
記住我

This study used a two-stage approach to develop the economic evaluations of the protocols. In the first stage, individual patient data (IPD) from the AVATAR-AF study were used to derive prognostic equations to predict the following outcomes: long-term follow-up rates of ablation, symptom development, symptom recovery and AF-related hospital attendance in addition to health-related quality of life (HRQoL) utilities. In the second stage, the equations were used, where possible, to parameterise a cost-effectiveness economic model considering either a three-way comparison (AVATAR protocol vs. conventional ablation protocol vs. optimised AADs protocol) or a two-way comparison (pooled ablation protocol data vs. optimised AADs protocol).
2.1 Stage One: Statistical Analyses of the AVATAR-AF Trial DataAll outcomes listed above were defined as functions of the treatment arm, and selected additional covariates of potential clinical relevance were used to produce adjusted mean estimates. Generalised linear models (GLMs), with either a Poisson (log link) or Gaussian (identity link) distribution, were used to model all outcomes. The most appropriate distribution for the statistical models was chosen based on the dependent variable type (e.g., count or continuous) and diagnostic criteria (e.g., Akaike’s Information Criteria).
An offset variable was included within the long-term follow-up statistical models to derive a rate per week, rather than an absolute count for each patient, to account for exposure time for the relevant models. In order to meet the requirements of the National Institute for Health and Care Excellence (NICE) reference case [4], EQ-5D-5L data were mapped onto EQ-5D-3L responses to generate utilities prior to any statistical analysis, using the van Hout algorithm [5].
Missing data from patients who were randomised into the trial but withdrew before beginning treatment were removed from the analysis dataset. However, when values of specific variables were missing for a small number of patients (< 5%) who did not withdraw from the study, the missing data were assumed to be missing completely at random, and either a multivariate imputation by chained equations or a last observation carried forward approach was adopted to impute the values. Finally, prior to all statistical analysis, 16 patients were removed from the analysis dataset due to having completed the wrong version of the EQ-5D questionnaire and were hence viewed as protocol deviations. This was done to ensure all HRQoL analyses were performed using information collected using the same instrument and to avoid the inclusion of any biases into the analyses.
All statistical analyses used a 12-week ‘blanking period’ after the initial procedure. This is in accordance with the Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation, which recommends that counting AF recurrences should be avoided within the first 3 months [6]. Despite a subset of patients requiring early re-intervention, events contributing to the outcomes of interest that occurred within the first 3 months were excluded from the reablation rate calculations to align with clinical guidance and the primary manuscript [2]. However, it should be noted that despite excluding early reablations from the long-term rate calculations, the costs associated with additional ablation procedures were captured in the decision tree portion of the economic model.
Two distinct sets of statistical analysis were undertaken. The first considered a three-way comparison (AVATAR protocol vs. conventional ablation protocol vs. optimised AAD protocol). In the event that the three-way comparison showed no significant differences between the AVATAR and conventional ablation protocols, these data would be pooled to increase the statistical power of ablation treatment when compared with optimised AADs in a two-way analysis.
The final selection of variables used for each statistical model were outcome-dependent and were selected via a stepwise deletion process. All GLMs included sex and baseline age as covariates of interest, and the HRQoL GLM also included symptom status as a covariate while adjusting for baseline EQ-5D. No second-order interactions were included in any of the statistical models. All statistical models were two-tailed and significance was defined as p < 0.05.
