
記住我



RESEARCH IN CONTEXT
Low incidence of gastrointestinal bleeding and emerging data describing the relationship between stress ulcer prophylaxis (SUP) use and adverse infectious complications have challenged the notion of “routinely” prescribing SUP in pediatric cardiac ICUs (CICUs). We have carried out a pilot study as a first step to examine feasibility and potential safety of a future multicenter study.AT THE BEDSIDE
Our pilot trial randomizing infants in the CICU to placebo or SUP shows feasibility and provides useful data to plan a larger definitive randomized controlled trial. Withholding SUP in this population was not associated with serious adverse events, although its safety needs to be confirmed in a larger trial. A multicenter trial has the potential to significantly change the bedside practice of routine SUP prescription.Stress ulcer prophylaxis (SUP) is commonly prescribed for critically ill patients in the PICU to reduce the risk of stress-related upper gastrointestinal (UGI) bleeding (1,2). The incidence of clinically significant UGI bleeding in the PICU population is very low, and data on the efficacy of SUP are limited (3). Three previous randomized controlled trials (RCTs) have compared SUP vs. no therapy or placebo in a total of 340 children in the PICU (4). In all three RCTs, there was no difference in macroscopic gastrointestinal bleeding between the two groups. In addition to the potential limited benefit, the safety of SUP has been called into question over the last decade (1,5–9). In a large multicenter cohort, we reported a significant association between SUP and ventilator-associated pneumonia in critically ill children (1). Exposure to SUP has been associated with an increased incidence of bacteremia, necrotizing enterocolitis, and mortality in the neonatal ICU population (5,7,8). The undesirable impact of SUP on normal gut microbiota may be a potential mechanism for the infectious outcomes associated with this practice (10). Hence, there is no consensus among pediatric intensivists regarding the clinical indications and role of SUP, and its routine prescription in the PICU is controversial (2,11). However, according to a 2016 survey of Canadian pediatric intensivists, there was “considerable interest” in a placebo-controlled RCT of SUP in critically ill children (12,13).
Critically ill infants with congenital heart disease may be at an increased risk of stress ulcer formation because of mucosal ischemia and reperfusion, use of nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids and vasoactive medications, and prolonged absence of enteral nutrition. Therefore, in this current single-center pilot RCT, we aimed to investigate the feasibility of conducting a clinical trial to assess the safety of withholding SUP in infants with CHD in the cardiac ICU (CICU). Based on the prevalent practice of histamine-2 receptor antagonists (H2RAs) as first-line SUP at our institution, we have designed a pilot RCT to explore differences comparing H2RA vs. placebo. Results of this pilot RCT will guide the development of a multicenter RCT that has the potential to significantly change routine SUP prescription and improve infectious outcomes in this population.
METHODS Study DesignWe conducted a prospective, single-center, double-blinded placebo-controlled pilot RCT to test feasibility of a multicenter RCT. The pilot RCT was carried out in the pediatric CICU at Boston Children’s Hospital (BCH), a quaternary free-standing children’s hospital. The protocol has been previously published (14). The BCH Institutional Review Board (IRB) approved the study, “Stress ulcer prophylaxis versus placebo—a blinded randomized controlled pilot trial to evaluate the safety of two strategies in critically ill infants with congenital heart disease” (IRB-P00028715), on October 18, 2018. All study procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975. The study was registered at ClinicalTrials.gov (NCT03667703) and was funded, in part, by The Gerber Foundation. The funding agency did not have access to data, and was not involved in the design, execution, analysis of the results, or the drafting of this article. An independent, interdisciplinary five-member Data and Safety Monitoring Board (DSMB) conducted reviews of safety data and predicted probability of success during predetermined interim analyses.
