
記住我

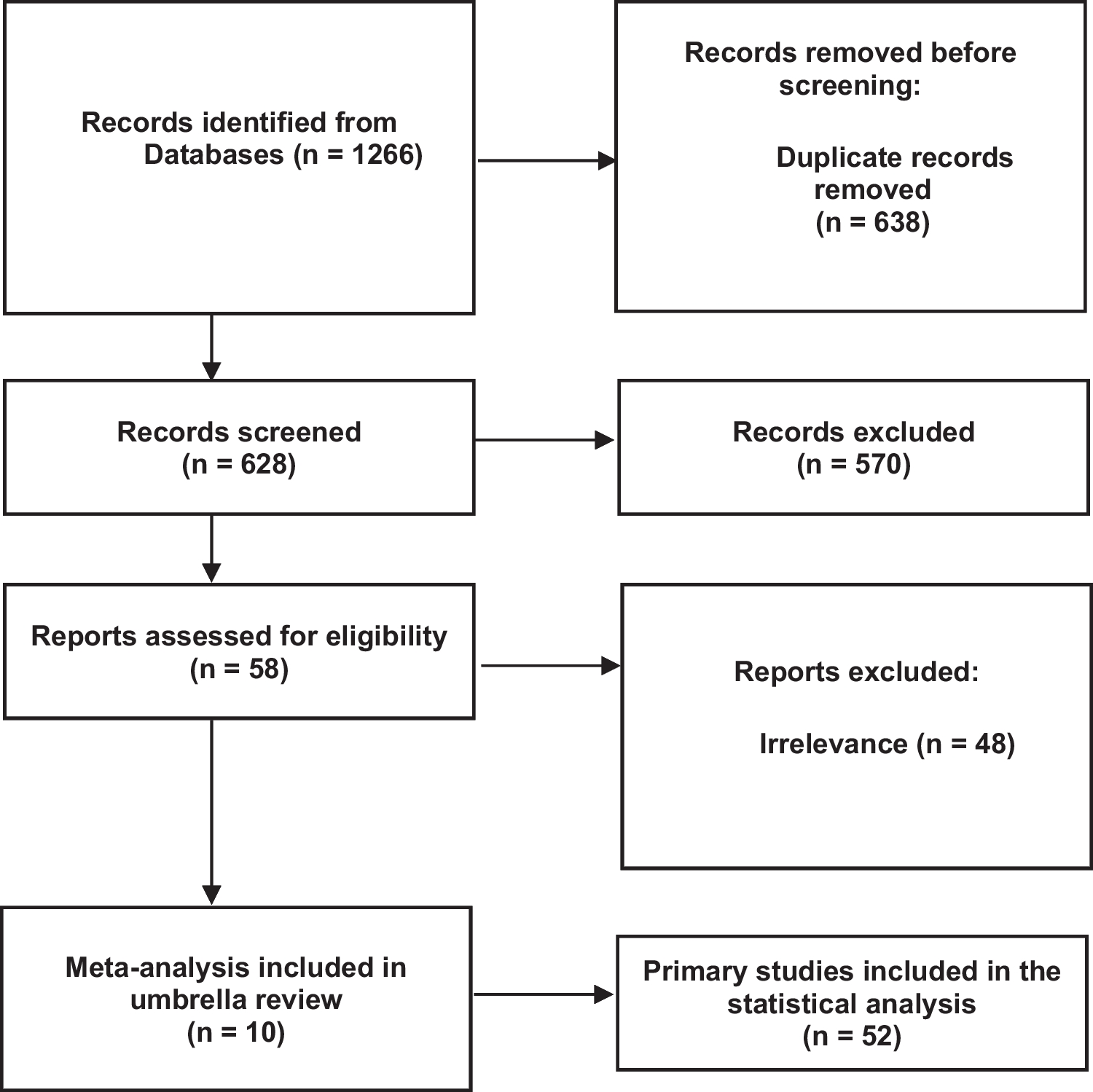
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [7]. A flow chart diagram is displayed in Fig. 1. The present study has also been registered in the Prospective Register of Systematic Reviews (PROSPERO) System (PROSPERO ID: CRD42023438865).