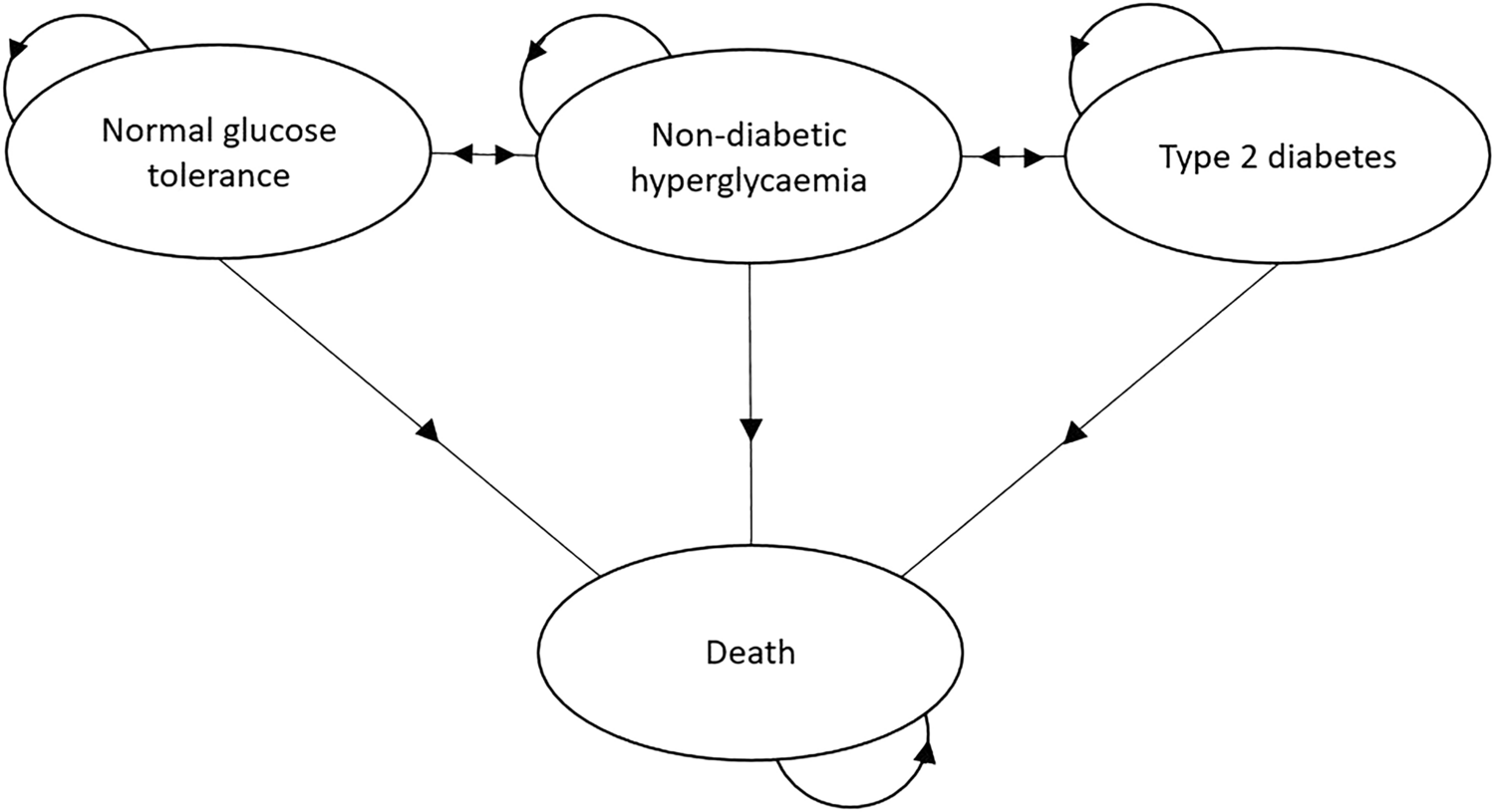
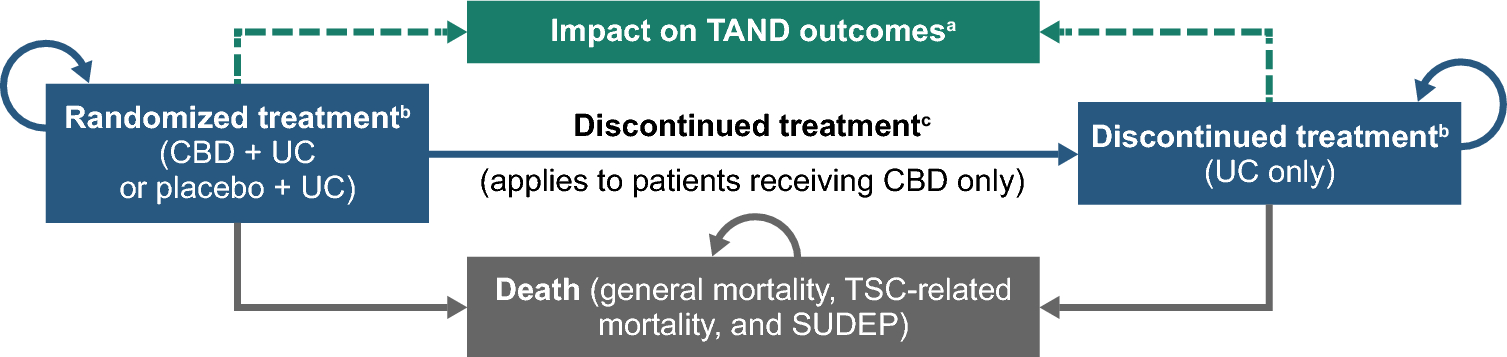
2.2 Stage Two: Description of the Economic Model2.2.1 Model DesignThe cost-effectiveness model was a hybrid of a decision tree with a 1-year time horizon, and a Markov model with a lifetime time horizon (Fig. 1). Costs and benefits were captured in both parts of the model. The endpoint allocation from the decision tree formed the initial state allocation in the Markov model. In line with methodological guidance issued by NICE, a UK National Health Service (NHS) perspective was used, and all benefits were expressed in terms of quality-adjusted life-years (QALYs). In addition to the lifetime time horizon, a cycle length of 3 months was used in the Markov model. This cycle length was chosen to align with the study collection follow-up appointments that occurred every 3 months. All costs and benefits, regardless of which part of the overall model they were derived in, were discounted at 3.5% per annum.