Study PopulationWe enrolled infants (age < 12 mo) with anatomic, myopathic, or arrhythmic heart disease, anticipated to require respiratory support (i.e., invasive mechanical ventilation, noninvasive positive pressure ventilation, or high-flow nasal cannula [HFNC]) for greater than 24 hours. We excluded patients with any of the following criteria: 1) received any form of acid suppressive therapy (AST) for greater than 7 days during the month before admission; 2) received more than one dose of AST during the eligible admission; 3) active gastrointestinal bleeding; 4) active Helicobacter pylori infection; 5) anticipated to receive high-dose steroids (i.e., equivalent dosing to 1.5 mg/kg/d of methylprednisolone); 6) scheduled IV NSAIDs like ketorolac, or high-dose aspirin during hospitalization; 7) receiving direct thrombin inhibitors or glycoprotein IIb/IIIa inhibitors; 8) planned or recent history of gastrointestinal surgery; or 9) support by extracorporeal membrane oxygenation (ECMO) or ventricular assist device (VAD).
Recruitment, Study Flow, and RandomizationThe parents or legal guardians of the patients provided written informed consent prior to enrollment and randomization. Potential candidates for study recruitment were identified after screening the daily operative schedule and CICU census. Then, in the preoperative clinic or in the CICU, a principal investigator or a research nurse approached the parents/legal guardians, either in-person or over the telephone, for consent. Families were not approached on the day of surgery. Randomization assignments were generated by SciRan (Boston Children’s Hospital, Boston, MA) using permuted blocks of sizes 2 and 4 to achieve balanced allocation within two strata defined by admission type (medical or surgical) and age (<30 or ≥30 d). The randomization key code was housed in BCH’s investigational drug services pharmacy and concealed from the study investigators. Patients were randomized in a 1:1 ratio to one of two arms; either H2RA (i.e., ranitidine or famotidine per institutional standard) or placebo. Study procedures were continued until whichever occurred first: 1) discontinuation of respiratory support; 2) transfer from the CICU; or 3) 14 days completed on study. The intervention could also be discontinued earlier at the discretion of the patient’s clinicians. All other clinical decisions were left to the medical team treating the child including anticoagulation management, initiation and advancement of enteral nutrition, prescription of intermittent doses of IV NSAIDs, and postoperative antibiotic prophylaxis.
Study InterventionParticipants received the study drug (i.e., an age-appropriate dose of H2RA or placebo) either IV or enterally via the mouth (PO) or the gastric tube (PG), as per the medical team, who decided based on the patient’s clinical status. For ranitidine, neonates (<31 d) received either 1 mg/kg/dose IV/PO/PG every 12 hours and infants (≥31 d) received 1 mg/kg/dose IV every 8 hours or 2 mg/kg/dose PO/PG every 12 hours. Following an initial warning and investigation, the U.S. Food and Drug Administration (FDA) requested all ranitidine products to be removed from the market in April 2020 (15), so ranitidine was removed from the BCH formulary and replaced with famotidine as our preferred H2RA. For famotidine, participants less than 3 months received 0.5 mg/kg/dose IV/PO/PG daily or if greater than or equal to 3 months received 0.25 mg/kg/dose IV every 12 hours or 0.5 mg/kg/dose PO/PG every 12 hours. The placebo to match IV ranitidine/famotidine consisted of an equivalent volume of 0.9% sodium chloride. The placebo to match enteral famotidine and ranitidine consisted of an equivalent volume of a buffered suspending vehicle, Ora-Plus (Perrigo, Dublin, Ireland), and a stevioside sugar-free syrup vehicle, respectively. Patient-specific, blinded syringes were provided at the bedside for the study team. Bedside clinicians, parents/guardians, and outcome assessors remained blinded to the trial allocation. Once a participant completed the study, the clinicians could prescribe acid suppression according to their usual practice.