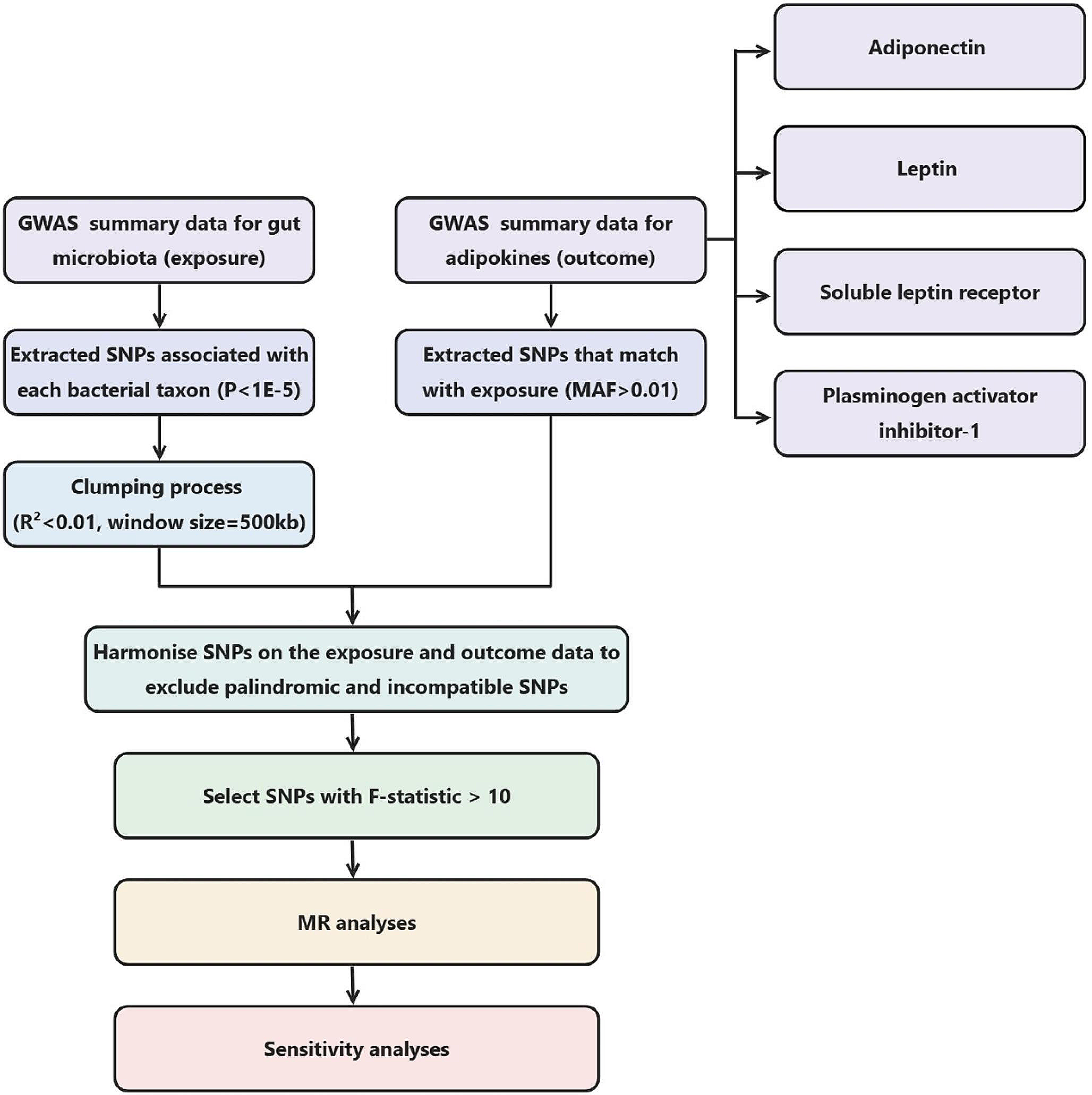
Fig. 1 Search strategy
Search strategyA systematic literature search was conducted from conception until July 31, 2023, in the MEDLINE (PubMed), Scopus, and Cochrane databases to identify eligible studies. The set of relevant terms is presented in Supplementary Table 1.