Fig. 1
Schematic of the economic model. (a) Decision tree covering the first 12 months of the economic model. The AAD decision nodes are identical to those presented for AVATAR-AF. (b) Markov model where decision tree endpoints constitute initial allocation. The Markov model covers the remaining lifetime of the economic model. Death is an absorbing state and movement into it is permissible from all other health states. The numbers at the end of each health state indicate the total number of ablations (post initial treatment) in each health state. Patients could have up to a maximum of three total ablations (including the initial procedure). Stroke, heart failure and other adverse events are not modelled as health states but rather as events that can occur to individuals within the health states, and therefore have not been included in the model schematic. AF atrial fibrillation, AAD antiarrhythmic drug, NSR normal sinus rhythm, ST short-term, LT long-term
The patient pathway in the decision tree was captured using three health states: NSR (‘Normal Sinus Rhythm’, defined as no AF episodes recorded within a 3-month period) and Short-Term Episodic AF (‘ST-Episodic’, defined as at least one AF episode [either paroxysmal or persistent] documented within a 3-month period) and death. In the Markov model, two additional health states were included: long-term persistent AF (‘LT-Persistent’, defined as the same symptoms as in the ST Episodic AF health state, but over at least a 12-month duration, that does not resolve on its own), and permanent AF (defined as AF symptoms from which NSR cannot be restored either spontaneously or through treatment).
In addition to AF symptoms, individuals could have a maximum of three ablation procedures (including the original one). For individuals in the optimised AAD arm, the first ablation procedure was classified as the first follow-up ablation within the economic model to allow parity to the ablation arms; however, patients in this arm were still restricted to a maximum of three ablations.
During any cycle in the long-term model, if an individual had an ablation procedure, their ablation count was increased by one, and they could either move back to the NSR health state (but with a higher ablation count) or remain where they were (again with a higher ablation count). In addition, those who received an ablation in a given cycle could move between health states with the same ablation count. As such, the Markov model has 14 distinct health states.
Stroke and heart failure (HF) were included in the model as key AF-related adverse events but were modelled as a proportion of individuals in each health state rather than independent health states. These events were associated with short-term and lifetime costs and HRQoL decrements, which were applied in the first year and all subsequent years respectively (see Table 1). Strokes were stratified by severity (non-disabling, moderately disabling and severely disabling) [7] and HF was captured via the New York Heart Association (NYHA) classification system [8]. Procedure-related adverse events (cardiac tamponade, PV stenosis, vascular complications, and persistent phrenic nerve injury) were also included in the model (using the same method used for stroke and HF). However, as these intraoperative events are typically short-lasting, it was assumed they would only result in additional treatment costs and there would be no impact on a patient’s HRQoL.
Table 1 Key model parameters2.2.2 Model ParameterisationWhere possible, parameters relating to the clinical efficacy of the AVATAR protocol arm were informed either by statistical outputs for the AVATAR protocol arm only or for the pooled ablation protocol data depending on the chosen comparator. Where parameters could not be sourced from the available trial data, inputs were taken from the published literature or derived by interviewing both the clinical co-authors of the study and external clinicians in a group meeting. This included two clinical co-authors who were Cardiologists in England and five external experts who specialised in cardiology and electrophysiology from Canada, Germany, England and the United States. A consensus was achieved by all experts for all inputs based on what was deemed reasonable and conservative given their clinical experience. The structure of the economic model and the definitions used to define each health state were also validated by the same panel of experts to ensure it was reflective of the typical patient pathway.
Table 1 provides information regarding the sources of key non-trial parameters used. Procedure-related equipment costs were supplied by Medtronic or based on publicly available national datasets [9, 10] (see electronic supplementary material [ESM] Table 1).
In order to account for symptom severity and adverse events, disutilities to the baseline utilities were applied to published age- and sex-adjusted population norms [11]. The value for ST-episodic AF was derived from the AVATAR-AF trial data analysis but all other values were derived from the literature [12,13,14,15].