Outcome VariablesThe major outcomes of interest were feasibility and safety. To be considered feasible, each of the following a priori variables had to be met as follows: 1) greater than 80% of eligible patients were identified (i.e., screening); 2) greater than 20% of eligible patients were randomized (i.e., consent); 3) greater than 80% of consented patients received their first dose of study drug within 48 hours of enrollment (i.e., allocation); and 4) greater than 80% achieved protocol compliance without deviation from assigned group (i.e., protocol adherence). The safety outcome—the rate of clinically significant UGI bleeding—was defined as the presence of new-onset bleeding from the UGI tract (i.e., hematemesis, grossly bloody gastric aspirate, or hematochezia) that was associated with: 1) decrease in hemoglobin by 2 g/dL; or 2) decline in mean arterial blood pressure by 10 mm Hg or initiation/increase of inotrope/vasoactive medications; or 3) increase in heart rate by 20 beats/min in the absence of an arrhythmia or fever; or 4) need for unanticipated blood transfusion; or 5) unexpected endoscopic or operative procedure to achieve hemostasis. This definition has been adapted from prior RCTs in adult patients with excellent inter-rater agreement (16,17). Secondary safety outcomes included: 1) acquisition of a healthcare-associated infections (HAIs), for example, bloodstream infections, catheter-associated urinary tract infections, superficial sternal wound infections, mediastinitis, or ventilator-associated pneumonia; 2) minor gastrointestinal bleeding was defined as stable hemoglobin and vital signs with either blood-tinged gastric output or positive fecal occult blood test; and 3) necrotizing enterocolitis (NEC) or intestinal ischemia.
Sample SizeWe powered the precision of our feasibility estimates for both screening and study drug allocation. We estimated that approximately 1,200 patients older than 12 months would be admitted to the CICU during the study period and that an estimated 200 would be eligible. The target to demonstrate feasibility was screening 80% of all patients. If n = 1,200, the lower limit of the 95% one-sided CI would include 80% as long as the observed screening rate was at least 82.7%. The target to demonstrate feasibility with respect to study drug allocation was to have 80% of randomized patients receive their first dose of study drug within 48 hours. If 100 patients were enrolled, the lower limit of the 95% one-sided CI would include 80% if the observed drug initiation rate was at least 86.9%. This pilot RCT was not powered to assess a statistical difference between the incidence of UGI bleeding and HAIs, as the historical incidences in the BCH CICU are very low, 0.5% and 2%, respectively. These outcomes should be further assessed in a future larger trial.
Data Management and AnalysisData were imported into a secure, password-protected, FDA-compliant (21CRF Part 11) database (using InForm Electronic Data Capture, Oracle, Austin, TX). Data collection included demographic, procedural, laboratory, pharmaceutical, nutritional, ventilator, and outcome variables. The primary analytic approach was according to the intention-to-treat principle. A secondary analysis was performed for safety events based on as-treated groups (placebo or SUP), with exclusion of patients who did not receive either treatment. Categorical variables were summarized as frequencies and percentages. Treatment group comparisons for categorical variables were made with a Fisher exact test. Continuous variables are presented as mean (± sd) or median (IQR). Student t test (parametric) or the Wilcoxon rank-sum test (nonparametric) was used to compare continuous variables by treatment arm. A two-sided p value of less than 0.05 was considered statistically significant. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
RESULTSOver the 3-year study period (February 2019 to March 2022), 1,426 patients aged younger than 12 months were admitted. We screened 1,425 patients (screening rate 99.9%, one-sided 95% CI, 99.7–100%), of whom 132 were eligible for the trial (Fig. 1). The primary reasons for exclusion for the 1,293 patients include: not anticipated to require respiratory support for greater than 24 hours (n = 457, 35%), greater than 7 days of AST exposure in the past month (n = 310, 24%), more than one AST administered during this admission (n = 155, 12%), IV NSAID exposure (n = 126, 9.7%), high-risk anticoagulation exposure (n = 46, 3.6%), and ECMO or VAD utilization (n = 34, 2.6%). Consent was obtained in 70 of 132 eligible patients (consent rate 53%). Reasons for consent not obtained in 47% of the eligible patients are provided in Figure 1. Two patients no longer required CICU admission after consent was obtained and were not randomized. Therefore, 68 patients were randomized (n = 34 SUP, n = 34 placebo) and included in the intention-to-treat analysis. A secondary analysis (n = 65) was performed for safety outcomes, classifying patients as they were actually treated (i.e., as treated), excluding the data of three patients who never received study treatment because they became ineligible after randomization (received platelet inhibitor, n = 2; or received additional antacid dose in parenteral nutrition, n = 1). Seven patients received open-label SUP after randomization (four in placebo and three in the SUP group). Consequently, 58 of 65 randomized patients admitted to the CICU followed the protocol (protocol adherence rate 89.2%, one-sided 95% CI, 80.7–100%). Study drug was administered within 48 hours of enrollment for all patients (allocation 100%).
