positive family history of cancer
留言 (0)