This study was conducted by the PICO (Population, Intervention or exposure, Comparison, Outcome) model for clinical questions, as follows: (i) Population: postmenopausal women who had received MHT for at least 1 year and had low BMD at baseline (i.e., manifested either as osteopenia or osteoporosis); (ii) Intervention: antiosteoporosis (either antiresorptive or osteoanabolic) therapy administered immediately after discontinuation of MHT; (iii) Comparison group: placebo or calcium plus vitamin D (CaD) or no therapy after MHT withdrawal; and (iv) Outcome: percentage (%) or absolute change in BMD or incidence of new fragility fractures. Grey literature was searched using relevant websites. A manual search was also conducted through citation searching of reviews, which were identified by the above systematic search. The main search was completed independently by two investigators (ED and JKB) who checked all available articles.
Study selectionThe specific inclusion criteria were the following: (i) studies conducted in postmenopausal women (either hysterectomized or non-hysterectomized) who had received MHT for ≥ 1 year and had low BMD at baseline, and (ii) studies providing extractable data on BMD or fragility fractures. RCTs and observational studies published in English were eligible. Only studies with a follow-up time of \(\ge\) 6 months were included. There was no limitation regarding the year of publication, population enrolled, or patients’ age.
Studies were excluded as follows: if they (i) were conducted in patients receiving therapy associated with bone loss, such as aromatase inhibitors or glucocorticoids; (ii) had included patients with metabolic bone diseases (e.g., rheumatoid arthritis or Paget’s disease) or secondary causes of osteoporosis (e.g., primary or secondary hyperparathyroidism, osteomalacia, thyrotoxicosis, Cushing’s syndrome, malabsorption syndrome, diabetes mellitus, rheumatoid arthritis, or genetic causes of osteoporosis); (iii) were written in a non-English language, (iv) were conducted in animals; and (v) were studies not answering the research question.
Data extractionThe following data were extracted and recorded: (i) first author’s name, (ii) year of publication, (iii) study design, (iv) country in which the study was conducted, (v) number and mean [± standard deviation (SD)] age of participants, (vi) duration of MHT, (vii) duration of antiosteoporosis treatment, (viii) BMD before and after antiosteoporosis therapy, and (ix) incidence of fragility fractures during treatment. Parameters, such as mean (± SD) body mass index (BMI), age at menopause, smoking status, alcohol intake, and physical activity, were also recorded where available.
The following comparisons were made: (i) absolute (in g/cm2) or percentage (%) change in BMD in women who received antiosteoporosis therapy after MHT discontinuation compared with those who received placebo, CaD, or no treatment, and (ii) fracture incidence in women who received antiosteoporosis therapy after MHT discontinuation compared with those who received placebo, CaD, or no treatment.
Risk of bias and study quality assessmentRisk of bias assessment for RCTs was carried out using Review Manager (RevMan computer program), version 5.4.2 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014), whereas the Newcastle–Ottawa scale (NOS) was used to assess the quality of observational studies. This scale evaluates studies according to three criteria, as follows: (i) participant selection, (ii) comparability of study groups, and (iii) assessment of outcome or exposure. Each category is assessed based on a four, two, and three-star scale, respectively. A study is characterized as “good quality” when it gets 3–4 stars in the selection domain, 1–2 stars in the comparability domain, and 2–3 stars in the outcome/exposure domain. “Fair quality” is considered to apply when two stars are obtained in the selection domain, 1–2 stars in the comparability domain, and 2–3 stars in the outcome/exposure domain. Finally, a study is characterized as being of “poor quality” in the case of 0–1 stars in the selection domain or 0 stars in the comparability domain or 0–1 stars in the outcome/exposure domain [8].
留言 (0)