 Figure 1.:
Figure 1.: Consolidated standards of reporting trials diagram for the trial. H2RA = histamine-2 receptor antagonist.
Figure 2 describes the trial enrollment timeline in relation to the initial projections. In their statement on September 13, 2019, the FDA alerted patients and healthcare professionals of an ongoing investigation into potentially unacceptable levels of N-nitrosodimethylamine in some ranitidine products, and suggested considering alternative treatments (18). The investigators responded with an 8-week pause to amend the protocol and replace ranitidine by famotidine. The following year, the study was paused for 8 months, March 2020 to October 2020, because of the coronavirus disease 2019 (COVID-19) when institutional policies halted all consented studies from being conducted. Despite these hurdles, the trial met all four a priori feasibility metrics, with no treatment group difference in safety outcomes. At their final review in April 2022, the DSMB concluded that the trial’s feasibility outcome measures were met with no serious safety events and recommended trial termination with 68 patients randomized, after 40 of the 48 months of the planned recruitment.
 Figure 2.:
Figure 2.: Trial enrollment timeline. FDA = U.S. Food and Drug Administration.
Table 1 summarizes the baseline characteristics of the treatment groups. They appeared similar, except for weight-for-length z score (median −0.2 vs. −1.3; p = 0.03). Overall, study drug was administered for a median (IQR) of 3 (2–6) days. The safety outcomes are displayed in Table 2. There were no episodes of clinically significant UGI bleeding in either treatment group (0/34 vs. 0/34; treatment difference 0% [95% CI –3 to +3%]). Ten minor safety events were reported, six in the placebo and four in the interventional arm. Five patients experienced minor UGI bleed (n = 3 placebo, n = 2 SUP). All five patients with a minor UGI bleed received open-label AST with resolution of symptoms.
TABLE 1. - Demographic and Key Baseline Characteristics by Treatment Assignment Characteristic n Overall PlaceboCPB = cardiopulmonary bypass, IQR = interquartile range, STAT = The Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery.
Descriptive statistics reported are mean ± sd, median (IQR), and frequency (%).
Table 3 shows the results of the secondary analysis for safety events, based on “as-treated” groups. Three patients experienced an HAI including mediastinitis (n = 1 placebo), tracheitis (n = 1 SUP), and a bloodstream infection (n = 1 SUP). There were no treatment group differences in 28-day mortality (0/34 SUP vs. 1/34 placebo, p = 1.00); median ICU or total hospital length of stay, or the rate of discharge with AST (10/34 SUP vs. 9/34 placebo, p = 1.00) between the groups.
TABLE 3. - Safety Outcomes—As-Treated Analysis Outcome No. of Events No. of Patients Placebo Drug Placebo (n = 28) Drug (n = 37) ExactGI = gastrointestinal.
N = 3 patients excluded due to becoming ineligible after randomization (received glycoprotein IIb/IIIa inhibitor, n = 2; received 2 doses of antacid in parenteral nutrition, n = 1).
N = 7 received open-label antacid.