Mortality was captured within the model via a combination of UK general population life tables (excluding stroke- and HF-related deaths) [16] and derived stroke- and HF-related mortality rates. Stroke mortality rates were estimated using published age-specific stroke mortality rates [17] conditional on stroke incident rates. Stroke incidence rates were obtained from trial-specific baseline CHA2DS2-VASc scores and published CHA2DS2-VASc score incidence [18]. NYHA class-specific mortality rates were combined with the HF incident rates [19] and HF-related mortality rates [20].
Where possible, costs in the first year of the model were derived from a protocol-driven within-trial cost analysis (ESM Table 1). Obtained resource use data for ablation procedures, hospital care and pharmaceutical use were extrapolated for the entire time horizon. Costs that could not be sourced from the within-trial analysis (such as those relating to adverse events) were sourced from the published literature and open databases [9, 10, 14, 21, 22]. All costs used in the model were from 2019/2020.
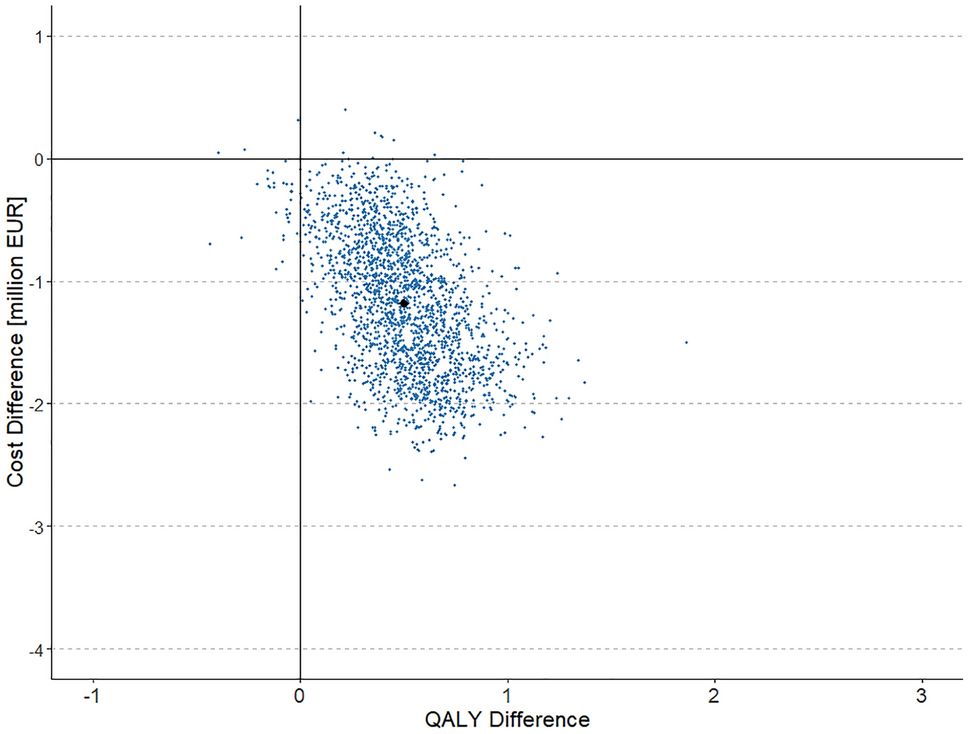
2.2.3 Analysis of UncertaintyUncertainty within the model was explored by conducting a probabilistic sensitivity analysis (PSA) and a series of scenario analyses (e.g., changing the magnitude of the relative risks of state transitions and incidence rates of adverse events). PSA (2500 iterations) was undertaken to estimate the probability of the AVATAR protocol being cost effective compared with the chosen comparator at different cost-effectiveness thresholds (£20,000 and £30,000 per QALY gained as per NICE recommendations) [4]. The scenario analysis involved changing base-case model inputs for inputs obtained from alternative sources, as well as varying inputs derived from clinical expert opinion with reduced or increased magnitudes. Scenarios included varying the values of relative risk of symptom development and recovery (relative to the number of previous ablations or treatment arm), the ablation success rate, and the incidence rate of stroke. The impact of using alternative utility estimation methods (i.e., EQ-5D form replaced by AF Quality of Life Survey form with additional utility decrement for higher European Heart Rhythm Association class) were also explored.
2.2.4 SoftwareRStudio with R 3.6.3 [23] was used for all statistical analyses. The cost-effectiveness model was developed in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA).
2.2.5 Consolidated Health Economic Evaluation Reporting Standards ChecklistA completed Consolidated health Economic Evaluation Reporting Standards (CHEERS) checklist has been reported in the supplementary materials.
留言 (0)