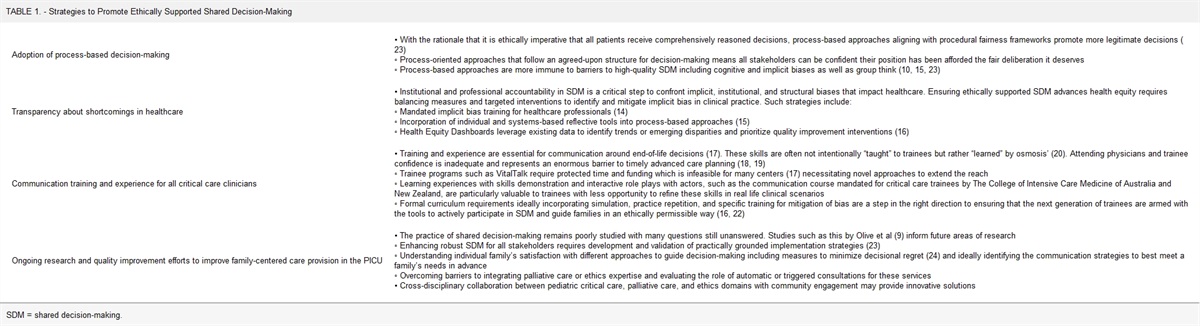
The results of our placebo-controlled pilot RCT confirm the feasibility of conducting a larger trial of withholding SUP in critically ill infants with CHD. We have demonstrated feasibility by meeting all four of our a priori metrics (i.e., screening, consent, allocation, and protocol adherence). We did not observe any serious safety events in our trial. The rates of minor adverse events that could be related to stomach acid or its suppression and secondary outcomes were similar in the treatment groups. The safety of withholding SUP in this population and its benefits for clinical outcomes need to be examined in a larger multicenter trial.
The historical (1986–2015) challenges to completing RCTs in the pediatric critical care population have been well described, with a common reason for failure being early stopping because of futility (19). However, as demonstrated by the national PICU trials network in the United Kingdom, there is an alternative approach which uses a combination of piloting feasibility before definitive RCTs that have led to the delivery of over 10 different multicenter RCTs since 2008 (20). Hence, feasibility of study protocols must be explored in the form of pilot studies before undertaking larger RCTs. To this end, we have demonstrated feasibility. Our screening strategy was successful. The rate of informed consent for the study (53%) was similar to previous Pediatric Heart Network studies’ with consent rates of 43–64% (21,22). Adherence to study protocol met our expected threshold (85% vs. 80%). There was low protocol violation rate in our trial, which attests to the equipoise about SUP use in the CICU population.
The current study provided unique learning opportunities related to enrollment during unanticipated world events. When ranitidine was discontinued due to the FDA recall, we amended the protocol to exchange ranitidine for famotidine, and the trial was restarted after an 8-week pause. During the COVID-19 pandemic, we experienced unprecedented changes to the patient flow and curtailment of nonemergent cases, which may have resulted in the lower than projected (approximately 8.5%) eligibility rate of the study. Our institution’s policies restricted researchers’ and parental presence in the hospital. Protocol amendment to include electronic consenting for nonemergent cases resulted in a modest improvement in enrollment (Fig. 2). Although lower than initially projected, eligibility and enrollment rates remained steady throughout the pandemic with achievement of feasibility metrics and completion, albeit delayed, for the pilot trial. Investigators will need to be prepared for such unanticipated hurdles to trials in the future.
Results of our single-center pilot study may not be generalizable to all institutions. We designed a pragmatic study design—which is well used in PICU trials (20,23)—and based the intervention (H2RAs vs. placebo) on the prevailing SUP practice at our institution. However, proton pump inhibitors (PPIs), either as a first-line or second-line SUP strategy, are frequently employed in adult and other PICUs. A multicenter trial will need to account for these practice variations, particularly the prevalence of PPI usage, in the study design. A three-arm design that includes H2RA, PPI, and placebo might address this issue and may be preferred but will have sample size implications (13). A noninferiority trial might be another design option to examine the strategy of withholding SUP (24). Second, the use of respiratory support for entry criteria may have limited the number of eligible patients. Although it is a strong indicator of severity of illness, current utilization of SUP in the CICU is not limited to those requiring respiratory support. An alternative approach might extend eligibility to a wider patient population, including those without respiratory support. Third, our study was conducted during the global pandemic characterized by unique workflow, personnel constraints, familial stress, and changes to patient characteristics as described above. Hence, the number of eligible patients as well as the consent rate may not be reflective of actual numbers during a routine year. The use of electronic consenting might allow timely enrollment when parents/guardians are not present in the CICU. Finally, our feasibility pilot study was not powered to detect differences in clinically significant UGI bleeds, HAI rates or the incidence of NEC. Thus, we caution changes to current practice until a definitive larger RCT is conducted to examine the safety of withholding SUP and its impact on HAI and other clinical outcomes in critically ill children with CHD.
In conclusion, our pilot feasibility study shows that a multicenter, RCT to determine the safety and potential benefits of withholding SUP in critically ill infants with CHD is warranted. Such a trial would confirm the safety of withholding SUP, its impact on gut microbiota, and its potential for reducing the incidence of HAIs.
ACKNOWLEDGMENTSWe thank the nurses and primary clinicians in the CICU for their support, and the Data Safety and Monitoring Board members for their guidance. We also thank Kerri Ann Fournier from the Institutional Centers for Clinical & Translational Research and Brooke Sens and Samuel Kim from the Pediatric Anesthesia Research Center, Boston Children’s Hospital, for their invaluable assistance with this trial.
REFERENCES 1. Albert BD, Zurakowski D, Bechard LJ, et al.: Enteral nutrition and acid-suppressive therapy in the PICU: Impact on the risk of ventilator-associated pneumonia. Pediatr Crit Care Med. 2016; 17:924–929 2. Duffett M, Chan A, Closs J, et al.: Stress ulcer prophylaxis in critically ill children: A multicenter observational study. Pediatr Crit Care Med. 2020; 21:e107–e113 3. Deerojanawong J, Peongsujarit D, Vivatvakin B, et al.: Incidence and risk factors of upper gastrointestinal bleeding in mechanically ventilated children. Pediatr Crit Care Med. 2009; 10:91–95 4. Reveiz L, Guerrero-Lozano R, Camacho A, et al.: Stress ulcer, gastritis, and gastrointestinal bleeding prophylaxis in critically ill pediatric patients: A systematic review. Pediatr Crit Care Med. 2010; 11:124–132 5. Terrin G, Passariello A, De Curtis M, et al.: Ranitidine is associated with infections, necrotizing enterocolitis, and fatal outcome in newborns. Pediatrics. 2012; 129:e40–e45 6. Selvanderan SP, Summers MJ, Finnis ME, et al.: Pantoprazole or placebo for stress ulcer prophylaxis (POP-UP): Randomized double-blind exploratory study. Crit Care Med. 2016; 44:1842–1850 7. Guillet R, Stoll BJ, Cotten CM, et al.; National Institute of Child Health and Human Development Neonatal Research Network: Association of H2-blocker therapy and higher incidence of necrotizing enterocolitis in very low birth weight infants. Pediatrics. 2006; 117:e137–e142 8. Bianconi S, Gudavalli M, Sutija VG, et al.: Ranitidine and late-onset sepsis in the neonatal intensive care unit. J Perinat Med. 2007; 35:147–150 9. Alhazzani W, Alshamsi F, Belley-Cote E, et al.: Efficacy and safety of stress ulcer prophylaxis in critically ill patients: A network meta-analysis of randomized trials. Intensive Care Med. 2018; 44:1–11 1
留言 (0)